




.png)


Late at night, after the appointments are over and the house is quiet, many people do the same thing. They start searching. One tab leads to another. A medical term turns into a forum thread, then a video, then a supplement site, and eventually the phrase B17 and cancer appears on the screen.
If that's where you are right now, you're not doing anything wrong. You're trying to help yourself or someone you love. You're trying to find a path that feels less frightening, more hopeful, more in your control.
Cancer pushes people into a world full of hard decisions and conflicting claims. Some websites promise hidden cures. Others dismiss those claims so bluntly that patients feel judged for even asking. Neither approach is helpful when you're scared and trying to make a careful choice.
What helps is a clear answer. B17, also called amygdalin or laetrile, has been studied for cancer for decades. The evidence does not show a proven anticancer benefit in humans, and the main safety concern is cyanide poisoning. Those two facts matter. But the practical question matters just as much. What should you do now, especially if you've already taken it, are thinking about it, or feel unsure how to bring it up with your oncologist?
The Search for Hope in a Cancer Diagnosis
A cancer diagnosis often changes how people think overnight. Someone who never searched for supplements before may suddenly be reading ingredient labels, watching patient testimonials, and asking friends if they've heard of something called B17.
That reaction makes sense. When standard treatment feels overwhelming, or when the disease is advanced or resistant, people want options. They want something that might help without adding more suffering. Families want to feel they haven't missed anything.
Why people look beyond standard treatment
Some people search because they want fewer side effects. Others search because they feel time pressure. Some are trying to make sense of a recommendation they found in an online support group. That search can also lead into other practical topics around treatment, records, and diagnosis language, including resources that explain terms used in cancer documentation such as expert ICD-10 coding for urology.
Patients also often come across clinics or programs that market themselves around hope, alternatives, or last-resort care. If you're sorting through those claims, it can help to compare them with a more grounded discussion of alternative cancer treatment centers and what questions to ask before trusting them.
You don't need to feel embarrassed for asking about an alternative therapy. The safer approach is to ask early, before a supplement creates a problem with treatment or causes harm on its own.
What most patients actually need
Rather than a lecture, what's needed is help separating three different questions:
| Question | Why it matters |
|---|---|
| What is it | Marketing language can hide what a product really contains |
| Does it work | Personal stories aren't the same as clinical evidence |
| Could it hurt me | Even "natural" products can be dangerous during cancer treatment |
That last question is where many online discussions fall short. They may argue about whether B17 works, but they don't help much if you've already bought apricot kernel products, started taking tablets, or mixed them with other foods or supplements. That's where careful, nonjudgmental medical guidance matters most.
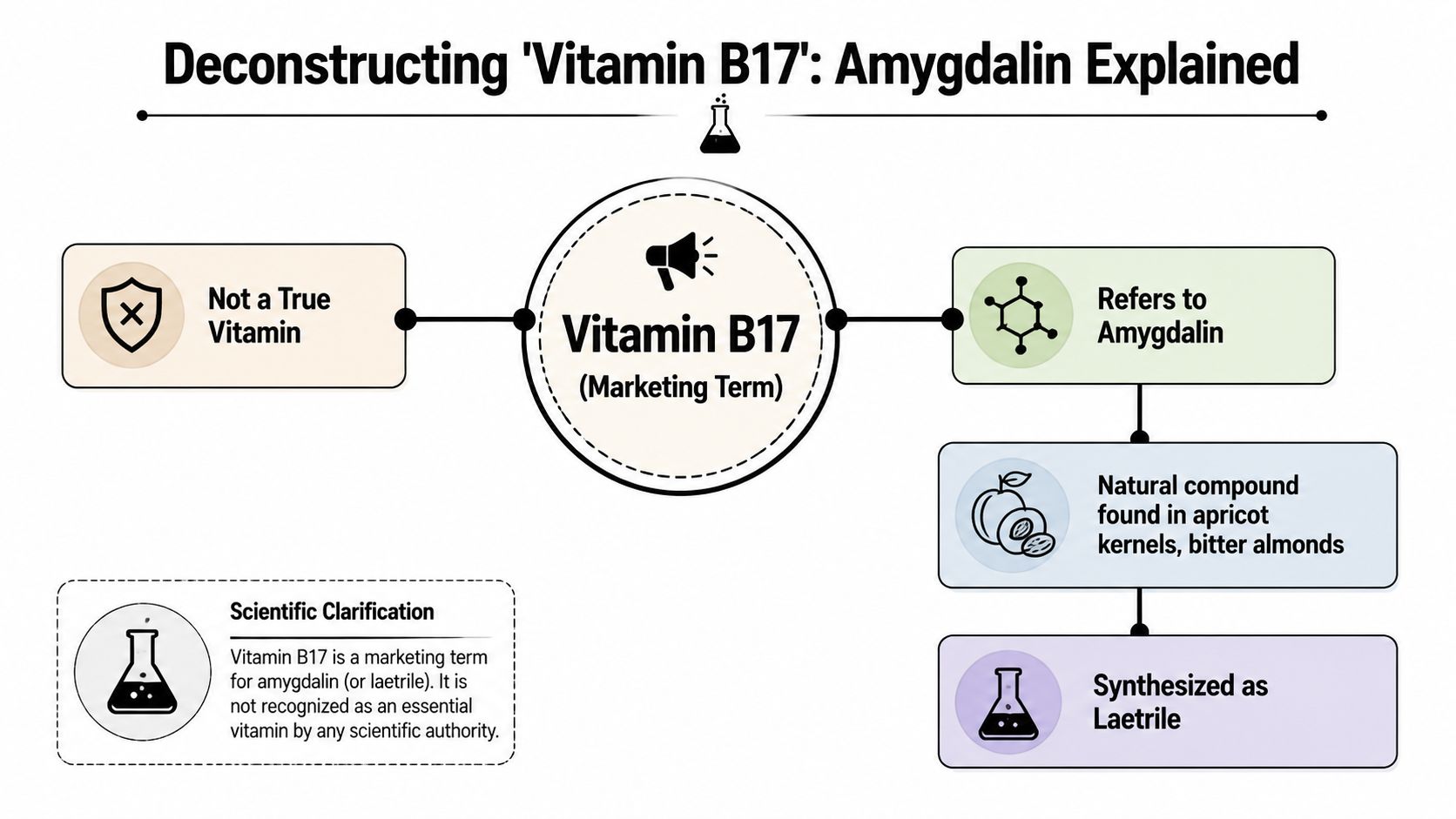
What Exactly Is Vitamin B17
Vitamin B17 isn't a vitamin. That's the first and most important point.
The name is a marketing term used for amygdalin, and for the related product laetrile. A real vitamin is something your body needs for normal function. If you don't get enough of a true vitamin, there is a recognized deficiency problem. Amygdalin doesn't fit that definition.
Why the word vitamin is misleading
Calling amygdalin a vitamin makes it sound familiar and necessary. That's misleading. A review discussing amygdalin notes that the classification of amygdalin as “Vitamin B17” is scientifically invalid because it isn't an essential nutrient and no deficiency syndrome exists. The same review states that the American Society of Clinical Oncology and Cancer Research UK recommend that oncology patients avoid amygdalin entirely, as described in this review of amygdalin and so-called Vitamin B17.
A simple analogy helps. Calling amygdalin a vitamin is like calling cough syrup a fruit juice because it comes in a bottle and is swallowed. The label may sound reassuring, but the category is wrong.
Where people encounter it
People usually hear about B17 in one of these forms:
- Apricot kernel products that are promoted online as natural anticancer support
- Amygdalin supplements sold under wellness language
- Laetrile, a manufactured form associated with alternative cancer marketing
- Food-based advice that blends ordinary plant foods with much stronger supplement claims
That last category creates confusion. Readers may assume that if a compound exists in plants, taking more of it must be safe or beneficial. That isn't how cancer treatment works, and it isn't how toxicology works either.
If you're interested in how supplements and plant-derived compounds are discussed more broadly in oncology care, this overview of nutraceuticals and their role in patient-centric cancer care gives useful context.
Practical rule: Before you take any product marketed for cancer, ask two plain questions. What is the actual chemical substance, and is it an essential nutrient or just being sold with nutrition language?
The History and Theory Behind B17
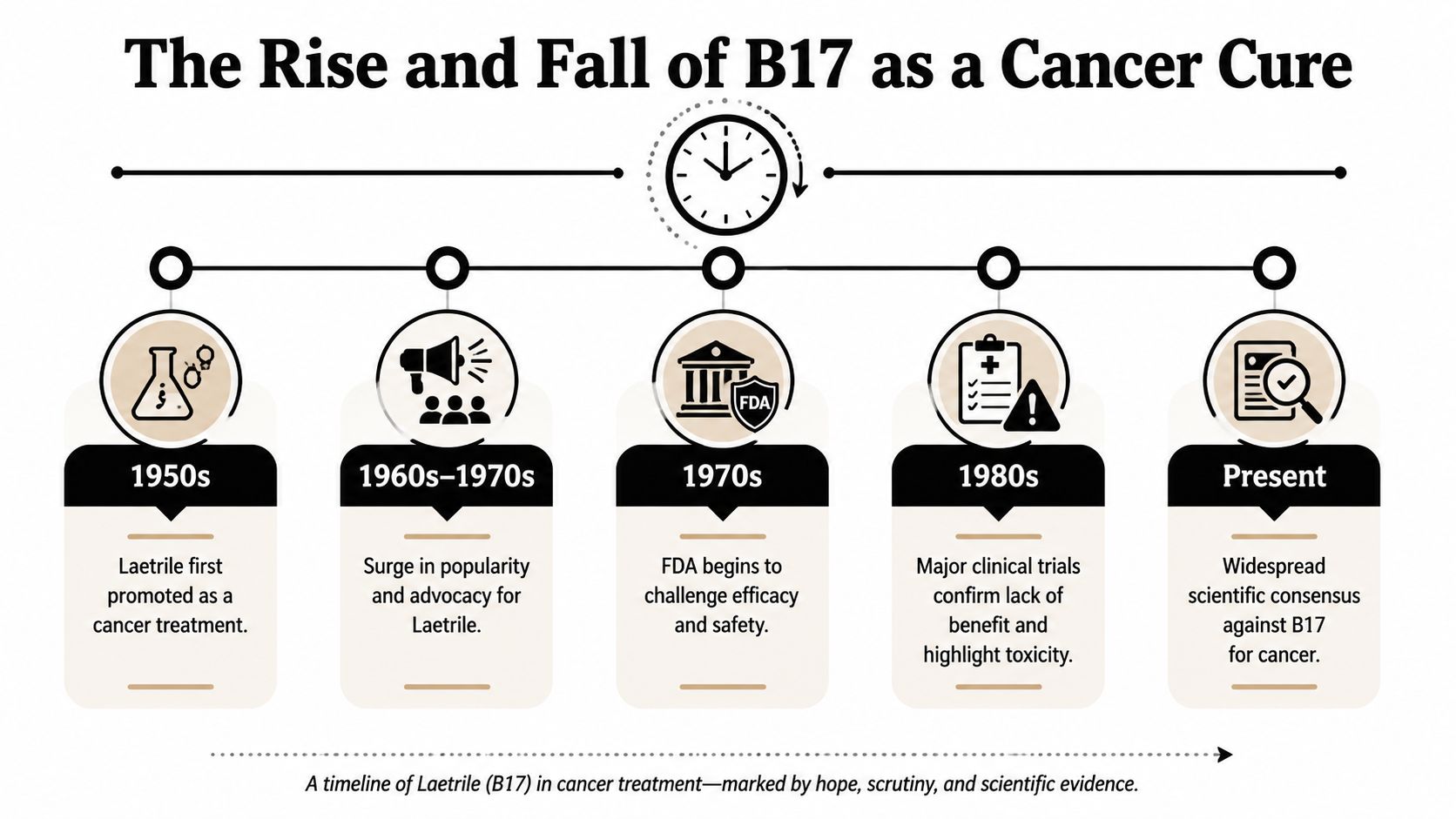
A cancer diagnosis often changes how people weigh risk. Treatments that once sounded questionable can start to sound reasonable if they promise selectivity, gentleness, or a path outside standard care. That is part of how laetrile remained in public discussion for decades, beginning in the mid-20th century and later drawing formal attention from the National Cancer Institute overview of laetrile.
History matters here, but not in the way marketing suggests. An old idea is not the same as a proven one. Some claims stay alive because they are repeated from person to person, repackaged online, and attached to understandable hope.
Why the theory appealed to patients
The central promise was emotionally powerful. Supporters claimed laetrile could harm cancer cells while leaving healthy cells largely untouched. For someone who has heard hard truths about surgery, chemotherapy, or radiation, that message can feel like relief.
The theory was usually presented in a simple chain of events. Amygdalin enters the body. It breaks down into several compounds, including cyanide. Advocates then claimed cancer cells were less able to defend themselves against that cyanide, while normal cells would stay protected by their own enzymes.
On paper, that can sound neat and targeted. In clinic, I understand why patients pause at that explanation and ask, "If it makes sense, why not try it?"
Because a biologically appealing story is only the opening chapter.
Where the theory runs into real-world medicine
Cancer biology is rarely that tidy. Tumors are not all alike, even within the same diagnosis. The human body is also not a test tube. A substance may behave one way in a simplified theory and very differently in an actual patient with variable metabolism, other medications, changing nutrition, and stressed organ systems.
That distinction is easy to miss. A mechanism is a hypothesis about how something might work. A treatment recommendation requires evidence that people benefited, and that the harms were acceptable in the context of their disease.
An analogy helps here. A blueprint can look excellent on paper and still fail once the building is exposed to weather, weight, and daily use. Medical theories work the same way. They must hold up in real patients, not only in a persuasive explanation.
Why this history still matters now
The B17 story is not only about a disputed compound. It is also about a decision many patients face after diagnosis. How do you respond when a treatment is presented as natural, suppressed, or unfairly dismissed?
A safer approach is to slow the conversation down and ask better questions. What is the proposed mechanism? Has it shown patient benefit, not just laboratory activity? What are the known harms? Could it interfere with standard treatment? What would your oncologist want to monitor if you were considering it anyway?
Those questions shift the discussion from hope alone to informed choice. That is the part many articles miss. Patients do not need ridicule for asking about B17. They need a framework for judging claims, protecting their safety, and bringing difficult questions into the exam room without embarrassment.
What the Clinical Evidence Shows
A patient sits across from me and says, “I know the internet says mixed things, but has anyone studied this in people?” That is the right question.
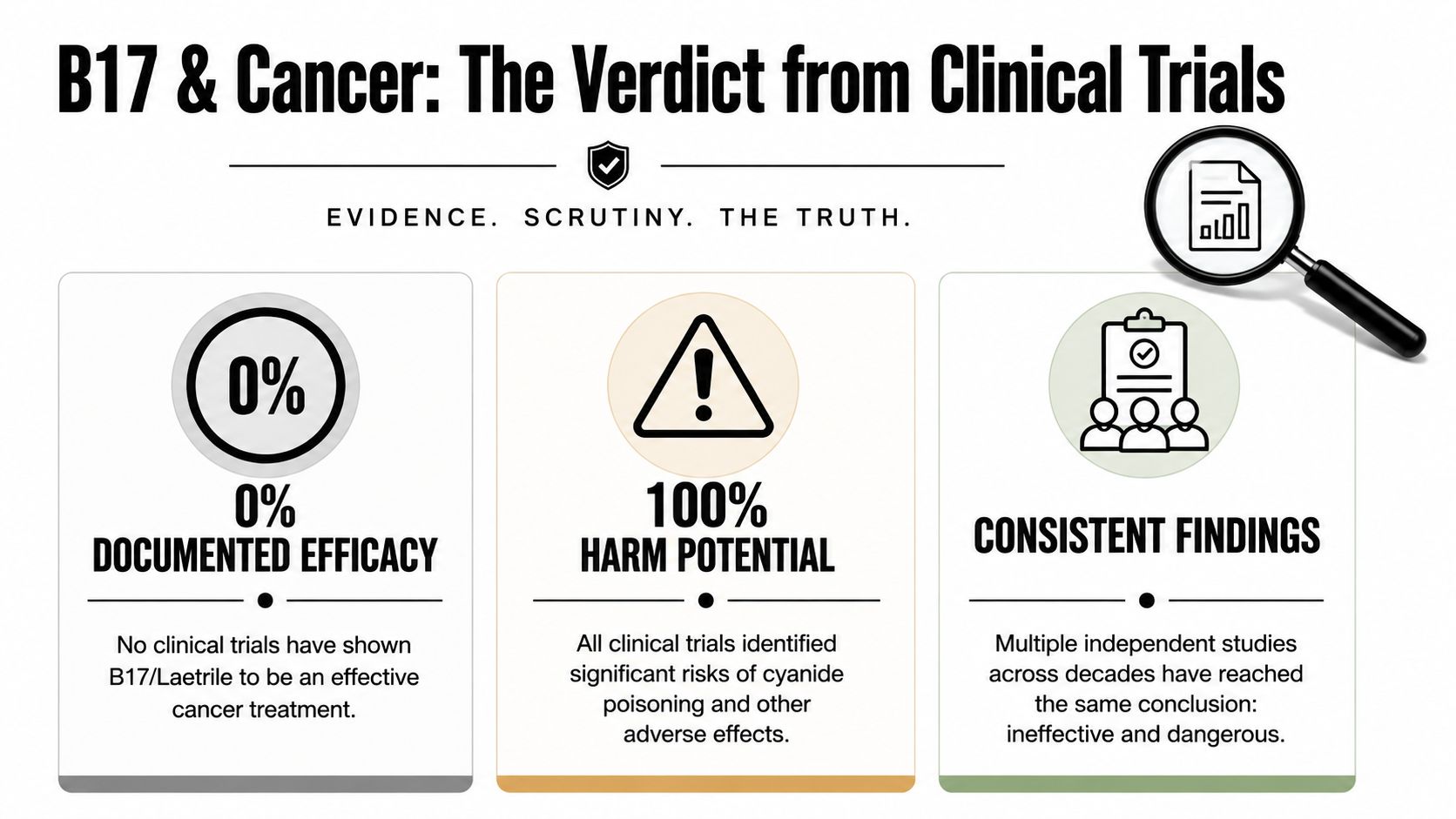
When oncologists judge a cancer treatment, the standard is simple. We look for evidence that real patients lived longer, felt better in a lasting way, or had measurable control of their cancer in careful human studies. For laetrile and amygdalin, that level of evidence has not shown a proven anticancer benefit.
What happened in human studies
The central finding from the human research is straightforward. Investigators did not find meaningful improvement in tumor response, survival, or overall clinical outcomes. Some reports described temporary symptom relief in a subset of patients, but short-term symptom changes are common in cancer care and do not prove that a treatment is controlling the disease.
That distinction matters. A person can feel better for a period of time because of other medications, changes in inflammation, day-to-day variation in symptoms, or the natural ups and downs of illness. What doctors need to see is durable benefit that holds up across patients. That has not been shown for B17 products.
What happened in laboratory and animal research
Preclinical research also failed to build a convincing case. The signal was weak, inconsistent, or absent in models that should have strengthened confidence before broader use in patients.
This is a common point of confusion online. Laboratory findings can be useful as a starting point, but they are closer to a dress rehearsal than an opening night performance. Cells in a dish do not capture the complexity of a human body, and animal models often fail to predict what will help actual patients with cancer.
How to read the evidence without getting lost
A lot of B17 marketing blends together different kinds of proof as if they carry the same weight. They do not.
A practical way to sort the claims looks like this:
| Type of claim | How much weight to give it |
|---|---|
| Personal story | Low. It may be genuine, but it cannot show that B17 caused the result |
| Theory about how it should work | Limited. Useful for research questions, not enough for treatment decisions |
| Lab or animal findings | More informative than theory alone, but still not proof for patient care |
| Human clinical outcomes | Highest value because they show what happened in people, not just what was hoped for |
If you are trying to decide what to do next, this table gives you a way to slow down and sort information before acting on it.
That “what now?” step is where many articles stop too soon. Patients are often left with a blunt message that B17 is unsupported, but not much help on what to do with that information. A better next step is to bring the claim into the exam room and ask your oncologist to place it in context. Does it improve survival? Does it shrink tumors? Could it interfere with treatment, nutrition, or symptom control? The same careful approach matters with other supplements and nonstandard therapies, including questions about antioxidants during cancer treatment.
Here is the plain-language conclusion. After decades of interest, B17 has not earned a role as an evidence-based cancer treatment. That does not make you foolish for asking about it. It means the safest, most constructive path is to use the question as a starting point for a broader treatment conversation, one focused on benefit, risk, and what gives you the best chance of real help.
Understanding the Significant Safety Risks
A patient may hear "vitamin" and assume the downside is minor. That assumption is dangerous here.
With laetrile and amygdalin, the main safety concern is cyanide poisoning. For someone already coping with cancer, treatment side effects, and a flood of conflicting advice, that risk changes the conversation from "Could this help?" to "Could this cause harm before it offers any proven benefit?"
What happens in the body
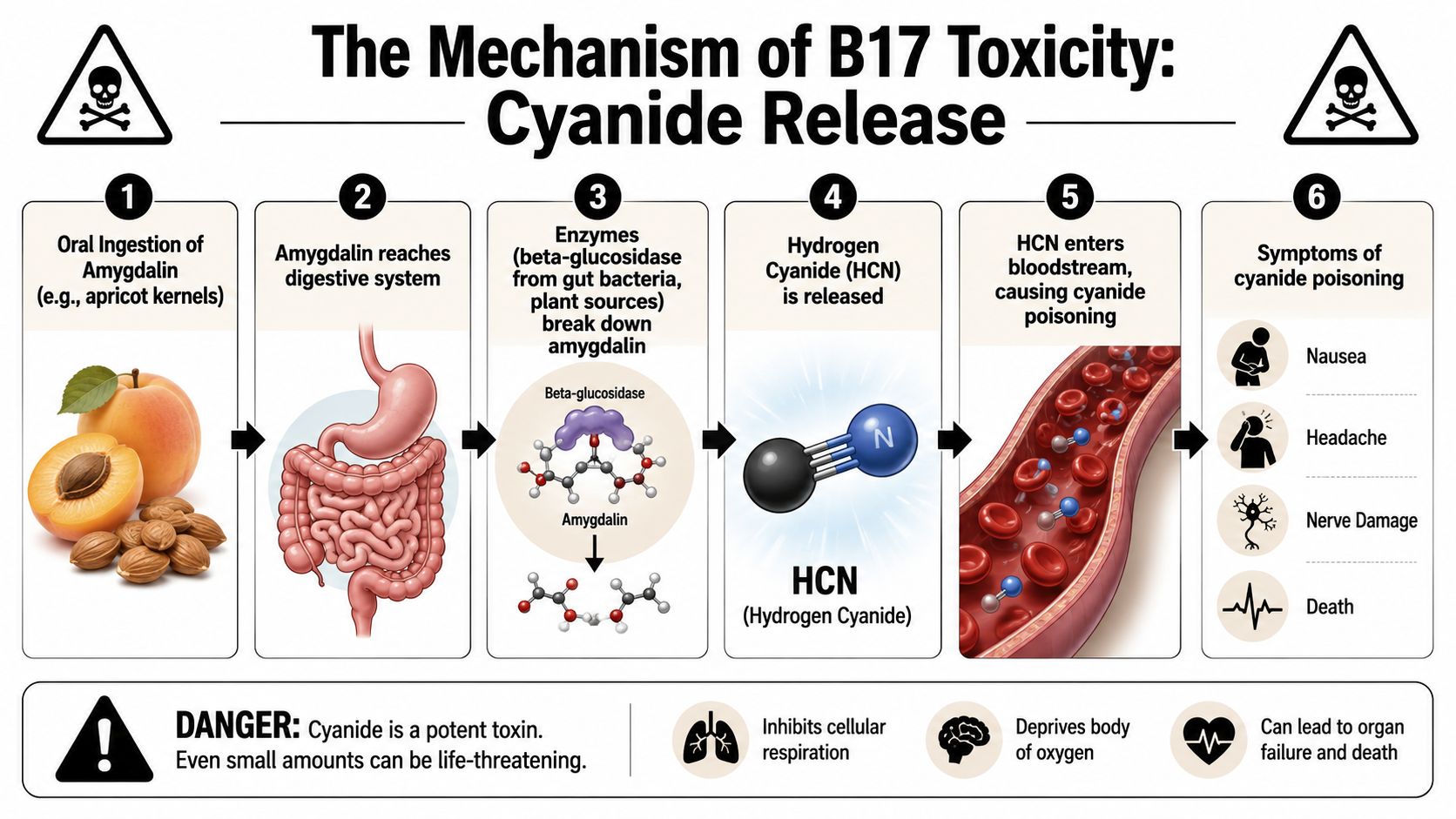
Amygdalin is a cyanogenic glycoside. After it is swallowed and digested, the body can break it down into compounds that release hydrogen cyanide. Cyanide interferes with how cells use oxygen. In plain terms, it blocks a basic process your brain, heart, and other organs need to stay alive.
That is why oral use raises special concern. The digestive tract can increase cyanide release, so a product marketed as natural can behave like a poison once it is metabolized.
Here's a short explainer that helps visualize the issue:
The harms doctors worry about
Cancer Research UK warns that laetrile can cause cyanide toxicity and describes serious reactions such as nausea, vomiting, headache, dizziness, confusion, low blood pressure, liver problems, nerve injury, coma, and death on its Cancer Research UK page on laetrile.
Some patients expect a dangerous product to feel obviously dangerous right away. That is not always how this works. Early symptoms of cyanide poisoning can look like problems many cancer patients already deal with, including weakness, nausea, fatigue, lightheadedness, or mental fog. That overlap can delay recognition and make emergency evaluation harder.
As noted earlier, human reports and clinical observations have also documented cyanide toxicity after amygdalin or laetrile use. The practical message is simple. This is not a harmless supplement with uncertain benefit. It is a substance with no proven anticancer effect and a known mechanism for serious poisoning.
Why this matters in real-world cancer care
For patients, the key question is often, "What does this mean for me right now?" It means risk has to be judged in the setting of your actual treatment plan, your symptoms, and your overall strength.
B17 can create problems in several ways:
- Direct toxicity from cyanide release
- Worsening of existing symptoms such as nausea, dizziness, confusion, or poor appetite
- Confusion during treatment because toxic effects may resemble chemotherapy side effects, dehydration, infection, or disease progression
- Delay in getting effective care if attention shifts toward an unproven product instead of symptom control and treatments that have been tested in patients
This broader point matters beyond B17. Many alternative products sound gentle because they come from plants, seeds, or "natural" sources, but that label does not predict safety during cancer care. If you want a practical example of how oncologists assess these questions, our guide to antioxidants during cancer treatment walks through the same safety-first approach.
If you have been looking into B17 because you want every possible chance to fight your cancer, that instinct is understandable. The safer next step is not to hide the question. It is to bring it to your oncology team so the discussion can focus on your goals, your treatment, and your safety.
How to Talk to Your Oncologist About B17
Many patients hesitate here. They worry their oncologist will dismiss them, sound irritated, or think they've been reckless. Good oncology care shouldn't work that way. Your doctor needs accurate information to protect you, not to judge you.
If you've searched B17 and cancer, bought apricot kernel products, or already taken amygdalin, say so directly. The conversation can be simple.
A script you can actually use
You can say:
I came across B17 or amygdalin online. I'm not sure what to believe, and I want to make safe choices. Can you help me understand whether it's dangerous with my treatment?
If you've already taken it, say that too:
I've already used this product, and I want to be honest about it. I'm especially worried about whether it could interact with my treatment or cause harm.
That kind of sentence helps your oncologist focus on what matters most. Timing, amount, symptoms, current medications, and whether you took it by mouth all affect the safety discussion.
What your oncologist needs to know
Bring the bottle, label, website screenshot, or ingredient list if you have it. "Natural supplement" isn't enough information. Products sold as B17 may vary in naming and formulation.
Use this checklist at your appointment:
Show the actual product
Bring packaging or a photo of the label. Your team needs the exact name and ingredients.Describe how you took it
Oral use matters because the NCI notes side effects are worse when laetrile is taken by mouth, and can be intensified by eating raw almonds or crushed fruit pits, as explained in the NCI patient page on laetrile safety.Mention related foods
If you also ate apricot kernels, raw almonds, or crushed fruit pits, say so clearly. That combination may worsen cyanide toxicity.Report any symptoms, even if they seem mild
Nausea, vomiting, headache, dizziness, confusion, weakness, or low blood pressure shouldn't be brushed off.
What to do if you've already started
Don't keep taking it in secret while you decide. Contact your oncology team. If you feel acutely unwell after taking an amygdalin or laetrile product, seek urgent medical care.
For a planned discussion about treatment options, supplement safety, and next steps, some patients also choose to speak with practices such as Hirschfeld Oncology, which provides oncology care and consultation around individualized treatment planning.
The most useful mindset is partnership. Your oncologist's job isn't only to prescribe chemotherapy or immunotherapy. It's also to help you avoid harm from treatments that don't help.
Your Path Forward with Evidence and Hope
For those investigating B17 and cancer, the pursuit is typically for something greater than a mere supplement. They're searching for another chance, another angle, another reason to keep going.
That search deserves respect. But respect also means honesty.
B17 isn't a true vitamin. Human studies haven't shown a proven anticancer benefit. The known safety concern is cyanide poisoning, especially with oral use and certain combinations that can make toxicity worse. That means the most hopeful next step isn't trying to make B17 safer or searching for the "right" brand. It's bringing your questions into the exam room and building a plan around treatments and supportive care that have a real scientific basis.
Hope in oncology shouldn't depend on rumor. It can come from better symptom control, smarter treatment sequencing, clinical trial discussions, targeted therapy when appropriate, immunotherapy in the right setting, and careful adjustment of care to match your goals and tolerance.
You don't have to face that alone, and you don't have to hide the questions you've been carrying.
If you're weighing unconventional cancer therapies and want a clear, medically grounded conversation about risks, evidence, and treatment options, the Hirschfeld Oncology blog offers practical guidance for patients and families navigating complex decisions.
.png)
.png)




