




.png)


One family sits in my office with a notebook full of questions. The patient has already been through standard treatment, and the phrase they keep coming back to is simple: “Is there anything new?”
That question is exactly why there is such widespread interest in mRNA cancer vaccine trials.
A New Horizon in Cancer Treatment
A family hears the word “vaccine” and pictures prevention. They picture flu shots, childhood immunizations, and protection before illness starts. Then they sit in an oncology office and learn that an mRNA cancer vaccine trial is trying to do something different. It is trying to help the immune system see a cancer that is already there.
That shift in meaning matters, especially for patients with advanced disease who have already been through surgery, chemotherapy, radiation, immunotherapy, or more than one of these. News about mRNA can sound exciting and hard to interpret at the same time. In the clinic, the situation is more nuanced. This is a serious area of research with significant promise, but it is still defined by clinical trials, careful patient selection, timing, and the fact that many patients will need more than one treatment working together.
Why people are paying attention
Interest in mRNA cancer vaccines grew quickly after COVID vaccines made the technology familiar to the public. That familiarity helps, but cancer is a tougher opponent than a virus. A virus is clearly foreign. Cancer starts from normal cells in the body, then changes just enough to grow, spread, and sometimes stay partly hidden from immune defenses.
mRNA vaccines are being studied as a way to make those hidden clues easier for the immune system to spot. A useful comparison is a clearer set of instructions for a search team. In some trials, those instructions are personalized from a patient's own tumor mutations. In others, researchers are testing shared targets that may apply to groups of patients with the same cancer type or molecular feature.
That does not make mRNA a shortcut around standard treatment.
For many advanced solid tumors, including pancreatic, bile duct, colorectal, gastric, and ovarian cancers, the central question is not whether an mRNA vaccine seems particularly novel. The better question is whether it fits the biology of the tumor and whether it is being paired with the right partners, such as checkpoint inhibitors, targeted therapy, chemotherapy, or surgery. That balanced view is especially important in practices like Hirschfeld Oncology, where patients often come in after standard treatment has already been tested and time matters.
Practical rule: Ask two questions together. “Could this trial help my cancer?” and “What other treatment does it need to work well?”
What patients and families need most
Patients and families do not need more hype. They need a plain-language explanation of where the science is encouraging, where the limits are real, and what trial participation involves.
That is particularly true in New York City, where patients may have access to major academic centers and early-phase trials, but still face the same hard realities seen everywhere else. A promising trial is not the same as a proven therapy. Some studies are designed to test safety. Some are asking whether the vaccine helps the immune system respond more strongly. Only a smaller number can answer whether patients live longer or stay in remission longer.
Hope belongs here. So does realism.
The most helpful conversation usually sounds like this: What is the goal of this trial, how likely is it to match my tumor type and stage, what are the risks, and is combination treatment part of the plan? Those questions help families move from headlines to informed decisions.
How mRNA Vaccines Teach Your Body to Fight Cancer
The easiest way to understand mRNA cancer vaccine trials is to think of the vaccine as a most wanted poster for your immune system.
Cancer cells often carry abnormal markers created by mutations. These markers are called neoantigens. They can act like fingerprints. The problem is that your immune system may not notice them well enough, or may notice them too late. An mRNA vaccine is designed to improve that recognition.
The most wanted poster analogy
Here's the basic idea in plain language. The vaccine does not contain your cancer. It contains instructions that help the body make a harmless piece of information related to the cancer target. Your immune system studies that signal and learns what to look for.

If you want a broader non-cancer primer on how this platform works, VirusFAQ.com's mRNA insights offer a useful overview in everyday language.
What happens step by step
A tumor sample is collected
This often comes from a biopsy or surgery. Researchers analyze the tumor to identify mutations that are distinctive to that cancer.The likely targets are selected
Not every mutation makes a good immune target. Scientists look for neoantigens that seem most likely to be recognized by the immune system.The vaccine is designed
The mRNA acts like a temporary instruction set. It tells certain cells in the body to make proteins or protein fragments that match those cancer targets.The immune system trains
Immune cells, especially T cells, are exposed to those target signals. The hope is that they become better at spotting and attacking real cancer cells carrying the same markers.The body mounts a more focused attack
If the process works, the immune system starts treating those tumor signals less like background noise and more like a threat.
Where readers often get confused
The first confusion is about DNA. mRNA doesn't rewrite your genes. It's a temporary messenger. It gives instructions and then breaks down.
The second confusion is about personalization. Some mRNA cancer vaccines are designed for one person's tumor. Others are not fully individualized. Both are being studied, but they are not interchangeable.
The third confusion is about immunotherapy. A vaccine is one kind of immune-based treatment, but it's not the same as checkpoint inhibitor therapy. Checkpoint inhibitors remove brakes from the immune system. A vaccine helps show the immune system what to chase. Many patients understand this more clearly after reading a basic overview of immunotherapy for cancer.
Think of it this way. The vaccine provides the mugshot. The checkpoint inhibitor may help the immune system stop hesitating.
What Recent Clinical Trials Reveal About Efficacy
The strongest reason patients are asking about mRNA cancer vaccine trials is simple. Some recent studies have produced results that are hard to ignore.
Not every cancer responds the same way, and not every patient will benefit. Still, the early signal in selected settings is meaningful enough that this field has moved from a theoretical discussion to a practical one.

Melanoma and pancreatic cancer stand out
In a randomized phase IIb trial for high-risk stage III melanoma, a personalized mRNA neoantigen vaccine called mRNA-4157 combined with pembrolizumab reduced the risk of recurrence or death by 49% after 3 years compared with pembrolizumab alone, according to this review of mRNA vaccine clinical development.
In that same review, a phase 1 trial of an investigational pancreatic cancer vaccine showed that 87.5% of immune responders, 7 out of 8 patients, remained alive 4 to 6 years after surgery, while 25%, 2 out of 8 non-responders, were alive, with a median survival time of 3.4 years in non-responders. For a disease as difficult as pancreatic cancer, that kind of signal gets oncologists' attention.
The same review also notes that pancreatic cancer has a five-year survival rate of around 13%, which helps explain why even early vaccine success in this disease matters so much.
The broader trial landscape
This is not a niche effort happening in one lab. The same publication reports that the United States has 118 registered mRNA vaccine clinical trials, representing 35.9% of the top 15 countries, followed by China with 74 trials, 22.5%, and Australia with 22 trials, 6.7%. It also states that, as of October 2024, there were 51 ongoing clinical trials for mRNA cancer vaccines, with 24 in Phase II and III development.
That tells patients two important things:
- This field is active: there are many ongoing studies, not just isolated experiments.
- Cancer remains a central focus: in non-infectious disease research, mRNA vaccine work is concentrated largely in cancer therapy.
How to read encouraging results without overreading them
A trial result can be exciting and still limited. Early-phase studies may involve small groups. Some results apply only after surgery. Others depend on whether a patient's immune system mounted a strong response.
That's why evidence-based reading matters. If you want a helpful framework for judging trial headlines, this guide to informed health decisions can help families separate “promising” from “proven.”
For readers looking specifically at gastrointestinal cancers, the article on personalized vaccine development for pancreatic cancer gives useful background on why this area has become such a focus.
A good clinical trial result should make you more curious, not less cautious.
Why Combination Therapy Is Often Essential
This is the part many headlines skip.
Patients often hear about mRNA vaccines as though the vaccine itself is the whole treatment. For many advanced cancers, that's not how the biology works. The vaccine may be important, but it often needs partners.
Why a vaccine alone may not be enough
Metastatic cancers often live inside a strongly immunosuppressive environment. Oncologists sometimes call these cold tumors. That means the tumor and the tissue around it make it hard for immune cells to enter, activate, and keep fighting.
A vaccine can try to train T cells. But if the tumor microenvironment blocks those T cells, the lesson may not translate into tumor control.
A review focused on this problem states that the highly immunosuppressive tumor microenvironment of metastatic disease renders standalone mRNA vaccines ineffective. The same review reports that Moderna's mRNA-4157 combined with Keytruda achieved a 50% overall response rate in head and neck cancer, while colorectal cancer patients showed no response, highlighting how much neoantigen density and microenvironment matter, according to this analysis of mRNA vaccine limits and combination strategies.
What combination therapy tries to do
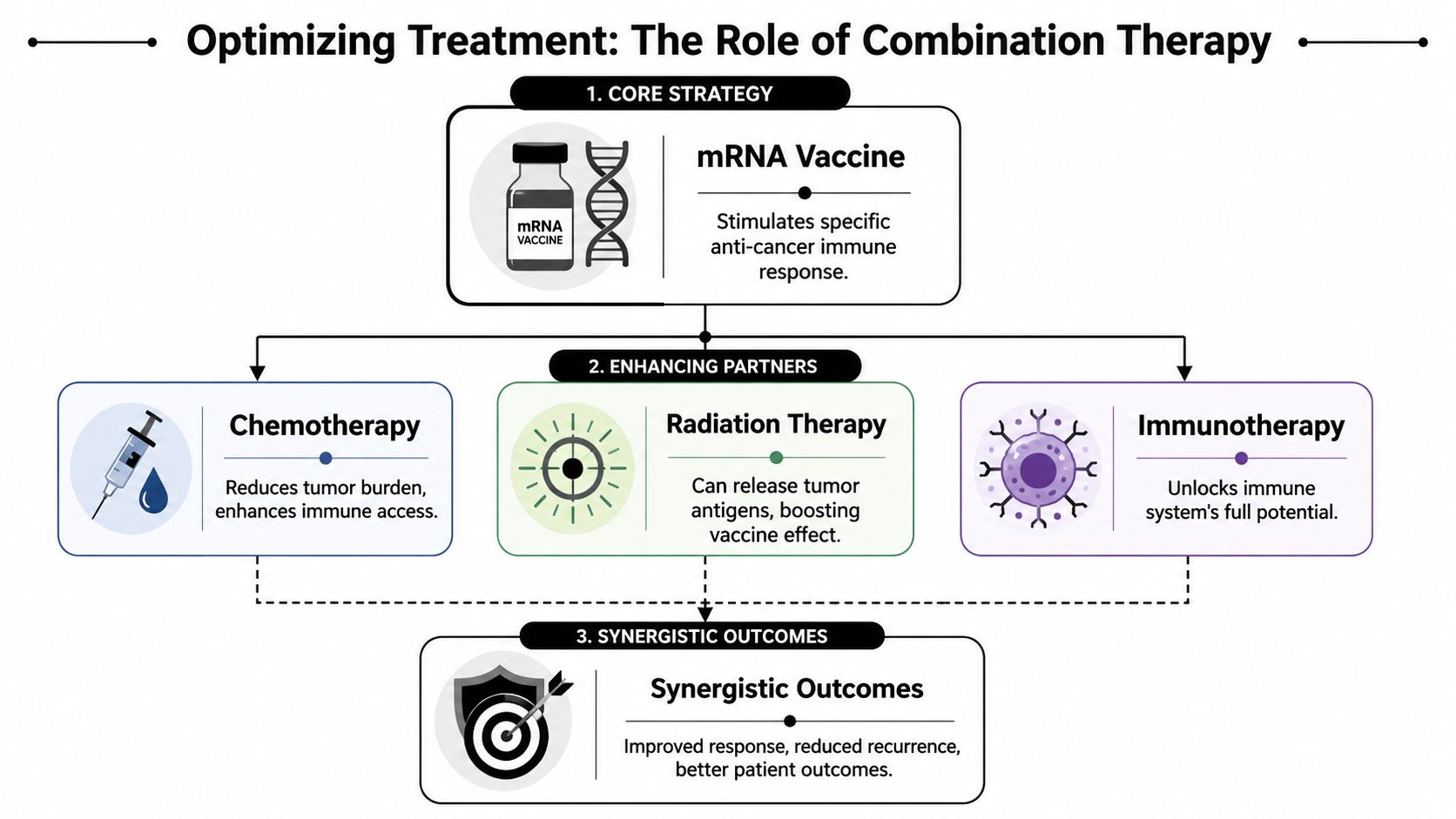
Different combinations aim to solve different obstacles:
| Treatment partner | What it may contribute |
|---|---|
| Checkpoint inhibitor | Helps release immune brakes so trained T cells can act |
| Chemotherapy | May reduce tumor burden and change immune access |
| Radiation | May expose tumor antigens and increase immune visibility |
This is why two patients can hear the phrase “mRNA vaccine” and be talking about very different treatment plans. One trial may pair the vaccine with pembrolizumab. Another may add chemotherapy. Another may focus on the post-surgery setting when tumor burden is lower.
Why this matters for hard-to-treat cancers
For pancreatic, ovarian, bile duct, and some colorectal cancers, the challenge isn't just building a vaccine. It's identifying targets that are visible enough and creating conditions where the immune system can act on them.
That's the reality families deserve to hear. A personalized vaccine is not a magic bullet for every stage IV cancer. In many cases, it's more accurate to think of it as one component of a broader immune strategy.
Some cancers are like a target in plain view. Others are hidden behind fog, walls, and locked doors. Combination therapy tries to clear the fog and open the doors.
Who Is Eligible for an mRNA Vaccine Trial
The question I hear most is not “Does this science exist?” It's “Could I qualify?”
Eligibility for mRNA cancer vaccine trials depends on the study design. There isn't one universal checklist. Still, several themes show up repeatedly.
The main factors doctors review
Cancer type matters
Some trials focus on melanoma. Others center on pancreatic cancer or another solid tumor. A trial usually targets a narrow patient population, not all cancers at once.Stage and timing matter
Certain studies enroll patients after surgery, when the goal is reducing recurrence risk. Others are designed for metastatic disease after prior treatment.Prior treatment history matters
Researchers often specify which therapies a patient must already have received, or which therapies would make them ineligible.Overall health matters
Patients usually need enough strength, organ function, and day-to-day functioning to safely undergo the trial protocol.
Tumor biology can determine fit
At such times, patients often require the clearest guidance. Some cancers naturally produce more visible immune targets than others. The UK Markey Cancer Center's 2024 phase II trial using autogene cevumeran for pancreatic cancer reflects how targeted this work has become. Pancreatic cancer has historically been considered non-immunogenic, and pancreatic as well as bile duct cancers often require personalized antigen selection and combinatorial immunotherapy to overcome immune evasion, as described in the Markey Cancer Center overview of therapeutic vaccine trials.
In plain terms, that means a patient may not be excluded because the cancer is “too hard.” Instead, the trial may be built specifically for that kind of difficulty, with tighter biological requirements.
What side effects are usually discussed
mRNA cancer vaccine trials don't look exactly like chemotherapy in terms of side effects. Doctors often discuss immune-related symptoms such as:
- Flu-like symptoms
- Fatigue
- Injection-site reactions
- Inflammatory effects related to the partner immunotherapy
The full risk picture depends on the combination regimen, not only the vaccine.
Questions worth bringing to your appointment
Ask your oncologist these directly:
- Is my cancer type one that current mRNA vaccine trials are actively targeting?
- Would my disease be considered immunologically “hot” or “cold”?
- Would I need fresh tumor tissue or prior sequencing to be screened?
- Is the likely setting adjuvant, metastatic, or recurrence prevention?
Those answers often clarify more than hours of internet searching.
How to Find Trials and Get Expert Guidance in NYC
A family often starts the same way. Someone searches late at night, finds a trial that sounds promising, and asks, “Is this the one?” The hard part is not finding a study with the words mRNA vaccine in the title. The hard part is figuring out whether that study fits the patient sitting in front of you, with a specific cancer type, treatment history, scan pattern, and daily reality in New York City.
Online searching is a reasonable first step. It just has limits. Trial listings are written for researchers and study staff, so the words can feel like a different language. Terms such as measurable disease, progression criteria, biomarker selection, and line of therapy can change whether a trial is a real option or only looks like one on paper.
Start broad, then translate the fine print
A good search begins with national registries and patient education tools. If you want a calmer starting point before reading technical listings, exploring clinical trial resources can help you understand how studies are organized and what questions to ask.
Useful search terms include:
- Personalized cancer vaccine
- mRNA neoantigen vaccine
- Pembrolizumab combination
- Pancreatic cancer vaccine
- Melanoma vaccine trial
Those phrases help you cast a wide net. The next step is narrower and more important. Read the eligibility section line by line.
A trial title is like a book cover. It tells you the topic, not whether the story matches your case.
What to check before you invest hope in a trial
Keep a short checklist beside you as you review studies:
- Disease setting: Is the study for treatment after surgery, for recurrent cancer, or for advanced metastatic disease?
- Prior treatment rules: Some studies require certain drugs to have been tried already. Others exclude patients who have received them.
- Travel and visit schedule: Frequent visits, blood draws, and scans can be manageable for some patients and exhausting for others.
- Tissue and testing requirements: A study may require stored tumor tissue, a fresh biopsy, or a specific molecular result before screening can even begin.

Why local guidance matters in New York City
New York City gives patients access to major cancer centers, which is a real advantage. Access still needs interpretation. One oncologist or trial specialist has to compare your records with the study rules, decide whether the science fits your cancer, and weigh practical issues such as travel, timing, symptom burden, and whether a combination approach makes sense.
That last point matters in advanced cancers. An mRNA vaccine trial may be promising, but it is often only one part of the treatment plan, not the whole plan. For some patients, the right question is not “Can I get the vaccine?” It is “Does this study fit with the treatments I need now, and does it give me a realistic chance of benefit without too much disruption?”
For patients in Brooklyn and across the city, Hirschfeld Oncology is one local practice that helps patients review emerging treatment options, understand clinical trial pathways, and coordinate care discussions around advanced cancer treatment. If you want a practical overview before your visit, read this guide to cancer clinical trials for patients.
Bring records, not just interest. Trial matching depends on details such as pathology, stage, treatment dates, molecular testing, and the most recent imaging.
A simple NYC action plan
Gather the core records
Bring your pathology report, imaging reports, treatment history, and molecular testing results if you have them.Search widely, then narrow quickly
Use vaccine and mRNA terms first, then filter by cancer type, stage, and treatment setting.Ask your oncologist to review the shortlist
A trial may sound encouraging online but still be a poor fit after the inclusion and exclusion criteria are matched to your actual case.Discuss logistics as seriously as biology
In NYC, distance may look small on a map and still take hours out of a treatment day. That matters, especially if the study involves combination therapy and frequent visits.
Common Questions About mRNA Cancer Vaccines
Is this the same as a COVID vaccine
They use a related delivery method, but they are built for different jobs. A COVID vaccine teaches the immune system to recognize a virus. An mRNA cancer vaccine teaches the immune system to recognize signals linked to a person's tumor.
A simple way to picture it is this: the platform is similar, but the target is different. One is aimed at an infection from outside the body. The other is aimed at cancer cells that have learned how to hide inside it.
Can an mRNA cancer vaccine change my DNA
No. mRNA does not enter or rewrite your DNA.
It acts more like a temporary set of instructions. Cells read the message, make the protein the immune system needs to see, and then the mRNA breaks down.
Are these vaccines safe for cancer patients
Safety depends on the specific vaccine, the cancer type, and the other treatments used alongside it. That is one reason trials move in stages. Researchers first study side effects and dosing, then look more closely at whether the treatment is helping.
As noted earlier, doctors have good reason to believe mRNA can stimulate immune activity in cancer care. Still, a cancer vaccine trial is not automatically low risk just because the technology sounds familiar. Some patients do well with mild flu-like symptoms, fatigue, or soreness. Others may face added side effects from the immunotherapy, chemotherapy, or targeted drugs paired with the vaccine.
The complete risk picture depends on the full treatment plan, not just the vaccine itself.
Who pays if I join a trial
Each trial has its own rules. In many studies, the sponsor covers the investigational vaccine and some research-related testing, while standard care costs are billed through insurance in the usual way.
Ask for a written financial review before you enroll. That discussion should cover office visits, scans, lab work, travel, and what happens if you need care outside the trial schedule.
If I have an advanced cancer, should I assume this won't work for me
Advanced cancer does not rule out benefit. It does change the conversation.
For many patients with later-stage disease, the key question is whether the vaccine can strengthen a broader treatment plan. In practice, that often means combining it with checkpoint inhibitors or another systemic therapy. A vaccine may help the immune system identify the cancer, but advanced tumors often use several escape mechanisms at once. That is why combination treatment is so often part of the trial design.
Hope matters. So does realism. For a patient with advanced cancer in New York City, the best next step is usually a careful review of tumor biology, prior treatment history, symptoms, and trial logistics before deciding whether an mRNA vaccine study makes sense.
If you're in Brooklyn or elsewhere in NYC and want help understanding whether mRNA cancer vaccine trials may fit your diagnosis, Hirschfeld Oncology offers consultations focused on advanced and treatment-resistant cancers. A careful review of your records, prior therapies, and current goals can help clarify whether a trial, a combination immunotherapy plan, or another research-informed option makes the most sense for you.
.png)
.png)




