




.png)


Introducing Adaptive Designs in Oncology
Adaptive clinical trial designs are research structures that allow pre‑specified, data‑driven modifications—such as changes to sample size, randomization ratios, or treatment arms—while preserving statistical validity and trial integrity. Unlike traditional fixed‑sample trials, which lock all parameters at the start, adaptive designs incorporate interim analyses governed by strict decision rules, enabling early stopping for futility or efficacy, dose‑adjustment, arm dropping, or enrichment of responsive subpopulations. This flexibility matters profoundly in cancer research because tumor biology is heterogeneous, patient populations can be limited, and rapid identification of effective therapies can mean the difference between life and death. By reallocating patients toward promising regimens and truncating exposure to ineffective or unsafe treatments, adaptive designs improve ethical conduct, reduce trial duration, and lower overall costs. In the United States, both the Food and Drug Administration (FDA) and the European Medicines Agency (EMA) have issued guidance encouraging adaptive approaches, emphasizing prospective planning, control of type I error, independent data‑monitoring committees, and transparent reporting. The FDA’s 2019 Guidance for Industry on Adaptive Designs for Clinical Trials of Drugs and Biologics outlines these expectations and provides a regulatory framework that supports the broader adoption of adaptive methods in oncology trials.
Fundamentals and Core Methods
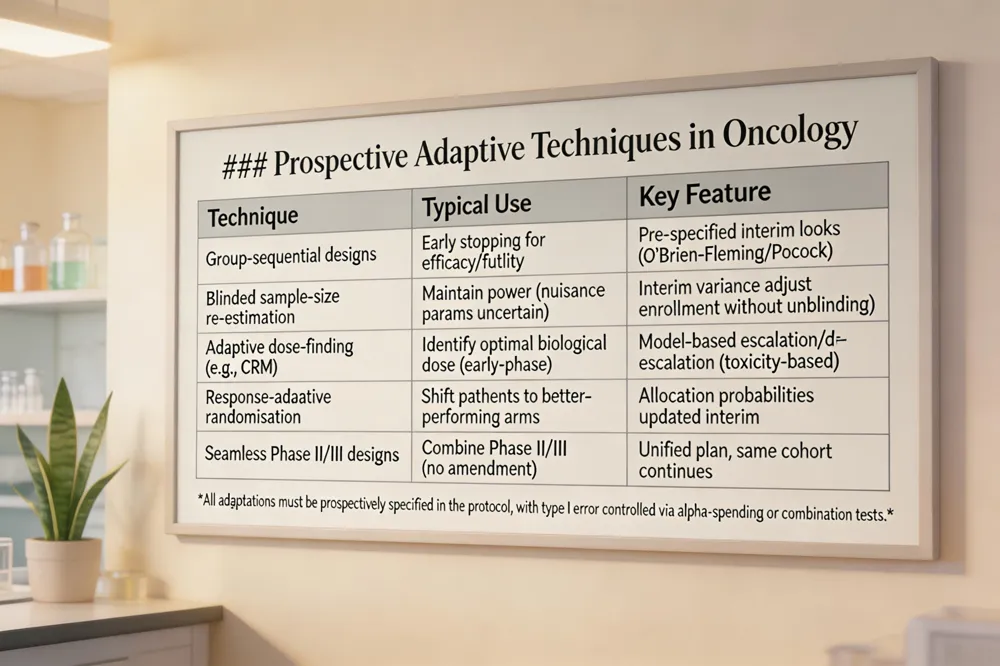 Common prospective techniques in oncology include group‑sequential designs with pre‑defined stopping boundaries, blinded sample‑size re‑estimation to maintain power when nuisance parameters are uncertain, adaptive dose‑finding (e.g., CRM) in early phases, response‑adaptive randomization that shifts allocation toward more effective arms, and seamless Phase II/III designs that combine learning and confirmatory stages without a protocol amendment.
Regulatory agencies such as the U.S. FDA and EMA require that all adaptations be pre‑specified in the protocol, that the overall type I error rate be controlled (often via alpha‑spending functions or combination tests), and that an independent data‑monitoring committee conduct interim analyses while maintaining blinding to prevent operational bias. Detailed simulation studies must be provided to demonstrate operating characteristics, and any unplanned modifications must be documented transparently in the final trial report.
Question: What are the adaptive design methods? Answer: Adaptive design methods are statistical strategies that allow pre‑specified modifications to a clinical trial based on interim data without compromising its integrity. They are generally classified into three categories: prospective (planned before the trial begins), concurrent or ad‑hoc (changes made during the trial in response to emerging information), and retrospective (post‑hoc analyses that adjust the design after data are collected). Common prospective techniques include group‑sequential stopping rules, sample‑size re‑estimation, adaptive dose‑finding, response‑adaptive randomization, and seamless phase II/III designs that combine learning and confirmatory stages. Concurrent adaptations often involve dropping or adding treatment arms, modifying eligibility criteria, or adjusting allocation ratios as the study progresses. Retrospective adaptations are typically used for exploratory re‑analysis or to refine future trial designs based on the observed patient population.
Advantages and Disadvantages of Adaptive Trials
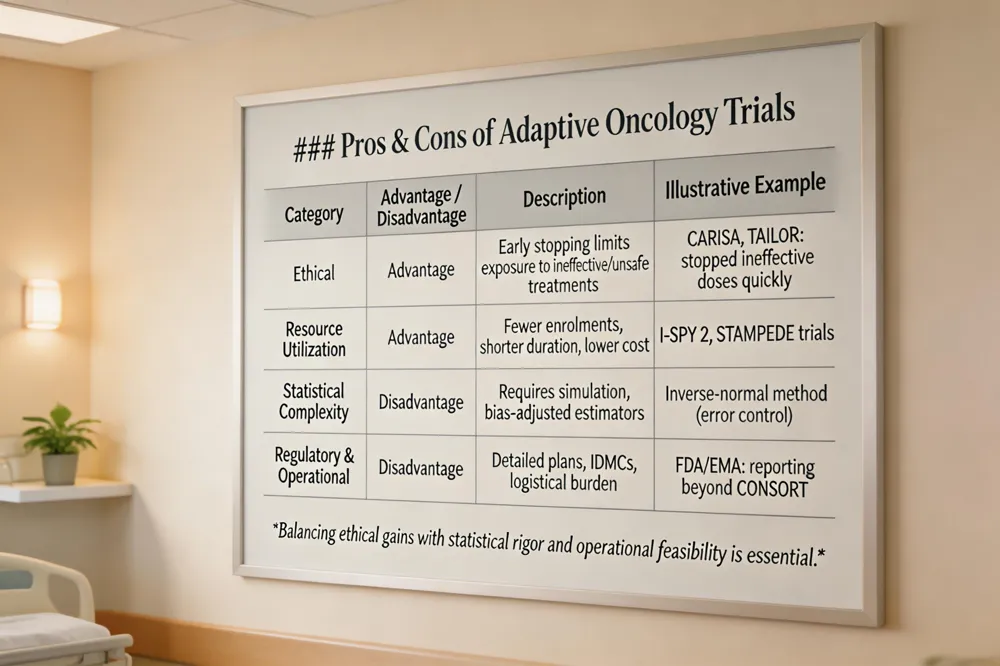 Ethical benefits stem from early stopping for futility or efficacy, limiting patient exposure to ineffective or unsafe arms. Trials like CARISA (sample‑size re‑estimation) and TAILoR (MAMS) illustrate how ineffective doses are dropped quickly, protecting participants and delivering promising therapies faster.
Resource utilization and cost savings follow from fewer enrolments, shorter trial duration, and shared control arms in platform or master‑protocol trials (e.g., I‑SPY 2, STAMPEDE). This translates into lower development costs and faster market entry for oncology drugs, including pancreatic cancer candidates.
Conversely, complexity of statistical planning and simulation is a major drawback. Maintaining unbiased effect estimates, correct confidence‑interval coverage, and type I error control requires extensive simulation studies, bias‑adjusted estimators, and combination tests (e.g., inverse‑normal method).
Regulatory scrutiny and operational challenges add another layer of difficulty. The FDA and EMA demand detailed adaptation plans, independent Data Monitoring Committees, and transparent reporting beyond CONSORT. Real‑time data capture, rapid protocol amendments, and strict firewalls to prevent information leakage increase logistical burden and cost.
In summary, adaptive designs offer flexibility, ethical advantages, and efficiency, but they require sophisticated statistical expertise, rigorous regulatory documentation, and robust operational infrastructure to avoid bias and preserve trial integrity.
Bayesian Adaptive Designs in Cancer Research
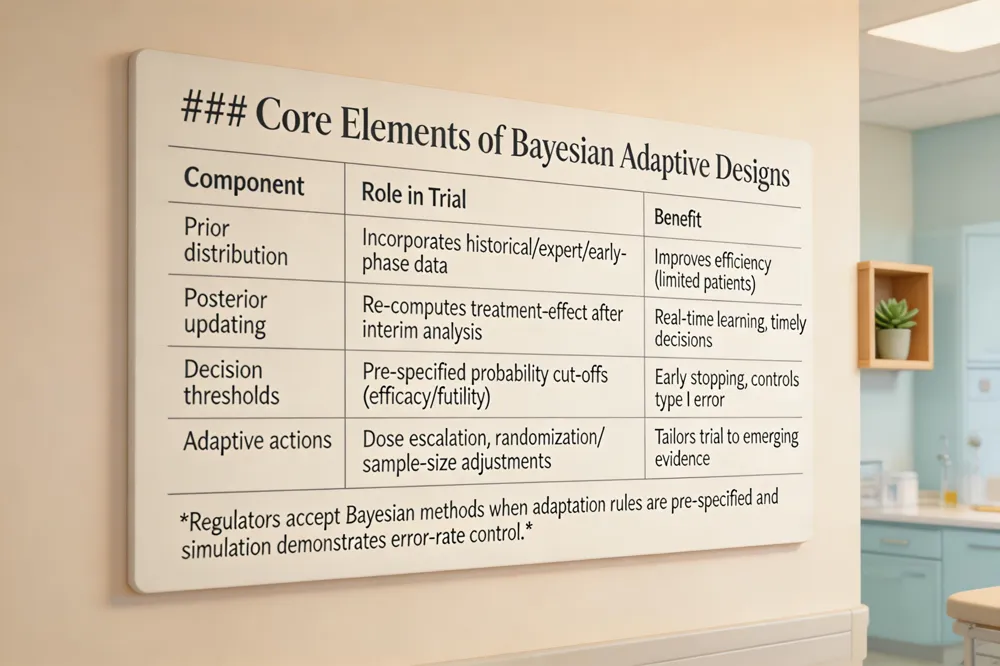 Bayesian adaptive designs integrate prior knowledge—historical trial data, expert opinion, or early‑phase results—into a probabilistic model that is continuously updated as patient outcomes accrue. At each pre‑specified interim analysis the posterior distribution of the treatment effect is recomputed, and adaptation decisions (e.g., dose escalation, randomization probabilities, or sample‑size changes) are triggered when the posterior probability crosses defined thresholds. This real‑time learning permits early stopping for efficacy when a high posterior probability of benefit is observed, or for futility when the probability of a clinically meaningful effect falls below a prespecified cut‑off, thereby protecting patients from ineffective or unsafe therapy. In aggressive tumors such as pancreatic adenocarcinoma, where patient numbers are limited and rapid decision‑making is critical, Bayesian methods enable enrichment of responders and efficient dose‑finding while maintaining ethical standards. Regulatory agencies—including the U.S. FDA—support Bayesian adaptive approaches provided that the protocol contains a priori adaptation rules and that extensive simulation studies demonstrate control of the overall type I error rate, appropriate power, and robust estimation. Consequently, Bayesian adaptive trials are becoming a cornerstone of precision oncology, accelerating the development of effective therapies while preserving scientific rigor.
Types of Adaptive Designs Used in Oncology
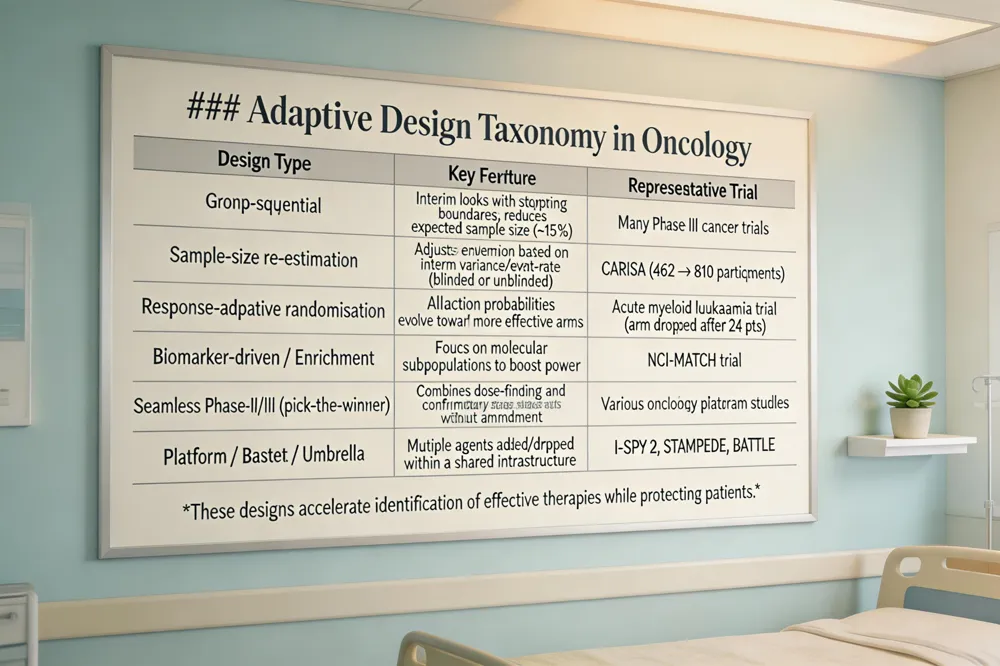 Adaptive trial designs in oncology encompass a range of pre‑specified modifications that preserve statistical validity while improving efficiency and patient safety. Group‑sequential designs employ interim analyses with O’Brien‑Fleming or Pocock boundaries, allowing early stopping for efficacy or futility and reducing expected sample size by roughly 15 % in many cancer studies. Sample‑size re‑estimation—both blinded and unblinded—adjusts enrollment numbers when nuisance parameters (e.g., variance or event rates) differ from assumptions, as illustrated by the CARISA trial’s increase from 462 to 810 participants to retain 90 % power. Response‑adaptive randomisation modifies allocation probabilities as outcome data accrue, shifting patients toward more effective arms and often leading to arm‑dropping, exemplified by the acute myeloid leukaemia trial that terminated a poorly performing arm after 24 patients. Biomarker‑driven and population enrichment designs focus enrollment on molecularly defined subpopulations, increasing power while preserving broader assessment; the NCI‑MATCH trial is a hallmark example. Seamless phase II/III or “pick‑the‑winner” designs merge dose‑finding and confirmatory stages, streamlining development, while platform trials, basket trials, and umbrella trials enable multiple investigational agents to be added or dropped within a single infrastructure, as seen in I‑SPY 2 and STAMPEDE. Together, these adaptive strategies accelerate identification of effective cancer therapies, limit exposure to ineffective treatments, and lower development costs.
Regulatory Guidance and Reporting Standards
 The EMA’s qualification of adaptive methods and real‑world evidence similarly encourages adaptive enrichment, biomarkers, and real‑world datasets, provided that the adaptation rules are prospectively defined and that type I error control is preserved. Both agencies expect clear reporting of the rationale, decision criteria, timing of interim looks, and the statistical techniques used for bias‑adjusted estimation.
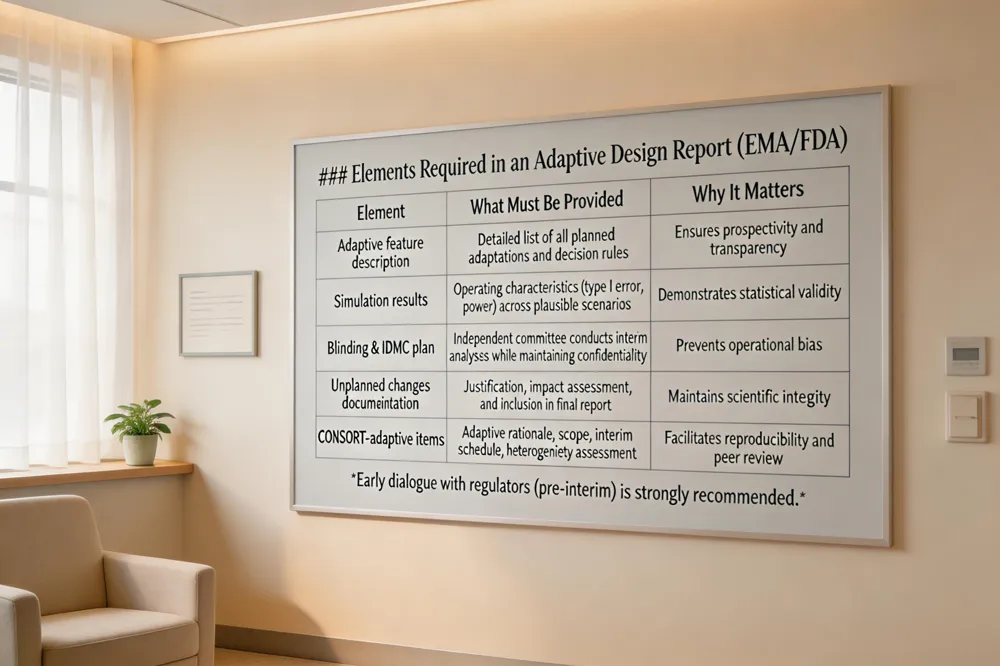
Key elements of an Adaptive Design Report include: (1) a thorough description of the adaptive features and decision rules; (2) simulation results that confirm error‑rate control and power across plausible scenarios; (3) plans for maintaining blinding and independent data monitoring; and (4) documentation of any unplanned changes with justification and impact assessment. The CONSORT extension for adaptive trials adds items such as the adaptive rationale, detailed adaptation scope, interim analysis schedule, and heterogeneity assessment across stages.
In practice, sponsors should prepare a protocol appendix that outlines all adaptation scenarios, secure independent review by an IDMC, and submit the Adaptive Design Report alongside the regulatory application. Early dialogue with the FDA or EMA—preferably before the first interim analysis—helps to confirm that the adaptive design meets the agency’s statistical and ethical standards, thereby smoothing the path to approval while protecting trial integrity.
Practical Implementation: Funding, Ethics, and Operations
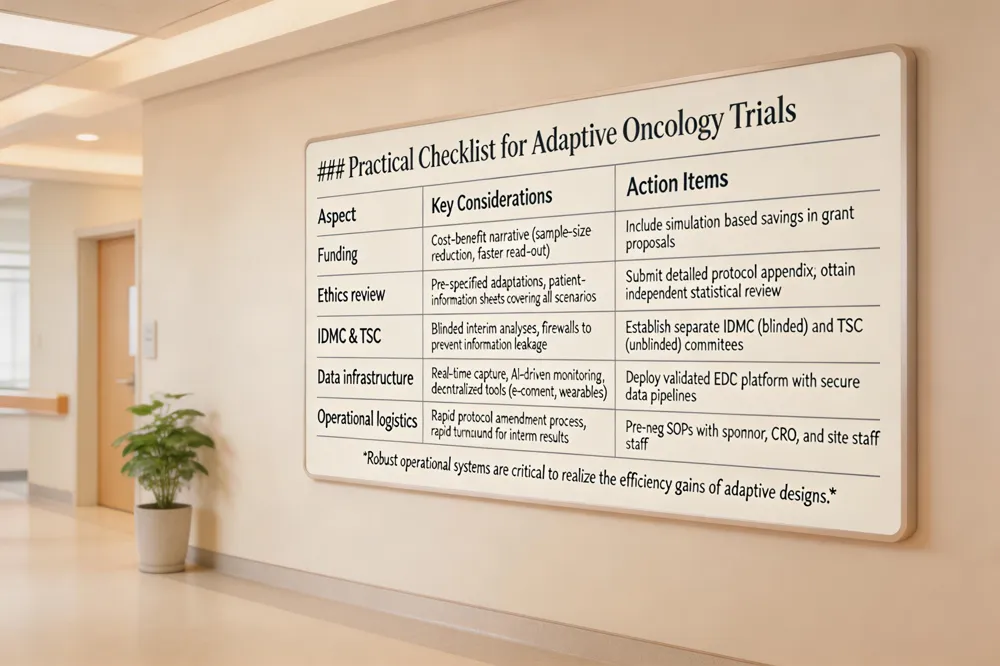 Secure funding for an adaptive oncology trial begins with translating the statistical advantages—such as reduced sample size, shorter duration, and ethical gains—into a concise, non‑technical narrative for grant panels or industry partners. Funding agencies often require a clear cost‑benefit analysis, which can be built from simulation results showing expected savings (see FDA 2019 guidance.
Ethics committee review must address the pre‑specified nature of all adaptations. Independent statistical review is frequently requested to verify that interim decision rules (e.g., group‑sequential boundaries, sample‑size re‑estimation preserve type I error control and patient safety. The committee also expects patient‑information sheets that outline every possible scenario—early stopping for futility or efficacy, arm dropping, sample‑size adjustments, and biomarker enrichment—so participants understand how the trial may evolve.
Maintaining integrity requires a blinded Independent Data Monitoring Committee (IDMC) that conducts interim analyses without revealing comparative results to investigators. A separate blinded Trial Steering Committee (TSC) reviews any ad‑hoc modifications, with strict firewalls to prevent information leakage, as recommended in the CARISA and TAILoR examples.
Operationally, adaptive trials rely on real‑time data capture platforms that feed interim analyses promptly. Incorporating AI‑driven monitoring and decentralized technologies (e.g., virtual consent, home drug delivery, wearable safety) supports rapid decision‑making and broadens patient access, aligning with NCI’s Clinical Trials Innovation Unit initiatives. Together, these practical steps enable adaptive designs to deliver faster, safer, and more efficient oncology studies.
Illustrative Case Studies and Educational Resources
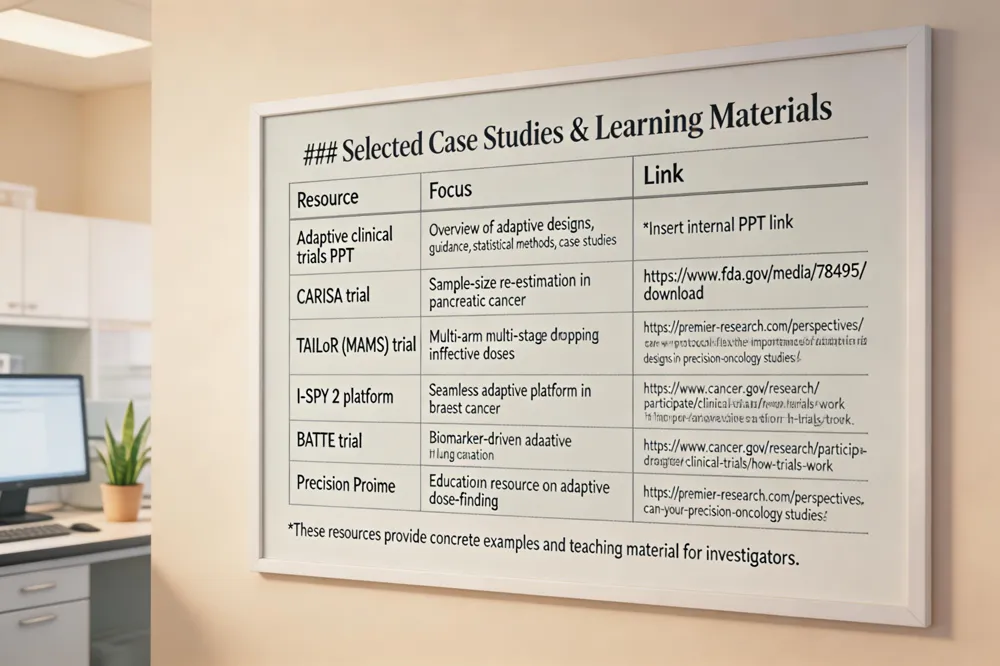 Adaptive clinical trials ppt – A typical PowerPoint deck begins by defining adaptive designs and contrasting them with fixed‑sample trials, then outlines FDA and EMA guidance that require prespecified adaptation rules, independent data‑monitoring committees, and strict type I error control. The presentation explains core statistical methods—group‑sequential testing, Bayesian updating, and response‑adaptive randomisation—followed by real‑world case studies (CARISA, TAILoR, I‑SPY 2, BATTLE, Precision Promise) that demonstrate accelerated decision‑making and ethical benefits. Finally, practical implementation tips cover interim‑analysis timing, data‑capture infrastructure, and communication strategies for investigators, ensuring that adaptive trials are conducted safely, efficiently, and transparently.
Future Horizons: AI, Real‑World Evidence, and Adaptive Devices
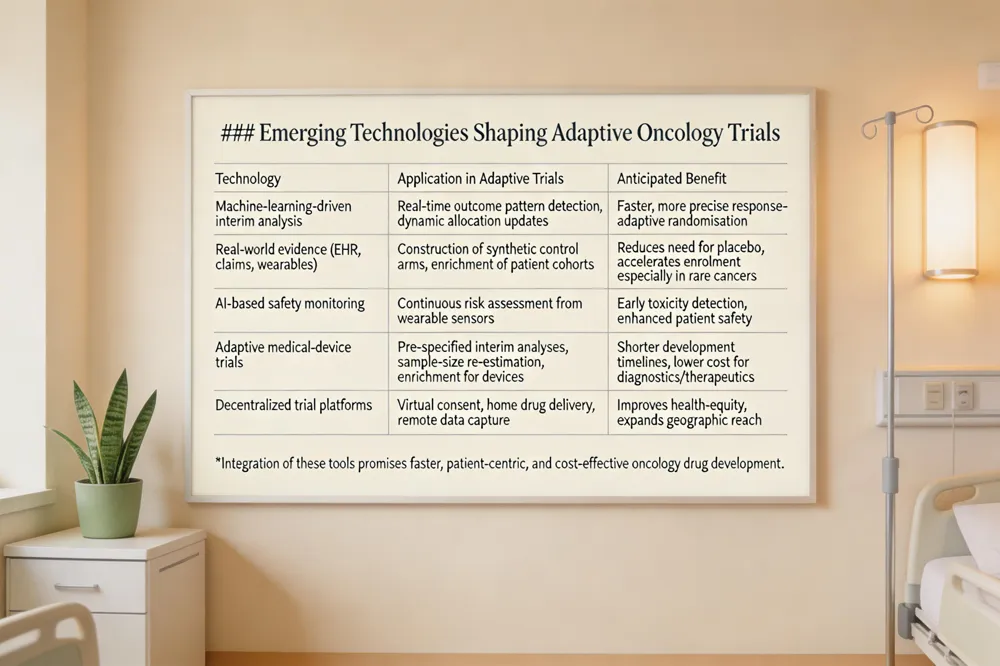 Machine‑learning algorithms are reshaping interim decision‑making in adaptive oncology trials. By continuously analyzing accumulating outcomes, AI can flag early efficacy signals, update Bayesian probability models, and recommend allocation adjustments in real time, thereby improving the speed and precision of response‑adaptive randomisation. At the same time, the incorporation of real‑world evidence (RWE) – electronic health records, claims data, and wearable‑device streams – enables the construction of synthetic control arms that reduce the need for placebo groups and accelerate patient enrolment. This approach is especially valuable for rare cancers, where patient numbers are limited and traditional control cohorts are often infeasible. Adaptive designs are also extending into medical‑device studies. The FDA’s guidance on adaptive designs for device trials permits pre‑specified interim analyses, sample‑size re‑estimation, and adaptive enrichment while preserving statistical validity, allowing innovative diagnostics or therapeutic devices to reach the market faster and at lower cost. Finally, these technologies support decentralized, patient‑centric trial models: virtual consent, home‑delivery of investigational products, and AI‑driven safety monitoring enable broader participation, improve health‑equity, and maintain rigorous oversight throughout the adaptive trial lifecycle.
The Bottom Line for Adaptive Oncology Trials
Adaptive clinical trial designs are reshaping cancer research by delivering greater efficiency, stronger ethical safeguards, and faster timelines. Pre‑specified interim analyses let investigators trim sample sizes, drop futile arms, and re‑allocate patients to promising therapies, reducing exposure to ineffective treatments and shortening trial duration. These efficiencies translate into lower costs and quicker access to effective drugs for patients with aggressive cancers such as pancreatic adenocarcinoma. However, the flexibility of adaptive designs comes with a responsibility for rigorous statistical planning and clear regulatory alignment. Sponsors must prespecify adaptation rules, conduct extensive simulation studies to confirm control of the family‑wise type I error, and establish independent data‑monitoring committees that preserve blinding and trial integrity. Detailed documentation of the adaptation rationale, timing, and decision criteria is required by FDA and EMA guidance and by CONSORT extensions for adaptive trials. Hirschfeld Oncology exemplifies this forward‑looking approach. By integrating robust adaptive methodologies—such as blinded sample‑size re‑estimation, multi‑arm multi‑stage designs, and biomarker‑driven enrichment—into its pancreatic‑cancer programs, the center delivers patient‑centered, precision‑medicine trials that accelerate therapeutic discovery while maintaining the highest standards of safety and scientific validity. This model illustrates how innovative trial design can improve outcomes for patients and streamline drug development in the United States.
.png)
.png)




