




.png)


A New Era in Bile Duct Cancer Treatment
Cholangiocarcinoma, a rare bile‑duct malignancy, accounts for roughly 3 % of gastrointestinal cancers and carries a 5‑year survival of less than 30 % when diagnosed at an advanced stage. Its heterogeneity— intratrahepatic, perihilar and distal subtypes—creates distinct molecular landscapes, with actionable alterations such as FGFR2 fusions (≈10‑15 %), IDH1 mutations (≈13‑20 %) and HER2 amplification (≈5‑10 %). Because only a minority of patients benefit from standard gemcitabine‑cisplatin, NCCN and ASCO guidelines now mandate comprehensive genomic profiling to match patients to FGFR, IDH1, HER2, BRAF, KRAS or NTRK‑targeted agents or immunotherapy. Hirschfeld Oncology embraces this precision‑medicine model: its multidisciplinary tumor board orders next‑generation sequencing for every advanced case, enrolls eligible patients in early‑phase trials (e.g., FGFR inhibitors plus chemotherapy or pembrolizumab‑based combos), and monitors resistance using liquid‑biopsy ctDNA. By integrating molecular data, targeted drugs, and supportive services, Hirschfeld Oncology exemplifies the personalized approach needed to improve outcomes in bile‑duct cancer.
Molecular Profiling: Mapping the Cancer’s Blueprint
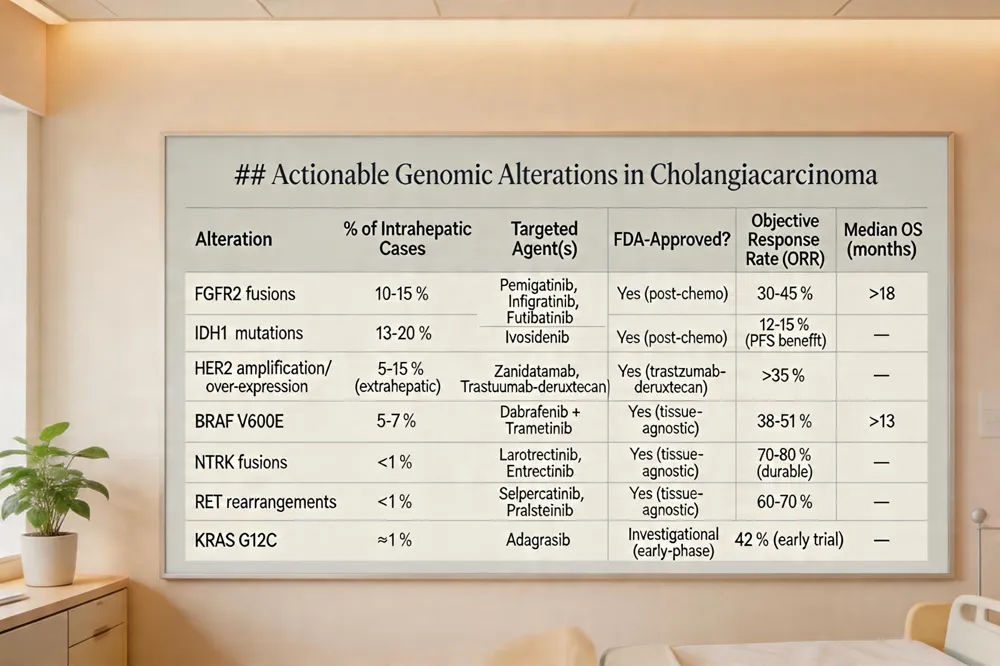 Comprehensive next‑generation sequencing (NGS) of tumor tissue—or circulating tumor DNA—has become a standard of care for all patients with advanced cholangiocarcinoma, as mandated by NCCN 2024 guidelines. This profiling uncovers actionable alterations in up to 40 % of cases. FGFR2 gene fusions present in 10‑15 % of intrahepatic tumors, predict sensitivity to FGFR inhibitors such as pemigatinib, infigratinib, and futibatinib, which have demonstrated objective response rates of 30‑45 % and median overall survival exceeding 18 months in real‑world analyses. IDH1 mutations occur in roughly 13‑20 % of intrahepatic disease; the oral inhibitor ivosidenib improves progression‑free survival (median 2.7 months versus 1.4 months placebo) and is FDA‑approved after chemotherapy failure. HER2 amplification or over‑expression, identified in 5‑15 % of extrahepatic cholangiocarcinomas, is targetable with bispecific antibodies (zanidatamab) and antibody‑drug conjugates (trastuzumab‑deruxtecan), yielding response rates above 35 %. BRAF V600E mutations (≈5‑7 %) respond to combined dabrafenib‑trametinib, achieving response rates of 38‑51 %. Rare NTRK fusions (<1 %) and RET rearrangements are actionable with larotrectinib, entrectinib, selpercatinib, and pralsetinib. KRAS G12C mutations, though uncommon (~1 %), can be inhibited by adagrasib, which has shown 42 % response in early trials. Routine NGS testing thus guides selection of these genotype‑matched therapies and enrollment in clinical trials, enabling a precision‑medicine approach to bile duct cancer.
Targeted Therapies – The Miracle‑Like Drugs
 Bile‑duct (cholangiocarcinoma) cancer is not cured by a single drug, but several precision medicines act like "miracle" agents when matched to a tumor’s molecular profile.
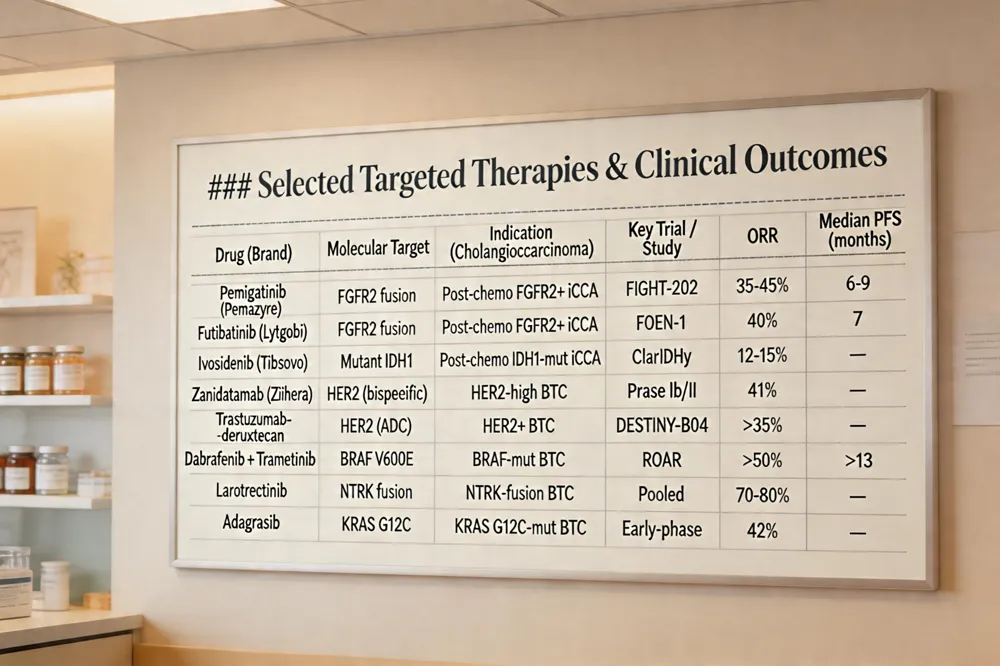
FGFR2 inhibitors – [FGFR2 gene fusions] (https://pmc.ncbi.nlm.nih.gov/articles/PMC8650725/) occur in ~10‑15 % of intrahepatic cholangiocarcinoma. FGFR2 inhibitors such as pemigatinib (Pemazyre) and futibatinib (Lytgobi) are FDA‑approved after prior chemotherapy and achieve objective response rates of 35‑45 % with median progression‑free survival of 6‑9 months.
IDH1 inhibitor – Mutant IDH1 is present in ~13‑20 % of intrahepatic disease. Ivosidenib (Tibsovo) blocks the mutant enzyme and prolongs progression‑free survival (median 2.7 months vs 1.4 months, ClarIDHy) with a favorable safety profile.
HER2‑directed agents – [HER2 amplification/over‑expression occurs] (https://pmc.ncbi.nlm.nih.gov/articles/PMC8650725/) in 5‑15 % of extra‑hepatic cholangiocarcinoma. The bispecific antibody zanidatamab (Ziihera) binds two HER2 epitopes, achieving a 41 % overall response rate in HER2‑high biliary tract cancers after standard therapy.
TRK inhibitors – Though rare (<1 %), NTRK fusions are targetable with larotrectinib or entrectinib, which have tissue‑agnostic FDA approvals and produce durable responses. TRK inhibitors
BRAF/MEK inhibitors – [BRAF V600E mutations] (https://www.cancer.org/cancer/types/bile-duct-cancer/treating/targeted-therapy.html) (≈5‑7 %) respond to dabrafenib plus trametinib, yielding response rates >50 % and median overall survival >13 months.
KRAS G12C inhibitors – [KRAS G12C inhibitor] (https://www.cancer.org/cancer/types/bile-duct-cancer/treating/targeted-therapy.html) adagrasib shows a 42 % response rate in biliary tract cancers.
Emerging bispecific antibodies – Agents such as zenocutuzumab (targeting HER2/HER3) and zanidatamab exemplify the next wave of bispecific therapeutics, expanding options for rare genomic subtypes.
These targeted drugs, selected through comprehensive genomic profiling, constitute the most promising "miracle‑like" advances in bile‑duct cancer today.
Immunotherapy and Combination Regimens
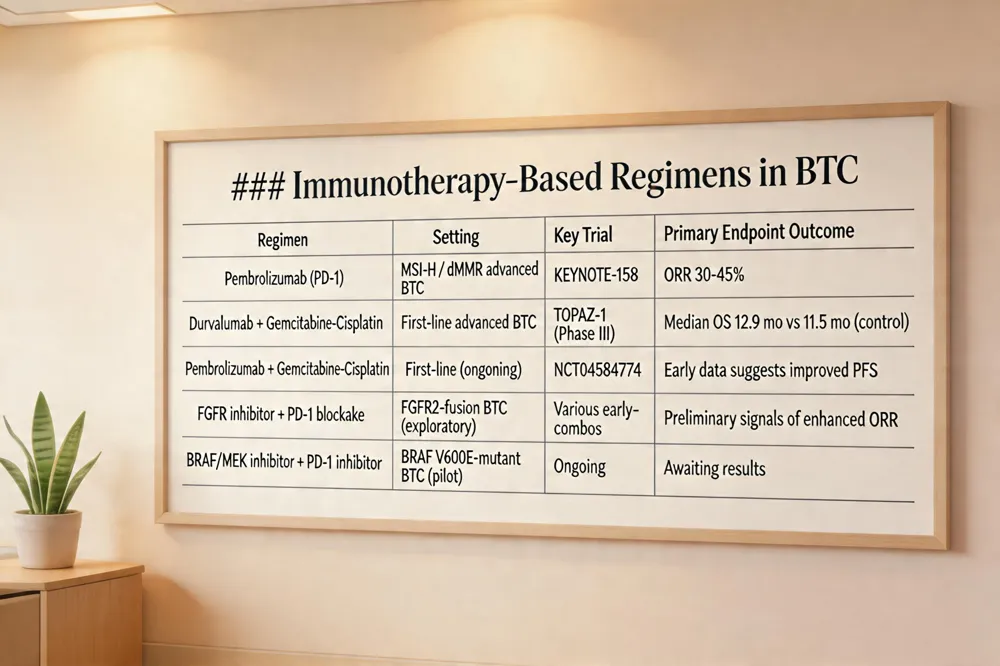 PD‑1/PD‑L1 checkpoint inhibitors have emerged as a pivotal component of biliary tract cancer (BTC) therapy, especially for tumors with high microsatellite instability (MSI‑H) or mismatch‑repair deficiency (dMMR), where pembrolizumab yields response rates of 30‑45 %. In the first‑line setting, the PD‑L1 inhibitor durvalumab combined with gemcitabine‑cisplatin has become a new standard after the TOPAZ‑1 phase III trial demonstrated a statistically significant overall‑survival benefit (median 12.9 months vs 11.5 months). Ongoing investigations such as NCT04584774 are evaluating pembrolizumab plus chemotherapy to further improve outcomes. Moreover, early‑phase studies are pairing FGFR inhibitors (e.g., pemigatinib or infigratinib) with PD‑1 blockade to overcome resistance and enhance response durability. These combination strategies reflect a shift toward integrated immuno‑targeted regimens in advanced cholangiocarcinoma.
Survival, Disease Spread, and Curability
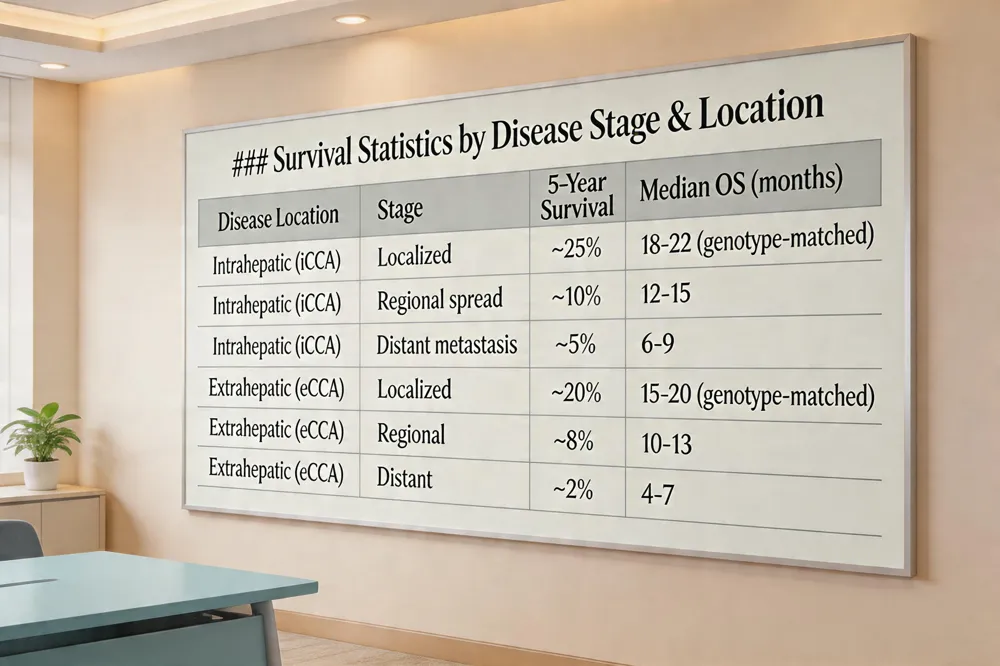 Can you survive bile duct cancer? Yes—survival depends on stage, location, and treatment. Intrahepatic cholangiocarcinoma (iCCA) has a 5‑year survival of ~25 % when disease is localized, dropping to ~10 % for regional spread and ~5 % for distant disease. Extrahepatic disease fares slightly better when localized (~20 %) but falls to ~2 % with metastasis. Multidisciplinary care, early surgical resection when possible, and modern systemic options—including FGFR2 and IDH1 inhibitors, HER2‑directed agents, and chemo‑immunotherapy—extend outcomes, with real‑world data showing median overall survival of 18–22 months for patients receiving genotype‑matched therapy versus 9–10 months on chemotherapy alone.
How fast does bile duct cancer spread? Cholangiocarcinoma is aggressive, often advancing from localized disease to regional lymph‑node involvement within weeks to a few months. Tumor invasion of the thin bile‑duct wall enables rapid entry into hepatic vasculature, leading to distant metastases (lungs, bone) if untreated. Early detection and multimodal therapy can slow this progression, but without treatment the disease typically disseminates quickly.
Is stage 3 bile duct cancer curable? Stage 3 is usually advanced and frequently unresectable; curative surgery is only possible in a minority of cases where the tumor remains resectable. Even when resection is feasible, adjuvant chemotherapy or radiation is needed. For most stage 3 patients, treatment is palliative, aiming to shrink tumor, prevent further spread, and improve quality of life.
Why is bile duct cancer so aggressive? The tumor often grows undetected, rapidly breaches the duct wall, and exploits the liver’s rich vascular network for early hematogenous and lymphatic spread. Its silent clinical presentation and lack of effective screening contribute to late diagnosis, while molecular subtypes such as FGFR2 fusions or IDH1 mutations drive proliferative and anti‑apoptotic pathways, further increasing its lethal potential.
Choosing the Best Center for Care
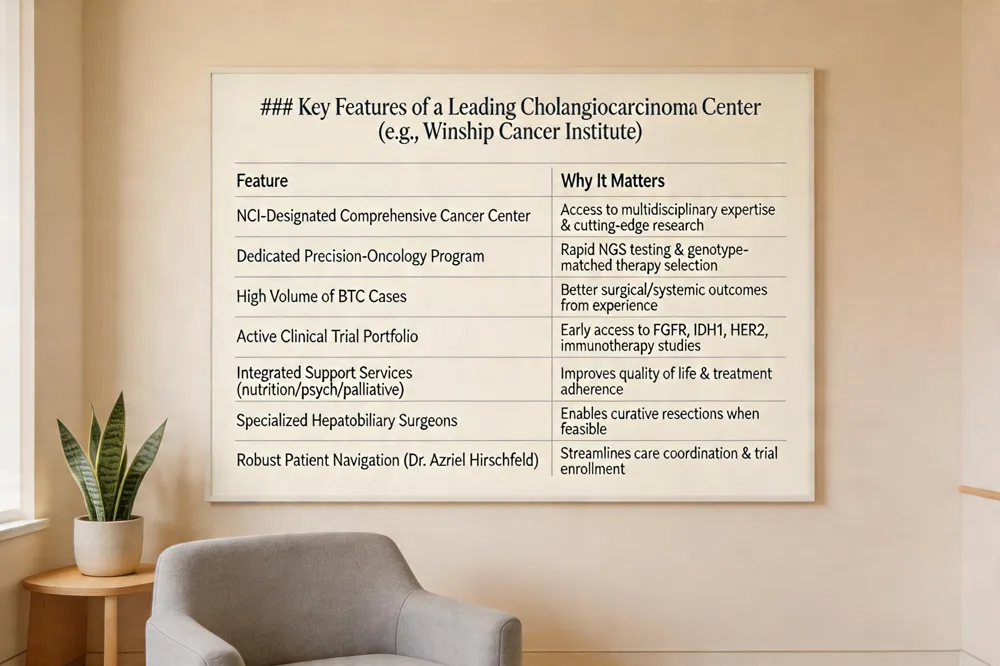 The Winship Cancer Institute of Emory University is widely regarded as the leading U.S. hospital for bile duct (cholangiocarcinoma) cancer. As Georgia’s only National Cancer Institute‑designated Comprehensive Cancer Center, Winship offers unparalleled medical, surgical, and radiation expertise, treating more cholangiocarcinoma cases than any other state center. Its multidisciplinary teams—medical oncologists, hepatobiliary surgeons, interventional radiologists, pathologists, and supportive‑care specialists—collaborate to develop individualized, evidence‑based treatment plans. Patients benefit from rapid access to cutting‑edge clinical trials, including FGFR‑, IDH1‑, and HER2‑targeted studies, often coordinated through dedicated precision‑oncology programs. Dr. Azriel Hirschfeld’s practice exemplifies this model, integrating next‑generation sequencing, targeted‑therapy selection, and compassionate navigation of trial enrollment. Robust patient‑advocacy resources at Winship further empower individuals to understand options, manage side effects, and connect with support networks, ensuring comprehensive, state‑of‑the‑art care.
Looking Forward: A New Horizon
Integrating targeted therapy into multidisciplinary care for cholangiocarcinoma is reshaping outcomes. FGFR2, IDH1, HER2, BRAF and emerging agents such as NTRK and KRAS‑G12C inhibitors are matched after routine next‑generation sequencing, enabling combos with gemcitabine‑cisplatin or immunotherapy to counter resistance. Future trials will test next‑generation FGFR inhibitors, antibody‑drug conjugates, bispecific antibodies and liquid‑biopsy‑guided adaptive strategies, aiming for durable responses and earlier‑line use. For patients, these advances mean longer survival, oral options, and renewed optimism that precision medicine can turn a fatal disease into a treatable condition. Clinicians and researchers remain committed to expanding access and equity for all patients worldwide today.
.png)
.png)




