




.png)


Why Patient‑Centric Oncology Matters
Patient‑centered oncology transforms the cancer experience by directly linking communication to outcomes. Studies show that clear, empathetic dialogue raises perceived quality of care (OR = 6.2) and trust in physicians (OR = 9.06), while allowing patients to ask all questions boosts trust dramatically (OR = 9.26). When patients feel understood and supported, self‑efficacy rises (OR = 0.56) and adherence to complex regimens improves. Shared decision‑making aligns treatment choices with personal values, cultural beliefs, and life goals, fostering empowerment and satisfaction. By integrating emotional support, transparent information, and collaborative planning, patient‑centric care delivers higher quality, stronger alliances, and more effective, value‑driven oncology for patients and across the cancer continuum.
Principle 1 – Respect for Values, Preferences, and Expressed Needs

Patient‑centered oncology care hinges on honoring what matters most to each individual. The Picker Institute’s eight dimensions of person‑centered care—respect for patients’ values and preferences, clear information and education, coordinated and integrated care, physical comfort, emotional support, involvement of family and friends, continuity and transitions, and easy access to services—provide a practical checklist for clinicians. The Institute of Medicine (IOM) narrows this to six essential dimensions: respect for values, coordinated‑, education information,,,, emotional emotional, involvement emotional friends and—. In practice, these frameworks translate into shared‑decision‑making where a patient’s goals—such as extending life, preserving function, or minimizing side‑effects—directly shape treatment planning. For example, at Hirschfeld Oncology, a pancreatic‑cancer patient’s desire to avoid intensive chemotherapy may lead to a personalized regimen that balances efficacy with quality‑of‑life considerations. By systematically assessing and documenting patient‑reported outcomes, providers can verify that each dimension is being met, fostering trust, higher perceived quality of care, and ultimately better clinical outcomes.
Principle 2 – Coordinated, Multidisciplinary Care

Oncology Medical Home (OMH) standards define a coordinated, patient‑centered model of cancer care that emphasizes accessibility, safety, and evidence‑based treatment. They are organized into seven core domains: patient engagement, availability and access, evidence‑based clinical pathways, comprehensive multidisciplinary team care, quality‑improvement measurement, goals‑of‑care/palliative discussions, and safe administration of antineoplastic therapy. Real‑time clinician access, symptom‑triage systems, and on‑site or expedited supportive services reduce emergency visits and hospitalizations. Multidisciplinary teams incorporate geriatric assessments, survivorship plans, and a just‑culture safety framework, with continuous performance measurement driving value‑based outcomes.
Clinical oncology guidelines such as NCCN and ASCO provide regularly updated, evidence‑based recommendations that standardize diagnostic work‑ups, staging, and treatment sequencing. Hirschfeld Oncology uses these guidelines as the foundation for every patient plan, tailoring therapy to disease biology and patient preferences while integrating innovative trial options and supportive care.
ASCO supportive‑care guidelines prescribe best practices for symptom management (pain, nausea, fatigue, anemia) and psychosocial, nutritional, and palliative interventions. Multidisciplinary panels develop these recommendations, which clinicians can access via ASCO’s AI‑powered Guidelines Assistant, ensuring compassionate, comprehensive care that complements disease‑directed therapies.
Principle 3 – Clear Information, Shared Decision‑Making, and Communication

A narrative review of patient‑centered communication (PCC) identifies six core components that define best‑practice: fostering a therapeutic relationship, gathering comprehensive patient information, providing clear, tailored explanations, engaging in shared decision‑making, responding empathically to emotions, and enabling disease‑ and treatment‑related behaviors. Applying these behaviors in oncology improves recall, adherence, and satisfaction. Structured models such as the Four‑Habits and Calgary‑Cambridge guides operationalize these components: they teach clinicians how to elicit concerns, summarize information, and check patient understanding using the “ask‑tell‑ask” cycle. When combined with patient‑reported outcomes (PROs) and decision aids, these models create a feedback loop that captures symptom burden and preferences, allowing real‑time adjustments to therapy.
Best practice for patient‑centered communication, as outlined in the narrative review, requires deliberate teaching and assessment throughout medical education, with faculty modeling and reinforcement to sustain competence.
Key articles on PCC demonstrate that frameworks like Calgary‑Cambridge and Four‑Habits improve trust and adherence, especially when integrated into multidisciplinary teams such as Hirschfeld Oncology.
Doctor‑patient communication PDFs provide downloadable, evidence‑based guides covering open‑ended questioning, active listening, empathy, and shared decision‑making, ensuring clinicians follow current best‑practice standards.
Aspects of communication that promote person‑centered care include building rapport, active listening, plain‑language explanations, visual aids, empathic responses, and honoring cultural, spiritual, and personal values—each reinforcing trust and empowering patients to partner actively in their cancer journey.
Principle 4 – Physical Comfort, Symptom Management, and Safety

Patient‑centered oncology care places physical comfort and safety at the forefront of every infusion visit. The Oncology Nursing Society (ONS) chemotherapy guidelines serve as the backbone for safe drug delivery. They require a systematic verification of patient identity, diagnosis, drug, dose, route, and timing before each infusion, the use of closed‑system transfer devices or smart pumps with programmed safety checks, continuous vital‑sign monitoring, and prompt recognition of adverse reactions. Documentation of drug name, concentration, rate, and any interruptions must be recorded in the electronic health record, and patients receive education on expected side effects and emergency contacts.
IV chemotherapy administration guidelines echo these standards, mandating a double‑check by a second qualified clinician, aseptic technique for a dedicated IV line, and real‑time monitoring for extravasation or allergic reactions. Laboratory values and vital signs are assessed before, during, and after the infusion, with emergency equipment readily available. Every step is captured in the patient’s record to ensure traceability and compliance with ASCO/ONS safety standards.
Therapeutic communication underpins symptom control and trust. Clinicians should tailor information to each patient’s preferred level of detail, using active listening, validation, and the “five E’s” (establish rapport, explain, educate, empathize, involve family) to foster shared decision‑making. This bidirectional dialogue reduces anxiety, improves adherence, and ultimately enhances quality of life for cancer patients.
Principle 5 – Emotional Support, Trust, and Self‑Efficacy

Patient‑centered communication (PCC) is a proven driver of trust and self‑efficacy in oncology. In a national survey of 1,932 cancer patients, low PCC was linked to dramatically lower odds of perceived quality of care (OR = 0.08, p < .001), trust in doctors (OR = 0.37, p < .001) and self‑efficacy (OR = 0.56, p < .001). Specific PCC practices—explaining next steps (OR = 6.2 for QOC, 9.06 for trust), addressing feelings (2.6, 3.95), clear explanations (4.5, 6.95), spending enough time (10.55, 4.31), helping with uncertainty (18.94, 3.09), and involving patients in decisions (13.35, 2.60)—were strongly associated with higher quality of care and trust. Emotional support, therefore, is not optional; it directly boosts the therapeutic alliance and patients’ confidence to manage their disease. Embedding patient‑reported outcome measures (PROMs) and shared decision‑making tools further empowers patients, leading to better adherence, reduced anxiety, and higher satisfaction. Hirschfeld Oncology exemplifies this model by offering clear, empathetic explanations of precision‑oncology options, allocating ample time for questions, and involving patients and caregivers in every treatment decision, thereby fostering trust, self‑efficacy, and improved overall outcomes.
Principle 6 – Access, Continuity, Innovation, and Future Directions
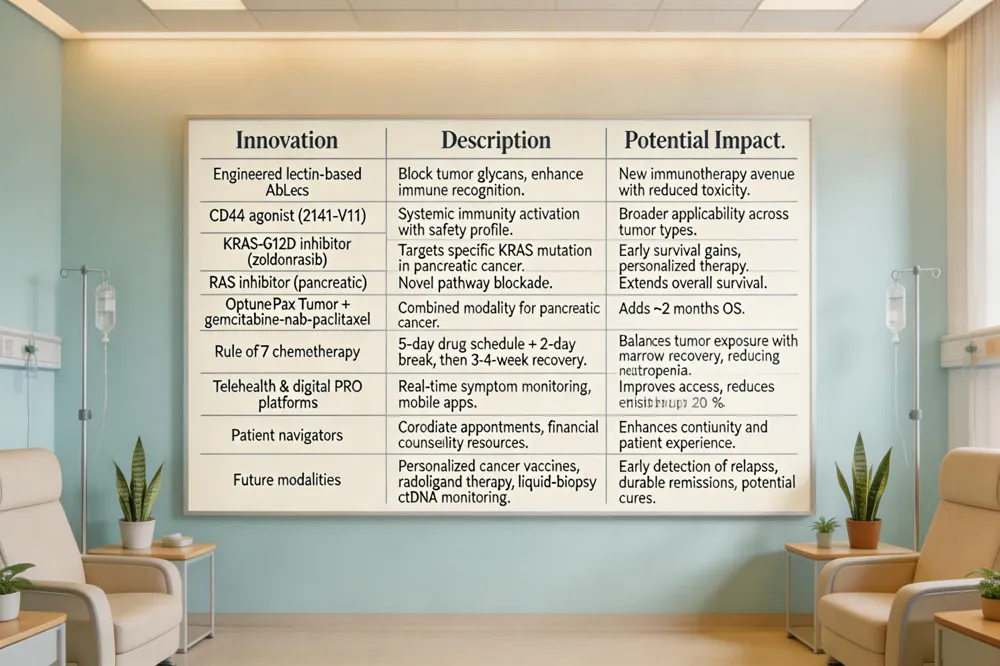
Recent cancer breakthroughs In 2025‑2026 immunotherapy advanced with engineered lectin‑based AbLecs that block tumor glycans and a CD40 agonist (2141‑V11) that triggers systemic immunity while limiting toxicity. Targeted therapy saw the arrival of a novel KRAS‑G12D inhibitor (zoldonrasib) and a new RAS inhibitor for pancreatic cancer showing early survival gains. Pancreatic care also benefited from Optune Pax Tumor combined with gemcitabine‑nab‑paclitaxel, extending overall survival by two months.
Rule of 7 in chemotherapy The “rule of 7” schedules drugs for up to five consecutive days followed by a two‑day break, completing a seven‑day cycle, then a 3‑4‑week recovery period. This pattern balances maximal tumor exposure with bone‑marrow recovery, reducing neutropenia and mucositis.
Telehealth, digital tools, and patient navigation Telehealth expands access, while electronic patient‑reported outcome platforms and mobile symptom apps enable real‑time monitoring. Dedicated patient navigators coordinate appointments, financial counseling, and community resources, decreasing emergency visits by up to 20 %.
Future outlook for cures Although no universal cure exists, precision‑targeted agents such as menin inhibitors for AML and RAS inhibitors for pancreatic cancer are turning many once‑fatal diagnoses into manageable chronic conditions. Personalized cancer vaccines, radioligand therapy, and liquid‑biopsy ctDNA monitoring are further personalizing treatment and early detection of relapse. Continued multidisciplinary collaboration and technology integration promise incremental moves toward durable remissions and, for some cancers, true cure. Ongoing research and policy support will be essential to sustain this momentum for patients worldwide and future generations.
Putting the Principles into Practice at Hirschfeld Oncology
At Hirschfeld Oncology the eight patient‑centric principles are woven into everyday operations. Respect for values is ensured by shared‑decision‑making sessions that capture each patient’s goals before a treatment plan is drafted. Coordination and integration are achieved through a dedicated oncology medical home, where nurses, social workers, and pharmacists meet to align appointments, medication reconciliation, and supportive services. Education is delivered via plain‑language summaries and interactive portals, while physical comfort is addressed by symptom management and pain teams. Emotional support, family involvement, continuity of care, and access are reinforced by a navigation team that arranges transportation, financial counseling, and tele‑health follow‑ups. Multidisciplinary tumor boards, including patient advocates, guarantee evidence‑based, personalized regimens, and the practice adopts therapies such as immunotherapy, targeted agents, and monitoring to stay at forefront of innovation.
.png)
.png)




