




.png)


A cancer diagnosis often drops people into a world of new words, fast decisions, and frightening uncertainty. Many patients tell me the same thing at the start: “I don't want to feel like I'm being put on a conveyor belt.” That feeling makes sense. Traditional cancer care has often relied on standard treatment pathways built around the cancer's location and stage first, then adjusted later if needed.
Modern oncology can do more than that.
Today, personalized treatment for cancer means learning as much as possible about your tumor, your body, and your day-to-day experience of treatment, then building a plan around those realities. Sometimes that means finding a drug that fits a specific mutation. Sometimes it means adjusting dose, timing, supportive medications, or monitoring so that treatment is effective and still livable. Both matter.
That second part is often overlooked. Precision medicine gets most of the attention. Precision care delivery deserves just as much. The best cancer plan isn't only the one that looks right on paper. It's the one that can be safely carried out, monitored closely, and adapted before side effects or complications take over your life.
Beyond One-Size-Fits-All Cancer Care
A patient sits in an exam room after hearing the words “advanced cancer.” Family members are texting. Questions are piling up. Is chemotherapy the only option? Will treatment feel unbearable? Is there any reason to believe this can be approached in a more thoughtful way?
That moment is where personalized care begins.

For many years, cancer treatment was organized mostly by where the cancer started. Lung cancer was treated one way. Colon cancer another. That framework still matters, but it's no longer the whole story. Two people with the same cancer type can have tumors driven by very different biological signals. They can also have very different goals, symptoms, strength levels, and tolerance for treatment.
Treating the person, not only the tumor
Personalized treatment for cancer is not one single therapy. It's a care philosophy. Your team asks several questions at once:
- What is driving this cancer biologically
- Which therapies are most likely to work against those drivers
- What can this patient realistically tolerate
- How do we preserve daily function and quality of life while treating the disease
That last question changes everything. A good plan doesn't stop at choosing a drug. It includes hydration, nausea control, fatigue management, pain support, lab monitoring, nutrition, mobility, and dose adjustment when needed.
Personalized cancer care means matching treatment to biology and matching delivery to the person living through it.
Precision care delivery matters
Recent data shows that functional indicators like gait, balance, and activity patterns can predict emerging risks before symptoms become severe, enabling earlier intervention, according to NCODA's discussion of personalized care delivery in oncology. That idea is simple but powerful. If a patient's movement, stamina, or daily activity starts changing, the care team may spot trouble before a crisis develops.
This is the part many patients find reassuring. Personalization doesn't only happen in the lab. It happens during the weeks and months of treatment, when your body tells us how the plan is working in real life.
How We Map Your Cancer's Unique Blueprint
Before choosing a personalized treatment, we need a map. Not a rough sketch. A detailed one.
Cancer cells carry clues about what helps them grow, what makes them vulnerable, and which medicines may be useful. The job of testing is to collect those clues carefully, then turn them into a treatment strategy.
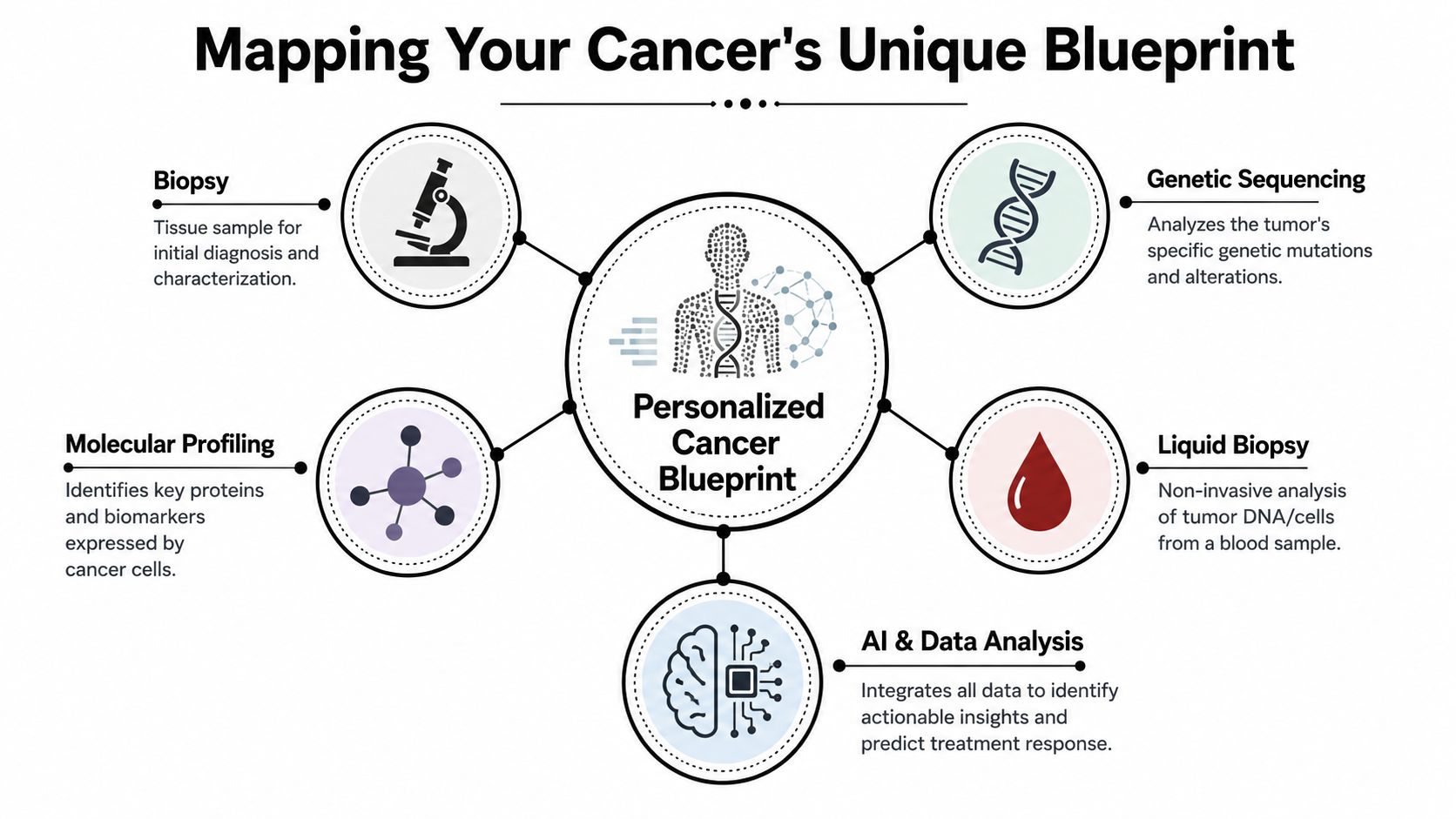
The main pieces of the map
Think of this as detective work.
A biopsy gives the starting sample. Pathologists study the tissue under a microscope to confirm what kind of cancer it is. After that, more detailed testing may look for features that don't show up on routine pathology alone.
Molecular profiling studies the tumor's internal makeup. It can identify changes in DNA, RNA, proteins, or other markers that may guide treatment. If you want a plain-language overview, this guide to molecular testing for cancer is a useful place to start.
A biomarker is a measurable sign that may point toward a treatment option. Some biomarkers suggest a targeted therapy. Others may make immunotherapy more relevant. Some show that a treatment is unlikely to help, which is also valuable information.
A liquid biopsy looks for tumor material in the blood. It doesn't replace every tissue biopsy, but it can sometimes help monitor the cancer over time and look for changes that emerge during treatment.
Why this testing matters
The point of all this testing isn't to produce a thicker file. It's to make decisions with more precision.
A meta-analysis involving over 13,000 patients found that personalized oncology treatments produced response rates over 30%, compared with 5% in non-personalized approaches, and that matched treatments were associated with median progression-free survival of 5.7 months versus 2.95 months for standard therapy, as reported in this review of personalized oncology outcomes.
That doesn't mean every patient will have a targetable finding. It also doesn't mean every target has a perfect drug. What it does mean is that careful mapping can uncover options that would otherwise be missed.
| Test approach | What it helps answer |
|---|---|
| Tissue biopsy | What cancer is this, and what does it look like under the microscope? |
| Molecular profiling | Which genetic or molecular changes may be driving growth? |
| Biomarker testing | Is there a known treatment target or resistance signal? |
| Liquid biopsy | Is the cancer changing over time, and can we monitor that through blood? |
Practical rule: The best treatment choice usually comes after the best diagnostic work, not before it.
Modern Treatments Tailored to Your Biology
Once we understand the tumor's blueprint, treatment choices become more strategic.
Traditional chemotherapy can still be important. Surgery and radiation still matter. Personalized treatment for cancer doesn't replace those tools across the board. It changes how we decide when to use them, how intensely to use them, and what else to combine with them.

Targeted therapy and immunotherapy
A targeted therapy is designed to interfere with a specific pathway the cancer relies on. I often describe it as a more selective strike. It isn't magic, and it can still cause side effects, but the goal is to hit a vulnerability that's more specific to the cancer.
An immunotherapy works differently. Instead of acting directly on the cancer cell alone, it helps the immune system recognize or attack the disease more effectively. In the right setting, that can be very powerful.
Patients often read these terms and assume one is always gentler than chemotherapy. That's not always true. The key question is fit. A treatment is only “better” if it matches the biology and can be tolerated.
Combinations and dose strategy
Some cancers need pressure from more than one angle. That's where combinations come in. A team may pair targeted drugs, combine systemic treatment with local treatment, or use a lower-dose strategy that allows treatment to continue more steadily.
This point is especially important for people with advanced or treatment-resistant disease. In the I-PREDICT trial, 46% of patients with treatment-resistant cancers who received multi-drug regimens matched to their tumor's mutations had an objective response, and the report notes that low-dose, ramp-up dosing strategies often helped minimize toxicity, according to the UC San Diego summary of I-PREDICT.
That idea deserves plain language. Starting lower and increasing carefully isn't “giving less care.” Sometimes it's the smartest way to keep a treatment safe enough for a real person to stay on it.
You can read more about how targeted therapy fits into modern cancer care if your doctor has mentioned that option.
A simple comparison
- Traditional chemotherapy: Often affects fast-growing cells broadly. It can be effective, but it may also affect healthy cells that divide quickly.
- Targeted therapy: Aims at a specific molecular feature the cancer depends on.
- Immunotherapy: Helps the immune system respond to the cancer.
- Cell-based or gene-directed approaches: Used in selected situations, usually when the cancer type and clinical setting make them appropriate.
The strongest treatment plan is not always the harshest one. It's the one that hits the cancer well enough while keeping the patient strong enough to continue.
How Your Care Plan Becomes Truly Individualized
A lab report alone doesn't create a treatment plan. People do.
The most thoughtful personalized cancer care comes from combining test results with clinical judgment. That means experienced physicians, pathologists, genetics experts, pharmacists, and other specialists looking at one patient's case together and asking, “What makes sense here, for this person, right now?”
The role of the molecular tumor board
A molecular tumor board is a group of specialists who review complex cases and interpret genomic findings in clinical context, as a mutation on paper doesn't automatically answer every treatment question. Experts still need to weigh how meaningful that result is, what drug options exist, whether combinations make sense, and what risks deserve caution.
That team approach has been linked with better matching of treatment to disease biology. A significant study reported that patients whose treatment was highly matched by a molecular tumor board had a three-year survival rate of 55%, compared with 25% for patients with low-matched or unmatched therapies, according to this UC San Diego report on personalized cancer therapy in advanced disease.
What individualization looks like in daily care
The individualized part doesn't end when the board makes a recommendation.
Here's what personalized care delivery often includes:
- Dose adjustment based on tolerance so treatment remains effective without overwhelming the patient
- Side effect prevention using anti-nausea plans, hydration, blood count support, skin care, bowel management, or pain control
- Schedule changes when timing needs to fit recovery patterns, work, caregiving, or travel realities
- Response monitoring through symptoms, scans, labs, and sometimes blood-based tools
- Goal-based decisions that respect whether a patient is prioritizing time, symptom relief, function, or aggressive disease control
Some patients need a plan that pushes harder. Others need one that preserves strength first so they can stay in treatment longer. Neither is “less serious.” Both are forms of careful oncology.
A good care plan is dynamic. If neuropathy worsens, if appetite collapses, if fatigue changes walking stability, the plan should change too. That's not failure. That's precision.
Your Personalized Treatment Pathway Explained
For most patients, the hardest part is not the science. It's the uncertainty about what happens next.
A personalized cancer pathway usually unfolds in stages. The details vary by cancer type, prior treatment, and urgency, but the overall sequence is more understandable when you see it as a series of decisions rather than one giant leap.
A visual overview can help make that pathway easier to follow.
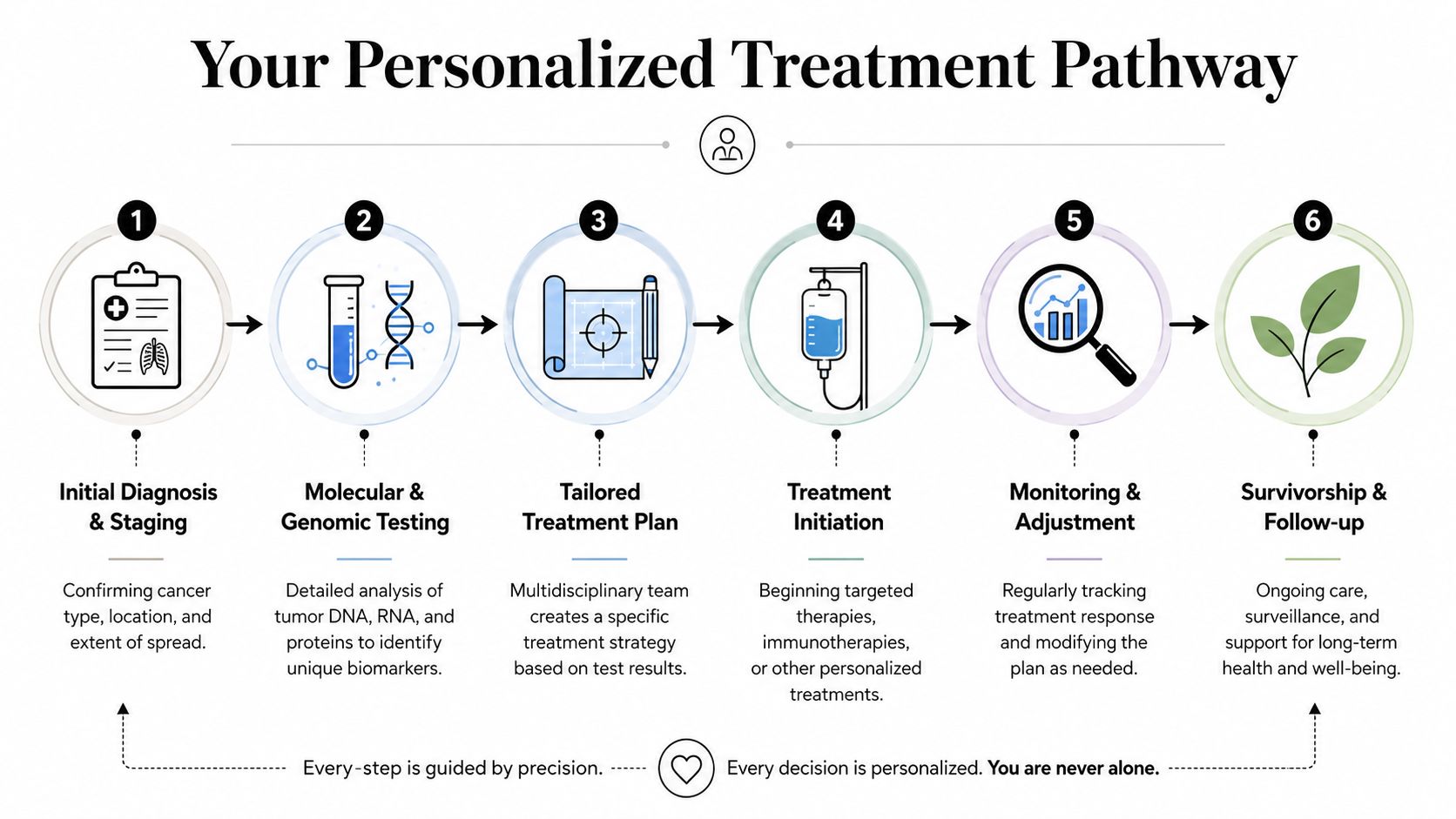
Step by step in real life
Diagnosis and staging
The team confirms the cancer type, where it started, and whether it has spread. This creates the medical baseline.Molecular and biomarker testing
Tissue or blood testing looks for features that may open the door to targeted therapy, immunotherapy, or a clinical trial.Expert review and plan design
The oncologist, and in some cases a tumor board, decides what treatment approach best fits the biology and the patient's overall condition.Treatment starts
This may involve targeted therapy, immunotherapy, chemotherapy, or a combination. Supportive medications are often added from day one.Close monitoring
The team watches not only the cancer response but also fatigue, appetite, pain, bowel function, neuropathy, and activity level.Adjustment over time
If the cancer changes or the side effects become too heavy, the plan is revised rather than followed blindly.
Later in the journey, some patients also benefit from educational resources like this video, which explains precision oncology in patient-friendly terms.
A pancreatic cancer example
Pancreatic cancer is a good example of why this process matters. On the surface, two patients may appear to have the same disease. Underneath, the biology may point in different directions.
For pancreatic cancer patients with certain biomarkers, personalized treatment can produce very different options. MSI-high tumors have shown a 60% response rate to immunotherapy compared with 5% with chemotherapy, and emerging KRAS G12C inhibitors have shown a 37% response rate in previously treated patients, according to this review of personalized cancer care techniques in pancreatic cancer.
If a patient has one of those findings, the pathway changes. The discussion becomes more specific. Which therapy fits that marker? What side effects are likely? How closely should we monitor? Can the patient tolerate the plan?
The pathway isn't just about finding a drug. It's about building a sequence of decisions that can adapt as the patient's situation changes.
A Practical Guide for Navigating Your Journey
Patients and families often worry that they need to become cancer experts overnight. You don't. But you do need a few good questions.
The right questions can change the quality of the discussion in the room. They help you understand whether your care is being individualized in a meaningful way or whether you're being moved through a standard pathway without enough review.
Questions worth asking your oncologist
- About testing: Has my tumor had molecular profiling or biomarker testing, and if not, should it?
- About fit: Are there targeted therapy or immunotherapy options that match my cancer's features?
- About interpretation: Is my case being reviewed by a molecular tumor board or another multidisciplinary team?
- About tolerability: If a treatment is promising but side effects are a concern, how would you adjust dose or schedule?
- About monitoring: What signs would tell us early that the treatment is helping, not helping, or becoming too hard on me?
- About goals: Is this plan aimed mainly at shrinking disease, controlling symptoms, extending disease control, or balancing several goals at once?
- About trials: Are there clinical trials that make sense for my cancer biology and treatment history?
These aren't confrontational questions. They're partnership questions.
What patient-centered care should feel like
When care is personalized, you should feel that your team is paying attention to more than scan dates.
Look for signs like these:
| What to notice | Why it matters |
|---|---|
| Your symptoms are reviewed in detail | Side effects often guide whether treatment should continue as planned or be adjusted |
| Your daily function is discussed | Walking, eating, sleeping, and energy tell us how your body is handling treatment |
| Your goals are asked about directly | Different patients define a good outcome differently |
| The plan is revisited regularly | Good oncology care adapts rather than staying rigid |
If travel is part of your care burden, practical support matters too. Families who need transportation help for treatment at a distance may want to review resources for aid for distant medical care, which can be relevant when specialized oncology services aren't close to home.
In New York City, one example of a practice built around personalized regimens, infusion care, close monitoring, and collaborative decision-making is Hirschfeld Oncology. That kind of setting may be worth asking about if you're looking for outpatient care that focuses on complex or treatment-resistant disease while paying attention to tolerability and quality of life.
When to seek another opinion
A second opinion is especially reasonable when:
- Standard treatment has stopped working
- Your cancer is advanced or unusual
- You've never had genomic or biomarker testing
- You're being offered treatment but not hearing a plan for side effect management
- You feel rushed into decisions without understanding alternatives
A second opinion doesn't mean you're rejecting your current doctor. It means you're being thorough.
Finding Advanced Cancer Care in New York City
Personalized treatment for cancer is no longer an abstract idea reserved for academic discussions. It's part of real-world cancer care now. The most effective modern approach combines detailed tumor mapping, thoughtful treatment matching, and careful day-to-day management of symptoms, dosing, and quality of life.
That combination matters most in advanced and treatment-resistant disease, where standard pathways may not be enough. Patients often need a team that can look beyond first-line options, interpret complex testing, and adapt the plan as the body responds.
For patients in Brooklyn and nearby neighborhoods such as Williamsburg and Bushwick, access to this kind of care can make the process feel more manageable. If you're comparing options locally, this overview of a Brooklyn cancer center may help you understand what to look for in an outpatient setting.
The most important message is simple. You are not limited to asking, “What's the standard treatment?” A better question is, “What treatment fits my cancer biology, my health, and my life?” That's often where new options begin.
If you want to explore a more individualized approach, Hirschfeld Oncology offers information on personalized oncology care, infusion treatment, and options for people facing advanced or treatment-resistant cancers. A consultation can help clarify what testing, treatment strategies, and supportive care approaches may fit your specific situation.
.png)
.png)




