




.png)


Setting the Stage: Precision Oncology in GI Cancer
Over the past decade, biomarker testing has become routine in gastrointestinal malignancies, with next‑generation sequencing panels and liquid‑biopsy assays now ordered for most colorectal, gastric, and pancreatic cancers. This expansion has translated into measurable clinical gains: patients matched to KRAS‑wild‑type, BRAF‑V600E, HER2‑amplified, or MSI‑high tumors experience higher response rates, longer progression‑free survival, and reduced exposure to ineffective chemotherapy. At Hirschfeld Oncology, multidisciplinary tumor boards—comprising medical oncologists, pathologists, radiologists, genetic counselors, and research nurses—integrate molecular reports, companion‑diagnostic results, and patient preferences to craft individualized treatment plans and trial enrollment strategies. The collective expertise accelerates turnaround, ensures adherence to NCCN and ASCO testing guidelines, and maximizes the therapeutic benefit of precision oncology for GI cancer patients.
From Bench to Bedside: Core Concepts of Precision Medicine in GI Oncology
 Precision medicine in gastrointestinal (GI) oncology is an individualized approach that uses detailed molecular and genetic information—DNA mutations, RNA expression, protein alterations, and tumor‑microenvironment features—to guide therapy selection. Advanced diagnostics such as next‑generation sequencing (NGS) panels, liquid biopsy (ctDNA), and multiplex imaging generate actionable data, which decision‑support platforms integrate with clinical evidence to recommend the most effective, least toxic regimens.
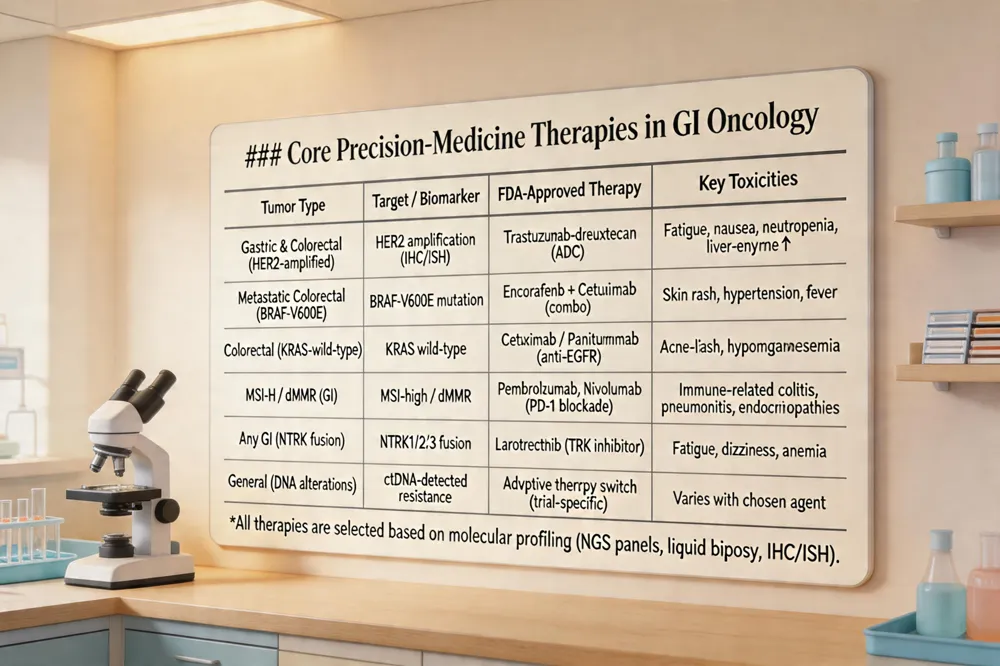
Examples of precision‑medicine therapies across GI tumor types include: HER2‑targeted ADC trastuzumab‑deruxtecan for HER2‑amplified gastric and colorectal cancers; BRAF‑V600E inhibitors (encorafenib) combined with cetuximab for BRAF‑mutated metastatic colorectal cancer; KRAS‑wild‑type anti‑EGFR antibodies (cetuximab, panitumumab) in colorectal cancer; MSI‑high/dMMR immune checkpoint blockade (pembrolizumab, nivolumab) across colorectal, gastric, and pancreatic cancers; and NTRK inhibitors (larotrectinib) for rare NTRK fusions in cholangiocarcinoma or other GI sites.
Biomarker‑driven clinical trials reshape treatment selection by enrolling only patients whose tumors harbor the predictive alteration (enrichment design). Basket, umbrella, and platform trials test multiple agents within a single protocol, accelerating drug development and allowing adaptive changes based on emerging resistance mutations.
Targeted agents typically cause fatigue, skin rash, hypertension, and liver‑enzyme elevations, while immune‑based therapies can trigger immune‑related adverse events such as colitis, pneumonitis, endocrinopathies, and rare severe toxicities. Hematologic toxicities (anemia, neutropenia, thrombocytopenia) also require routine monitoring.
Molecular Landscape of Gastric Cancer: Biomarkers and Emerging Therapies
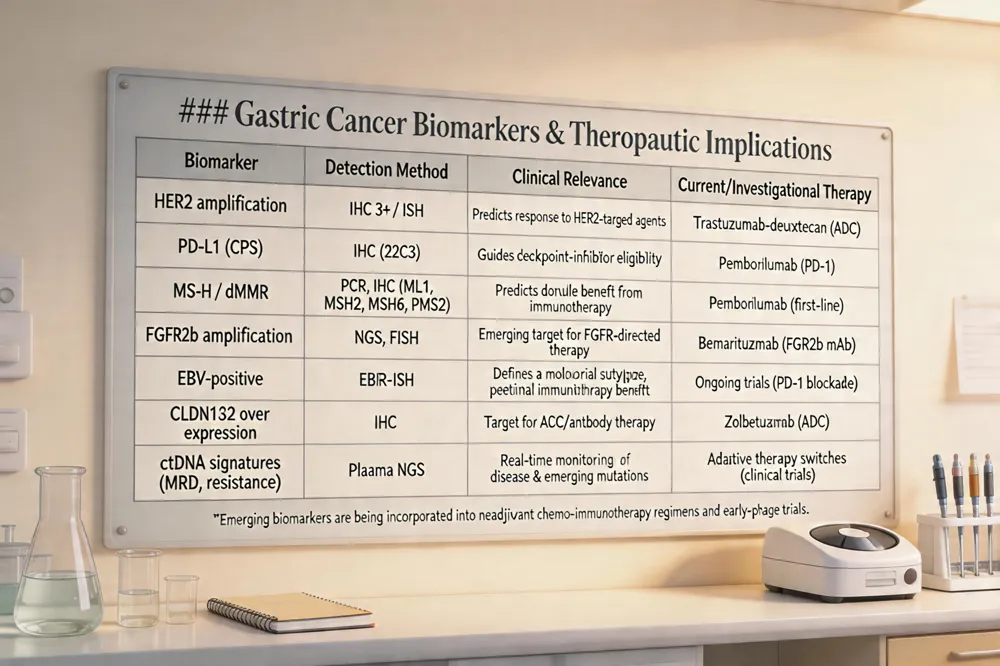 Gastric and gastroesophageal junction (GEJ) cancers are now classified by a set of clinically validated biomarkers that drive therapy selection. Established markers include HER2 amplification—identified by IHC and ISH and predictive of response to trastuzumab‑based regimens—PD‑L1 expression (CPS) that guides checkpoint‑inhibitor use, and microsatellite instability–high (MSI‑H) or mismatch‑repair deficiency (dMMR) which predicts durable benefit from pembrolizumab regardless of tumor site. Emerging targets under investigation comprise FGFR2b amplification, EBV‑positive disease, CLDN18.2 over‑expression, and circulating tumor DNA (ctDNA) signatures that enable real‑time monitoring of minimal residual disease and resistance mutations.
Therapeutic advances are increasingly biomarker‑driven. Neoadjuvant chemo‑immunotherapy (e.g., durvalumab + FLOT) is being explored in resectable disease. HER2‑positive tumors now benefit from trastuzumab‑deruxtecan, an antibody‑drug conjugate with superior response rates. MSI‑H cancers receive first‑line PD‑1 blockade, while ongoing trials assess bispecific antibodies such as zanidatamab and FGFR2b‑targeted agents like bemarituzumab. CLDN18.2‑directed antibody zolbetuximab has demonstrated survival gains in Phase III studies, and CAR‑T approaches targeting gastric antigens are entering early‑phase testing.
Are there biomarkers for gastric cancer? Yes. Clinically validated biomarkers include HER2 amplification, PD‑L1 expression, and MSI‑H. Emerging markers such as FGFR2b amplification, EBV positivity, and ctDNA profiles are being studied to refine prognosis and guide therapy selection.
What are the latest advances in stomach (gastric) cancer treatment? Recent advances comprise neoadjuvant chemo‑immunotherapy, HER2‑targeted trastuzumab‑deruxtecan for HER2‑positive disease, MSI‑guided checkpoint inhibitor therapy, and ongoing trials of antibody‑drug conjugates (e.g., zanidatamab) and CAR‑T cells targeting gastric antigens. FGFR2b‑targeted agents (bemarituzumab) and CLDN18.2‑directed antibodies (zolbetuximab also show promise.
What is the gold‑standard test for diagnosing stomach (stomach) cancer? Upper endoscopy (esophagogastroduodenoscopy, EGD) with biopsy is the gold‑standard. Direct visualization of the gastric mucosa allows targeted sampling, and histopathologic examination confirms cancer type, grade, and molecular characteristics.
Liquid Biopsy, ctDNA, and the Companies Powering Personalized Oncology
 Circulating tumor DNA (ctDNA) has become a cornerstone of gastrointestinal (GI) oncology, enabling non‑invasive detection of minimal residual disease, early recurrence, and emerging resistance mutations after surgery or during therapy. Its rapid turnaround supports adaptive trial designs, allowing clinicians to switch agents when ctDNA‑derived alterations such as KRAS, NRAS, BRAF V600E mutations or HER2 amplification resistance arise.
Clinical‑trial enrichment relies on a set of well‑validated biomarkers: KRAS, NRAS, BRAF V600E mutations; HER2 amplification; microsatellite‑instability‑high (MSI‑H) or mismatch‑repair‑deficient (dMMR) status; PD‑L1 expression; tumor‑mutational burden (TMB); NTRK fusions; FGFR2b alterations; and ctDNA‑identified resistance mutations. These markers stratify patients into basket, umbrella, or platform studies, improving response rates and reducing exposure to ineffective therapies.
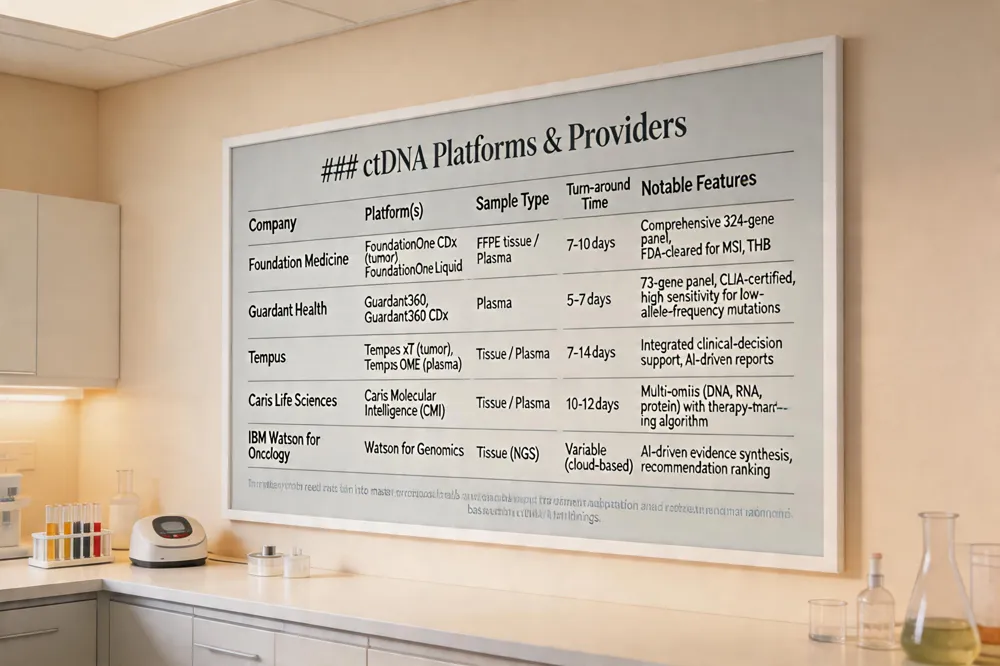
Leading companies delivering comprehensive genomic profiling and personalized cancer‑treatment services include Foundation Medicine (FoundationOne CDx and FoundationOne Liquid), Guardant Health (Guardant360 and Guardant360 CDx), Tempus, Caris Life Sciences, and IBM Watson for Oncology.
Innovative Trial Designs and the Rise of Personalized Cancer Vaccines
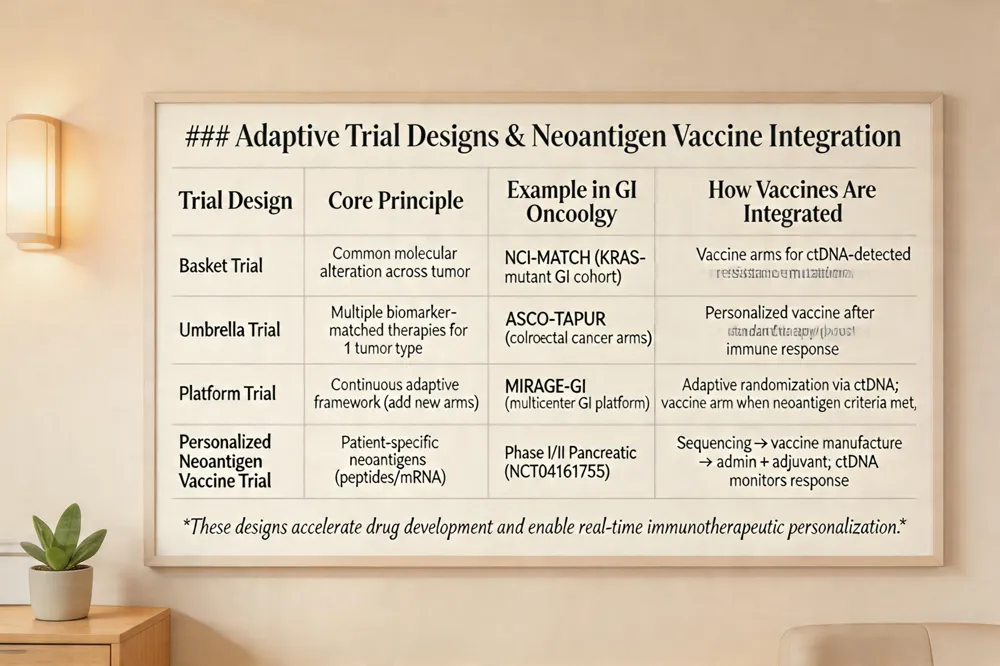 Personalized cancer vaccines are tailor‑made immunotherapies that use a patient’s tumor‑derived neoantigens. Tumor sequencing identifies immunogenic mutant peptides; these are synthesized (as peptides or mRNA) and administered with adjuvants. Dendritic cells present the neoantigens, activating T‑cells that seek and destroy cancer cells bearing the same mutations. Early‑phase GI trials, especially in pancreatic and colorectal cancers, have shown robust immune responses and signals of clinical activity, supporting the integration of neoantigen vaccine arms into adaptive umbrella or platform trials that use circulating tumor DNA (ctDNA) to monitor response and guide subsequent treatment decisions.
Future Outlook: Integrating Biomarkers, Technology, and Multidisciplinary Care
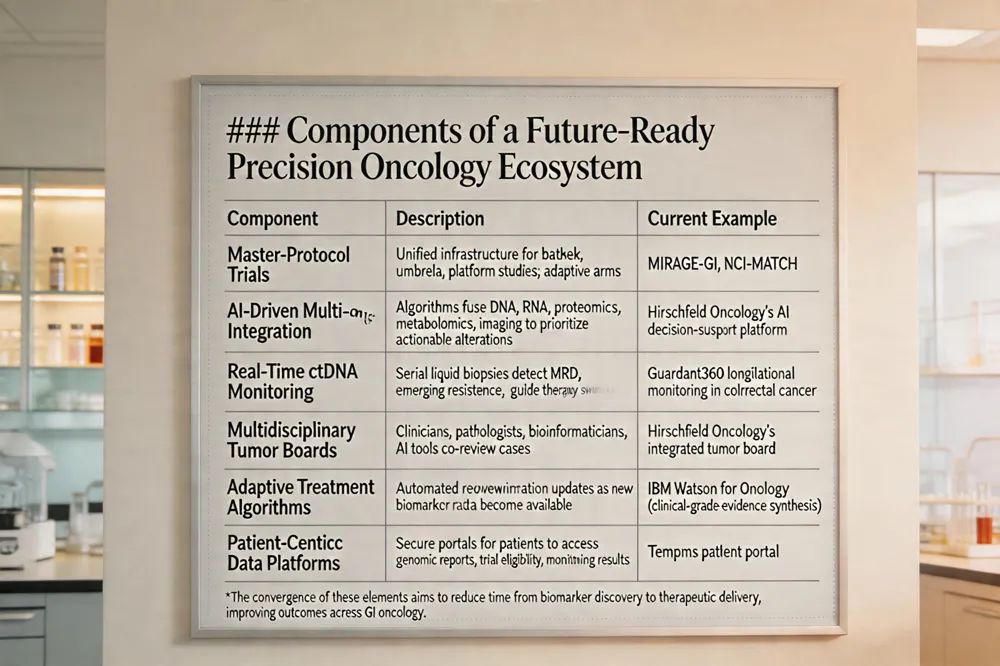 Master‑protocol designs—basket, umbrella, and platform trials—are reshaping GI oncology by allowing multiple biomarker‑defined cohorts to be studied under a single adaptive framework. This consolidates screening, reduces duplicate infrastructure, and shortens enrollment timelines, as demonstrated by the rapid expansion of NCI‑MATCH, ASCO‑TAPUR, and the MIRAGE‑GI platform. At the same time, artificial‑intelligence algorithms that fuse multi‑omics data (genomics, transcriptomics, proteomics, and metabolomics) are becoming integral to patient‑selection pipelines. Predictive models can prioritize the most actionable alterations, forecast resistance pathways, and recommend optimal trial arms in real time, thereby improving match rates and trial efficiency. Hirschfeld Oncology exemplifies this integration: its multidisciplinary tumor board couples comprehensive NGS profiling with AI‑driven decision support, uses rapid ctDNA assays for dynamic monitoring, and enrolls patients into master‑protocol studies across the United States. The result is a seamless, biomarker‑driven care pathway that accelerates access to precision therapies while maintaining rigorous scientific oversight.
Putting Biomarker Science into Practice at Hirschfeld Oncology
At Hirschfeld Oncology every gastrointestinal cancer patient undergoes comprehensive molecular profiling using next‑generation sequencing panels that assess KRAS, NRAS, BRAF, HER2, MSI‑H/dMMR, TMB and emerging alterations such as FGFR2, NTRK and MET. The in‑house laboratory delivers tumor‑informed ctDNA results within two weeks, ensuring that adjuvant therapy decisions—particularly in stage II colorectal cancer—are made before the optimal six‑week window closes, while metastatic cases receive biomarker‑guided first‑line regimens (e.g., anti‑EGFR for KRAS‑wild‑type, encorafenib plus cetuximab for BRAF V600E). Multidisciplinary tumor boards review each profile, integrate data from master‑protocol trials (basket, umbrella, platform) and match patients to active precision studies, thereby translating trial evidence into individualized treatment plans. Real‑time ctDNA surveillance identifies resistance, allowing prompt regimen adjustment to sustain response in patient care continuously.
.png)
.png)




