




.png)


If you're reading about 3000 mg vitamin C, you're probably trying to answer a practical question, not win an argument on the internet. You may be in treatment, recovering from treatment, or caring for someone with cancer and looking for options that feel less toxic, more supportive, or more aligned with quality of life. High-dose vitamin C comes up often in that search.
In clinic, I see the same pattern again and again. A patient hears that vitamin C is “natural,” then hears that some oncology practices use IV vitamin C, then finds a bottle online that offers large oral doses and wonders whether that gets them to the same place. That confusion is understandable. The words sound similar. The biology is not.
The most helpful way to approach this topic is with calm precision. A 3000 mg oral dose has a very different meaning from high-dose IV vitamin C given in a monitored medical setting. Some patients may still decide oral supplementation has a place in their routine. Others may decide it isn't worth the side effects or false hope. In oncology, the right answer usually depends on the goal, the patient's risk profile, and how the therapy fits with the larger treatment plan.
Why Patients Ask About 3000 mg Vitamin C
Individuals do not typically inquire about 3000 mg vitamin C out of casual curiosity. Their questions arise from a desire to assist themselves in circumstances that feel urgent. Cancer pushes people to search beyond standard labels. They want something active, something they can do today.
Sometimes the question starts with fatigue. A patient feels depleted during chemotherapy, starts looking into nutrition and supplements, and quickly lands on vitamin C. In that stage, it can help to look at broader symptom-oriented resources on matching supplements to fatigue symptoms, because fatigue is often multifactorial and not automatically a sign that more vitamin C is the answer.
The hope behind the question
In an oncology setting, I rarely hear this question as a purely nutritional question. I hear it as a deeper one.
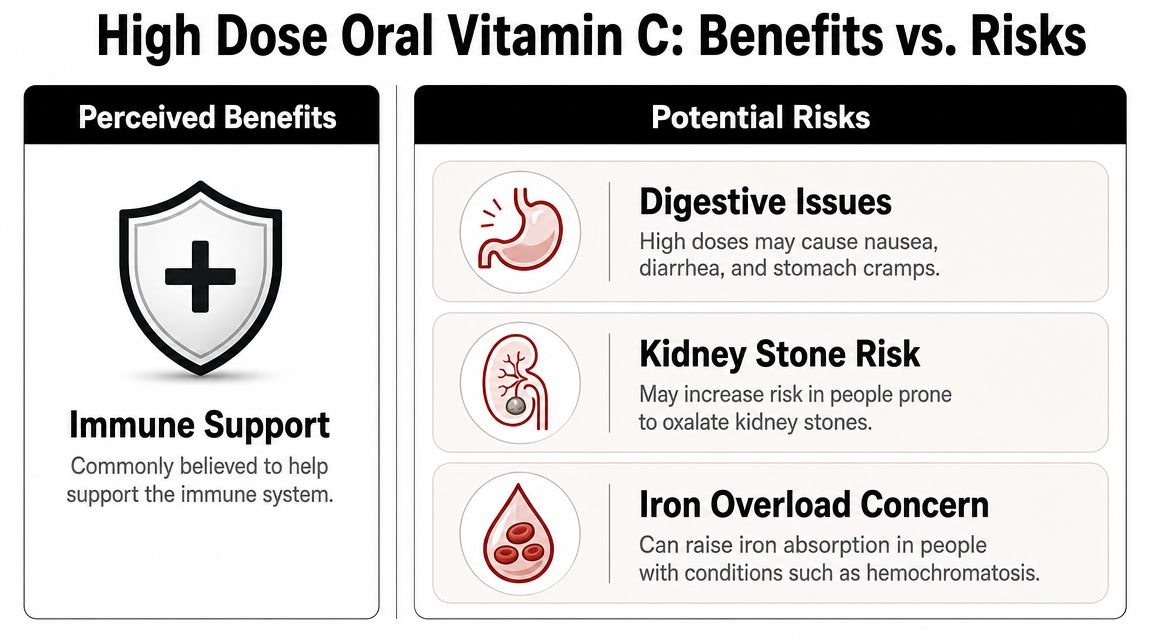
- “Could this support my immune system?” Patients often want to feel less vulnerable during treatment.
- “Could this make treatment easier to tolerate?” That usually means less fatigue, less brain fog, or faster recovery.
- “Could this help fight the cancer itself?” This is the part many people are hesitant to say out loud, but it's often present.
Patients aren't wrong to ask. They're trying to separate a hopeful idea from a useful one.
Why the online answers often feel incomplete
Most online discussions stop at a single point: 3000 mg is above the usual upper limit, therefore don't do it. That answer is partly true, but it leaves out the part patients care about. They want to know whether a large oral dose changes anything meaningful, and whether it relates in any real way to the IV vitamin C used in some integrative oncology clinics.
That missing nuance matters. A person in active cancer care doesn't need vague encouragement or blanket dismissal. They need a clear explanation of what an oral dose can do, what it can't do, and when medical supervision changes the equation.
What a 3000 mg Oral Dose Means for Your Body
A patient in clinic will sometimes hold up a bottle labeled 3000 mg and ask a very reasonable question: if the number is that high, should it do something meaningful? In practice, that dose usually creates more questions about absorption and tolerance than clear evidence of added benefit.
A 3000 mg oral dose sits well above the usual upper intake limit for adults. It also goes far beyond what the body needs to prevent deficiency. That matters because once you move into this range, the issue is less "am I getting enough vitamin C?" and more "what happens to the extra amount?"
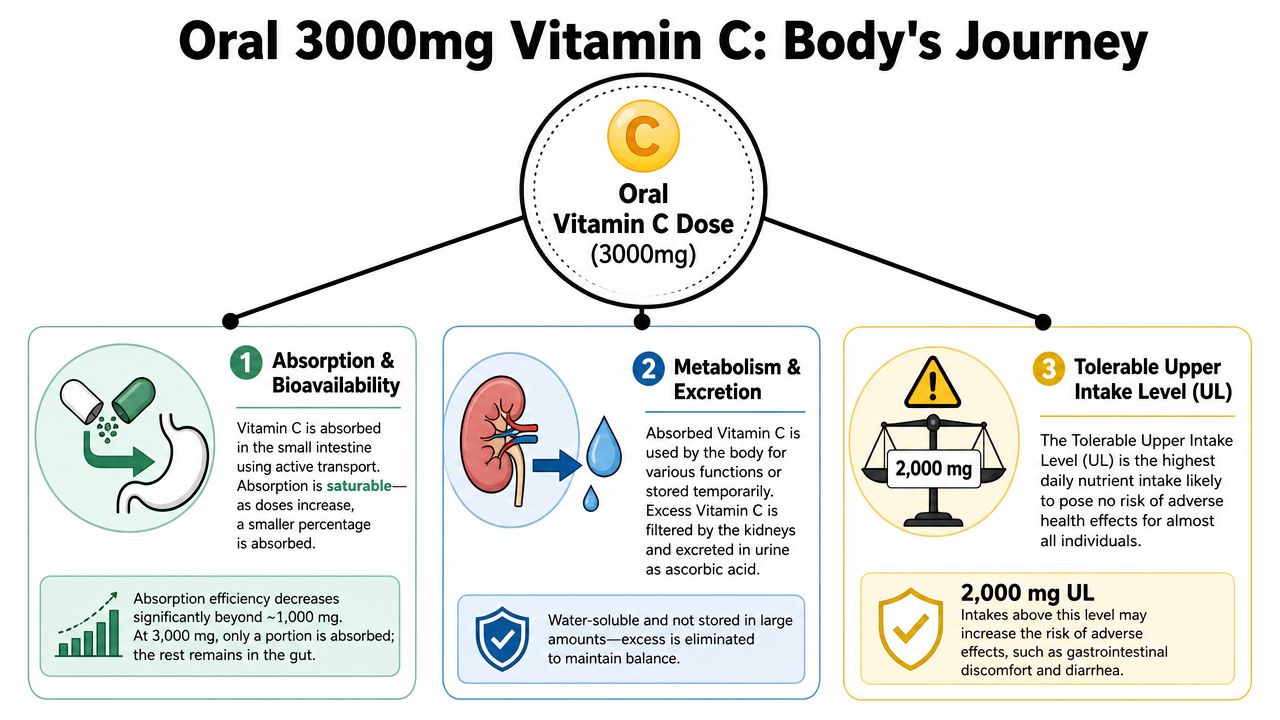
Your gut has a limit
Oral vitamin C absorption works well up to a point, then becomes less efficient as the dose rises. By the time someone swallows 3000 mg at once, the body does not fully transfer all of that dose into the bloodstream. A meaningful portion stays in the intestine, which is one reason loose stools, cramping, nausea, and bloating are so common with larger doses.
This is the practical trade-off I want patients to understand. A bigger oral dose can increase side effects without producing a proportional increase in useful blood levels.
That is why some people take 3000 mg and notice very little except GI irritation.
What patients usually notice
In clinic, large oral doses tend to lead to one of three real-world outcomes:
- No clear difference: energy, immunity, or treatment tolerance do not change in an obvious way
- Digestive side effects: the gut becomes the limiting factor before any meaningful benefit is felt
- Confusion about purpose: the dose sounds therapeutic, so patients assume it behaves like medically supervised vitamin C treatment, which it does not
That last point causes a lot of anxiety. The label on a supplement bottle can make an oral dose sound more potent than it is.
For general supplement framing, some readers may find this overview of vitamin C for health-conscious adults useful. In cancer care, though, the decision is narrower and more clinical. The question is not whether vitamin C is popular or marketed aggressively. The question is whether this dose fits your diagnosis, kidney function, treatment plan, and actual goal.
Food often deserves more attention than another large capsule. If eating has become difficult during treatment, a practical nutrition plan may matter more than escalating supplements. Hirschfeld Oncology has a useful guide on what to eat during chemotherapy that speaks to that day-to-day reality.
Practical rule: If you cannot name the specific problem a 3000 mg dose is supposed to solve, it is worth pausing before you keep increasing it.
Oral Pills vs IV Infusion Which Is Better
A patient in clinic will often hold up a bottle labeled 3000 mg and ask whether it is basically the same thing as the IV vitamin C offered at some cancer centers. It is a fair question. The two routes can sound similar on paper, but in practice they serve different purposes and belong in different clinical conversations.
Oral vitamin C is a supplement route. IV vitamin C is an infusion therapy route. In oncology, that difference matters more than the number on the label.
An oral dose has to pass through the gut, and the body limits how much ultimately reaches the bloodstream. An IV infusion bypasses that step and produces blood levels that oral capsules cannot match. That is why a large pill does not function like an infusion protocol, even if the milligram number looks impressive.
Why route matters in real oncology care
In my clinic, the decision is rarely "which one is stronger?" The useful question is, "What are we trying to accomplish?"
If the goal is ordinary nutritional support, oral supplementation may be reasonable, though 3000 mg is often more than is needed. If the goal is a medically supervised adjunct that aims for pharmacologic blood levels, oral dosing is the wrong tool. Patients and families often blur those two goals together. Once you separate them, the discussion gets much clearer.
Route also changes the practical burden. A pill is easy to buy and take at home. An infusion requires screening, scheduling, venous access, cost discussion, and coordination with the oncology plan. It also raises treatment-specific questions about timing, expected benefit, and whether antioxidants fit the regimen. Hirschfeld Oncology reviews some of that broader context in this discussion of antioxidants and cancer treatment decisions.
Oral Vitamin C vs. IV Vitamin C at a Glance
| Feature | Oral Vitamin C (e.g., 3000 mg pill) | IV Vitamin C (High Dose) |
|---|---|---|
| Absorption route | Through the digestive tract | Directly into the bloodstream |
| Main limitation | Limited delivery into circulation at high doses | Requires medical screening and supervision |
| Achievable blood levels | Modest compared with infusion | Far higher than oral dosing can provide |
| Typical setting | Home use | Infusion clinic or medical office |
| Primary role | Supplement use | Possible adjunctive use in selected oncology settings |
| Most common practical issue | Patients expect a treatment effect from a supplement dose | Choosing the right patient, timing, and clinical goal |
Which is better
"Better" depends on the target.
For replacing a deficiency or covering a basic nutritional gap, oral vitamin C is usually the simpler option. For patients asking about high-dose vitamin C as part of cancer care, the topic is usually IV therapy, because that is the route used when clinicians are trying to reach blood concentrations that supplements cannot produce.
That does not make IV vitamin C automatically useful. It means the question shifts from supplement advice to treatment selection. At that point, I want to know the diagnosis, current drugs, kidney function, stone history, and what the patient hopes will improve. Without that context, comparing a 3000 mg pill with an IV infusion is like comparing two interventions that happen to share a name.
Understanding the Risks of High Dose Vitamin C
For most adults, the immediate problem with 3000 mg oral vitamin C isn't classic poisoning. It's tolerance. The body often tells you fairly quickly when the dose is too high for your gut.
At 3000 mg/day, oral vitamin C can cause osmotic gastrointestinal intolerance, including diarrhea and nausea, because unabsorbed ascorbate draws water into the intestine. It can also raise urinary oxalate, and doses above 1000 mg/day have been linked to an increased risk of recurrent kidney stones in susceptible people, as summarized in this clinical overview of vitamin C safety.
The common risk is the gut
In practice, the most predictable side effects are gastrointestinal.
- Diarrhea: A classic sign that more is staying in the bowel than being absorbed.
- Nausea: Often dose-related and sometimes worse when taken on an empty stomach.
- Abdominal cramping or heartburn: These symptoms don't make the dose “effective.” They usually mean the opposite. Your body isn't handling it well.
The more important risk is patient-specific
Kidney stone risk is where high-dose vitamin C stops being a simple comfort issue and becomes a screening issue. Not every person who takes a large dose will form a stone. But in someone with a prior stone history, impaired kidney handling, or other susceptibility, the risk profile changes.
That matters in oncology because patients may already be dealing with dehydration, altered nutrition, changing renal function, and multiple medications. A supplement that looks benign on a store shelf can become less benign in a patient whose physiology is already under strain.
For a broader cancer-care discussion of timing and caution around antioxidant use, this overview of antioxidants and cancer is worth reading.
High-dose supplements should be judged in the context of the patient taking them, not in the abstract.
What doesn't work well as a decision rule
Many people use “it's water-soluble” as the entire safety argument. That's incomplete. Water-soluble doesn't mean consequence-free. It means the body has ways to eliminate excess. The gut and kidneys are part of that story, and they're often where the trade-offs show up first.
A more reliable rule is simpler: if the dose is high enough to exceed normal safety ceilings and produce predictable side effects, it deserves the same respect as any other medical decision.
Reviewing the Evidence for Vitamin C in Oncology
In oncology, vitamin C becomes more interesting and more complicated. The conversation is no longer just about preventing deficiency or supporting general wellness. It becomes a question of whether high-dose IV vitamin C might have a role as an adjunct to conventional care in selected patients.

Why oncology clinics discuss IV and not 3000 mg pills
In real-world oncology practice, when clinicians consider vitamin C seriously, they're generally not talking about oral 3000 mg regimens. They're discussing IV therapy because that route can achieve blood concentrations oral dosing cannot.
That distinction is the foundation for the whole oncology conversation. If a patient asks whether a large oral dose “does the same thing” as an infusion, the practical answer is no.
The theory clinicians consider
At pharmacologic concentrations, vitamin C has been studied for behavior that looks different from ordinary nutritional supplementation. In oncology discussions, one proposed mechanism is that very high concentrations may act in a pro-oxidant manner in certain contexts, generating hydrogen peroxide in ways that may stress cancer cells more than normal cells. That's one reason IV administration gets attention in integrative and supportive cancer care.
But a biologically plausible mechanism is not the same thing as a proven clinical outcome. That distinction matters. Patients deserve honesty here.
- What it may offer: In selected settings, some clinicians explore IV vitamin C as a supportive or adjunctive therapy.
- What it has not established: It should not be presented as a proven standalone cure for cancer.
- What determines appropriateness: Cancer type, treatment timing, kidney function, lab screening, goals of care, and the rest of the regimen.
A broader framework for fitting supportive therapies into individualized care appears in Hirschfeld Oncology's article on nutraceuticals and their role in patient-centric cancer care.
Where the evidence is strongest in practice
In clinic, the strongest conversations are usually not about miracle claims. They're about whether a therapy can be integrated safely and rationally. That means asking questions like:
- Is this being used alongside active treatment or after standard options have narrowed?
- Could it affect treatment timing or tolerability?
- Are we trying to support quality of life, or are expectations drifting into cure language?
Those are better questions than “Does vitamin C work?” because they reflect how oncology care is delivered.
Later in the discussion, it can help to hear an overview in a different format:
The interaction issue is real
One of the most important clinical points is that supportive therapies don't exist in isolation. High-dose vitamin C may not fit every chemotherapy or radiation plan, and timing can matter. That doesn't make it off-limits across the board. It means it should be integrated by a clinician who understands the larger oncology picture.
A useful oncology question isn't “Can I add this?” It's “How does this interact with everything else I'm already doing?”
Careful clinics differ from casual supplement advice in their approach. They don't treat vitamin C as a wellness add-on. They treat it as a therapy that may or may not fit.
Who Should Avoid High Dose Vitamin C
Some patients should be especially cautious, and some should avoid high-dose vitamin C unless their medical team has very clearly evaluated the risk. This is not just about comfort. It's about avoiding predictable harm.
Mayo Clinic and other health authorities warn that individuals with kidney disease, a history of kidney stones, G6PD deficiency, or hemochromatosis should avoid high-dose supplementation due to the risk of serious side effects in this Mayo Clinic overview of vitamin C precautions.
The clearest red flags
- Kidney disease: If kidney function is impaired, clearing large supplemental loads becomes more complicated.
- History of kidney stones: This is especially relevant when stone risk is already part of the patient's history.
- G6PD deficiency: High-dose vitamin C can create a risk of hemolytic anemia in this group.
- Hemochromatosis or iron overload states: Vitamin C can increase iron absorption, which is not a minor issue in someone already prone to excess iron.
Why screening matters in oncology
Cancer patients often assume a vitamin is safer than a medication. Sometimes that's true. Sometimes it isn't. The difference lies in the details.
A patient with advanced disease may have fluctuating renal function, dehydration, weight loss, inflammation, or treatment-related organ stress. Those factors can shift the risk-benefit balance quickly. What looks harmless for one person may be unwise for another.
If a clinic is considering IV vitamin C, pre-screening isn't bureaucracy. It's part of the treatment itself. The decision starts with the patient's biology, not with the popularity of the therapy.
A Practical Guide for Talking to Your Doctor
The most productive conversation is collaborative, specific, and tied to your actual goals. You don't need to walk into the visit asking for permission or making a pitch. You need a clear question.
Try language like this:
- “I've been reading about 3000 mg oral vitamin C and IV vitamin C. Can you help me understand whether either is relevant in my case?”
- “I'm interested in supportive therapies, but I don't want to interfere with treatment. Is vitamin C something I should avoid, monitor, or consider?”
- “If IV vitamin C is ever appropriate, what screening would you want first?”
What to bring to the appointment
Bring the actual supplement label if you're already taking one. Bring a full medication and supplement list. If you have a history of kidney stones, kidney disease, or known G6PD deficiency, say that early.
A good oncology discussion usually covers three points:
- The route matters. Oral 3000 mg and IV vitamin C are not equivalent.
- The goal matters. Nutrition support, symptom support, and adjunctive cancer therapy are different goals.
- The timing matters. Even a reasonable supportive therapy may be wrong at the wrong time.
If you're looking for a clinic-based review of whether adjunctive therapies fit your treatment plan, Hirschfeld Oncology offers consultations that evaluate supportive options, including infusion-based approaches, as part of an individualized oncology plan rather than as a one-size-fits-all add-on.
If you want a more personalized next step, explore the educational resources at Hirschfeld Oncology. The blog reflects the same practical approach used in clinic: look at the diagnosis, the current treatment plan, the patient's risk factors, and the core goal of care before deciding whether a therapy like vitamin C belongs in the plan at all.
.png)
.png)




