




.png)


You may be sitting with a notebook full of unfamiliar words, trying to remember what your doctor said after the phrase “stem cell transplant.” You heard some of it. Then the fear kicked in. Was this the next treatment? Was it the last option? Was it dangerous? Was there really more than one kind?
Those questions are normal. Patients and families often leave that first conversation feeling as if they were handed two maps written in a language they don't yet speak. The terms allogeneic and autologous sound technical, but the core difference is simple. One approach uses your own cells. The other uses cells from a donor.
That difference affects almost everything that follows, including timing, risk, monitoring, and how doctors think about the chance of the cancer coming back. In other words, allogeneic vs autologous isn't just a vocabulary lesson. It's a real treatment decision that needs to fit your disease, your body, and your goals.
Your Doctor Mentioned a Stem Cell Transplant What Now
Maria had expected to hear about another chemotherapy regimen. Instead, her oncologist said, “We should talk about transplant.” She nodded in the room, then cried in the car because she wasn't even sure what transplant meant in this context. Many patients picture surgery first. They imagine an operating room, not an infusion chair.
A stem cell transplant is usually less about replacing an organ and more about rebuilding blood formation after intensive treatment. The broad idea is this: doctors use strong therapy to treat the cancer, then give stem cells so your body can restart making healthy blood cells. That's why people sometimes describe transplant as a reset, though in real life it's more demanding and more medically complex than that word suggests.
Two paths usually come up.
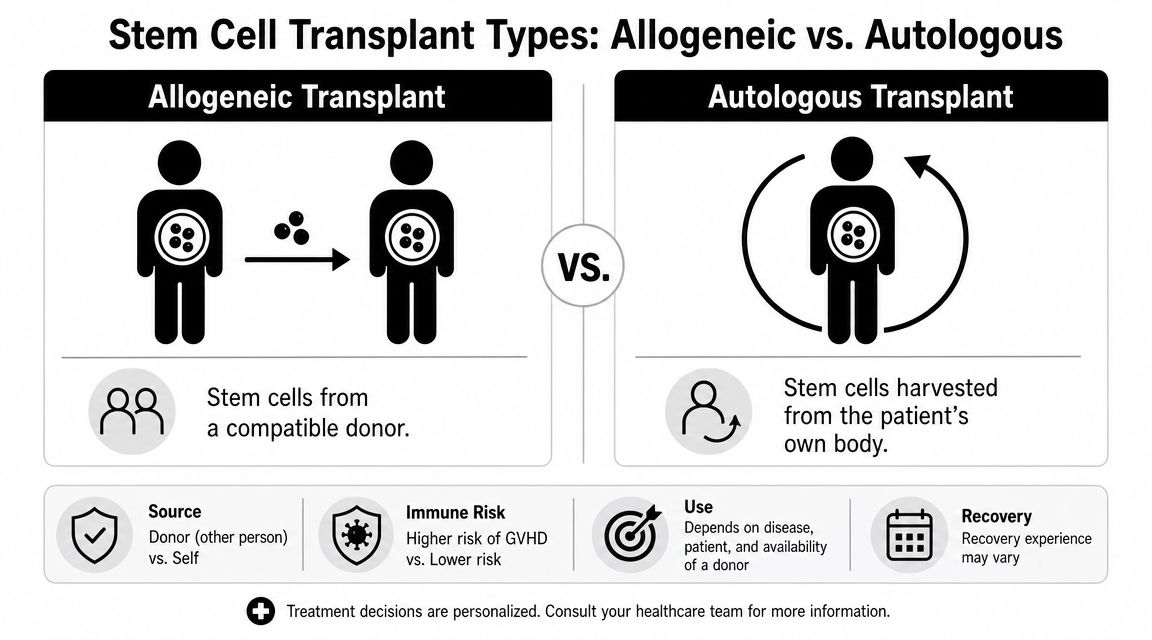
- Autologous transplant means your own stem cells are collected ahead of time and later returned to you.
- Allogeneic transplant means stem cells come from another person whose tissue type is a suitable match.
If you're still sorting through tests, scans, and procedures, it may help to review related basics like what happens during a bone marrow biopsy procedure, since biopsy results often help shape the transplant conversation.
When a doctor brings up transplant, it doesn't automatically mean one option is clearly better. It means your team is weighing a serious decision with different kinds of risks and benefits.
A quick comparison
| Factor | Allogeneic Transplant | Autologous Transplant |
|---|---|---|
| Cell source | Donor stem cells | Your own stem cells |
| Main immune issue | Donor cells may recognize your body as foreign | Lower risk of immune rejection because the cells are yours |
| Potential advantage | Donor immune system may help fight remaining cancer | Avoids donor-related immune complications |
| Main concern | GVHD and other donor-related complications | Higher concern about cancer returning in some settings |
| Logistics | Requires donor identification and matching | Requires collecting your own cells before treatment |
Defining Allogeneic and Autologous Transplants
The easiest way to understand allogeneic vs autologous is to focus on one question only: Where do the cells come from?
Autologous means self
With an autologous approach, doctors collect your own cells, preserve them, and give them back after treatment. In modern oncology more broadly, autologous cell therapy uses a patient's own cells, which are collected, modified, and reinfused to reduce the risk of immune rejection, while allogeneic therapy uses donor cells and can face HLA mismatch and rejection risks, as described in this overview of autologous and allogeneic cell therapy differences.
Imagine renovating a home with materials already from that house. The structure may still need major work, but the materials are familiar to the body. That familiarity is why autologous treatment generally avoids the classic donor-against-patient immune conflict.
Allogeneic means donor
With an allogeneic transplant, the cells come from someone else. That donor may be a relative or an unrelated volunteer, depending on the situation and the match. This introduces a new layer of biology. The donor cells can help fight cancer, but they can also react against your body.
That's why allogeneic transplant is never just “the same treatment with different cells.” It's a different immune strategy.
Why this distinction matters in daily life
The source of the cells shapes the whole treatment experience.
- Speed and availability: Allogeneic platforms are being pursued partly because they may support broader, off-the-shelf access in some cell therapy settings.
- Personalization: Autologous approaches are individualized because they start with the patient's own cells.
- Immune complexity: Donor cells can create both benefit and harm.
If you want a broader primer on the role of transplant in cancer care, can stem cells cure cancer is a useful companion read.
Key idea: The first question isn't “Which transplant is stronger?” It's “Whose cells are being used, and what does that choice ask your body to handle?”
How Each Transplant Procedure Works
Most patients experience transplant as a journey with three major phases: conditioning, infusion, and engraftment. The names sound sterile. The lived experience isn't. This is the part where planning, support, and daily monitoring matter.
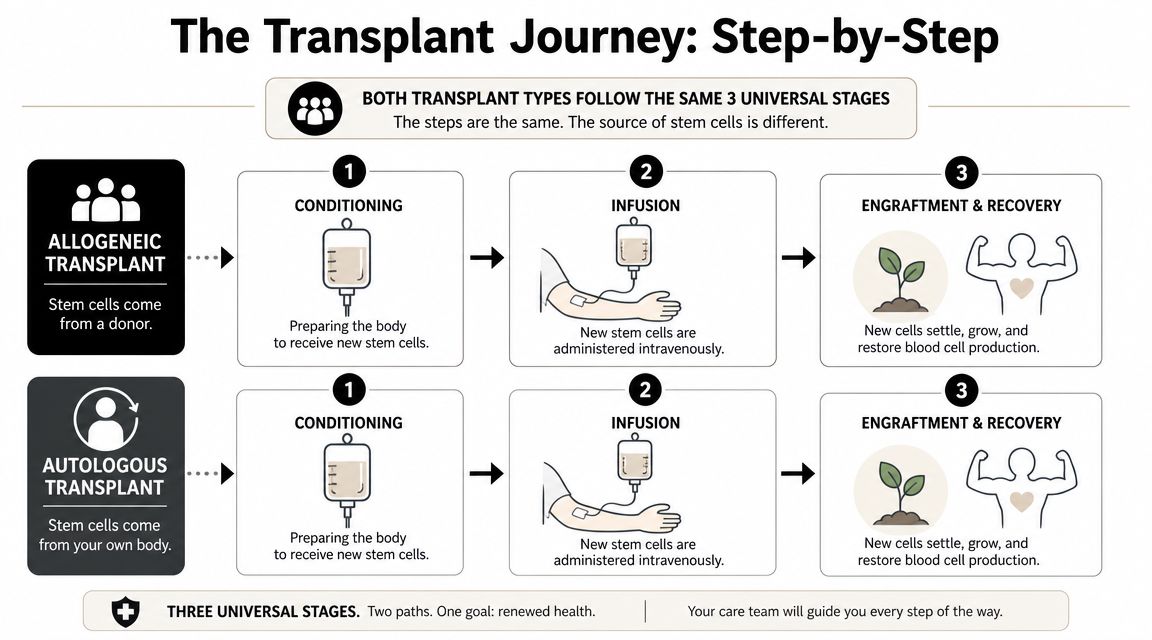
Conditioning
Before the new stem cells are infused, doctors give treatment to prepare the body. This is called conditioning. It may include high-dose chemotherapy, and in some cases radiation, depending on the disease and the transplant plan.
The purpose is usually more than one thing at once:
- Reduce cancer burden by attacking remaining malignant cells.
- Create space in the bone marrow for new cells to grow.
- Adjust the immune environment so the transplant can take hold, especially in allogeneic settings.
For patients, conditioning is often the part that feels most physically draining before the transplant itself. Fatigue, nausea, weakness, mouth soreness, and infection risk are common themes doctors discuss ahead of time.
Infusion
The actual transplant day surprises people because it often looks more like a blood product infusion than a surgery. The stem cells are infused into a vein. You're monitored closely, but there usually isn't an operation in the traditional sense.
In an autologous transplant, those are your previously collected cells coming back to you. In an allogeneic transplant, they come from the donor source your team selected.
A short visual overview can help make that sequence easier to picture:
Engraftment and recovery
After infusion, everyone waits for the cells to settle in and begin producing blood cells. That process is called engraftment. Families sometimes expect dramatic improvement right away. Usually, recovery is slower and more uneven.
During this period, the medical team watches closely for:
- Infections: Blood counts may be low, and the immune system is vulnerable.
- Bleeding risk: Low platelets can make bruising or bleeding more dangerous.
- Organ stress: Prior treatment can affect the liver, kidneys, lungs, and heart.
- GVHD in allogeneic transplant: Donor immune cells may attack the recipient's tissues.
Recovery is rarely a straight line. One day may feel encouraging, and the next may bring a fever, a rash, diarrhea, or profound exhaustion. That doesn't always mean the transplant is failing. It means transplant medicine requires patience and frequent reassessment.
Comparing Key Outcomes and Survival Data
When doctors discuss allogeneic vs autologous, they aren't only comparing procedures. They're comparing different patterns of benefit and harm. The numbers can help in this regard, as long as they're interpreted carefully and not treated like a fortune teller.
What the key terms mean
A few clinical terms often show up in these conversations:
- Overall survival refers to how many patients are alive after a defined period.
- Progression-free survival refers to how many patients are alive without the disease worsening during that period.
- Transplant-related mortality refers to death related to the treatment process rather than the cancer itself.
Those categories matter because a transplant can lower relapse risk yet still carry more treatment danger up front. That tension sits at the center of many transplant recommendations.
What one meta-analysis found
In a systematic review and meta-analysis of 30 trials involving 1,765 patients with refractory or relapsed blood cancers, 3-year overall survival was 50% for allogeneic transplant versus 55% for autologous transplant, and 3-year progression-free survival was 42% versus 41%, which was nearly equivalent. The major separation was in transplant-related mortality, which was 32% for allogeneic procedures versus 7% for autologous procedures, according to the meta-analysis of allogeneic and autologous HSCT outcomes.
That pattern is important. It tells patients something many find surprising at first. A treatment can be more immunologically aggressive and still not translate into better overall survival in every setting.
Practical rule: Ask your doctor which outcome matters most in your exact case. Lower relapse risk, better early safety, longer disease control, or a specific quality-of-life goal can lead to different recommendations.
How to read those numbers without losing the human story
These data don't mean autologous is “safer and therefore best” for everyone. They also don't mean allogeneic is “too risky” to consider. They mean the tradeoff is real.
For some patients, especially when the biology of the cancer makes relapse a dominant concern, an allogeneic strategy may still be worth the added treatment intensity. For others, preserving a lower early treatment burden matters more, especially if their disease and prior response make an autologous approach reasonable.
Statistics inform the decision. They don't make it for you.
Understanding the Major Risks GVHD vs Relapse
If families remember only one medical tradeoff from the transplant discussion, it's often this one: GVHD versus relapse.
An allogeneic transplant brings in a donor immune system. That donor immune system may attack residual cancer, which is one reason the approach can be so powerful. But it may also attack normal tissues. That complication is called graft-versus-host disease, or GVHD.
An autologous transplant avoids that donor-versus-host conflict because the cells are your own. But it doesn't provide the same donor immune attack on leftover cancer cells. So the central concern often shifts toward whether the disease may come back.

What GVHD can feel like
GVHD is not one single experience. It can range from manageable to severe. Patients may notice rash, gastrointestinal symptoms, liver problems, eye or mouth dryness, or more persistent whole-body effects that interfere with daily life.
This matters when talking about quality of life. Some people hear “lower relapse risk” and understandably focus on the cancer only. But transplant decisions also involve asking what kind of recovery a person is prepared to live through.
Why relapse remains such a powerful concern
Relapse isn't just a lab value or scan result. It means more treatment, more uncertainty, and often a heavier emotional burden the second time around. Patients who choose autologous transplant may do so because avoiding donor-related immune injury is very important to them. That can be a sound choice. It still requires an honest discussion about the possibility that disease control may be less durable in some settings.
Infection risk also deserves attention during recovery. Families trying to protect a loved one after transplant often benefit from practical education on hospital-acquired infection risks, including this guide to understanding nosocomial infections, because infection prevention becomes part of everyday life after intensive therapy.
Allogeneic vs. Autologous Transplant At-a-Glance
| Factor | Allogeneic Transplant | Autologous Transplant |
|---|---|---|
| Cell source | Donor | Patient's own cells |
| GVHD risk | Present | Not a classic concern |
| Graft-versus-tumor effect | Possible and often clinically important | Absent |
| Relapse concern | May be lower in some settings | May be higher in some settings |
| Immune suppression and monitoring | More complex | Usually less donor-immune complexity |
| Recovery experience | Often more medically intensive | Often less donor-related immune toxicity |
The hardest part of allogeneic vs autologous is that both choices can be reasonable. You aren't choosing between “good” and “bad.” You're choosing which risk your team believes is more acceptable in your situation.
Cancers Treated and Patient Eligibility
The transplant recommendation usually starts with the disease. But it never ends there. Doctors also look at your age, organ function, treatment history, physical strength, infection history, and support system at home.
Where each approach often fits
Autologous and allogeneic transplant are both used in blood cancers, but they tend to serve different clinical purposes. In broad terms, doctors often consider autologous transplant when they want to intensify treatment while avoiding donor-related immune complications. They often consider allogeneic transplant when they need not only marrow replacement but also the immune anti-cancer effect that donor cells may provide.
That's the medical reasoning. The patient-level question is different: can your body tolerate the plan, and does the potential benefit justify the burden?

A real example beyond blood cancers
Cell therapy thinking is also expanding into solid tumors. One example comes from pancreatic cancer. In the TACTOPS phase 1/2 trial, 37 patients received six monthly infusions of autologous T cells targeting multiple tumor antigens. The trial reported 84.6% disease control in patients whose disease had responded to frontline chemotherapy in Arm A, 25% disease control in refractory metastatic disease in Arm B, and 2 of 9 surgically resected patients in Arm C remained disease-free for more than 5 years after surgery, as reported by Baylor College of Medicine on the TACTOPS autologous T-cell trial.
This doesn't mean standard stem cell transplant is now routine for pancreatic cancer. It does show something important. Personalized autologous immune approaches are being studied in advanced solid tumors, while allogeneic approaches are also being pursued because broader manufacturing and faster access could help more patients if immune barriers can be overcome.
Eligibility is more personal than many people expect
A transplant team often weighs questions like these:
- How aggressive is the disease right now
- How well did it respond to prior treatment
- Can the heart, lungs, liver, and kidneys tolerate intensive therapy
- Is there enough day-to-day support for medications, visits, and symptom monitoring
- Does the patient value maximum anti-cancer intensity, or a gentler recovery path when options are close
Patients with complex diagnoses often benefit from seeing how different cancers are approached across specialties, including resources on cancers we treat.
Making the Right Choice for Your Situation
This decision isn't only medical. It's personal. Two patients with the same diagnosis may reasonably choose different paths because they define an acceptable risk differently.
Start with your real goal
Some patients say, “I want the strongest anti-cancer option, even if recovery is harder.” Others say, “I want meaningful treatment, but I also need to protect function, independence, and time at home.” Neither answer is wrong.
The trouble comes when people think they're supposed to want what the statistics alone seem to favor. Treatment should fit your values, not just your pathology report.
The first 100 days matter
One comparative cohort of 751 patients found that first-transplant allogeneic therapy had lower relapse at 36 months, 45.9% versus 68.4%, but also higher non-relapse mortality, 27.0% versus 7.3%. The study also found a marked early hazard, with a higher risk of death and progression in the first 100 days for the allo-first group, according to this Haematologica study of allo-first versus auto-first transplant outcomes.
For families, that means the question isn't only “Which transplant lowers relapse?” It's also “Can we safely get through the early recovery window?”
If an allogeneic transplant is on the table, ask who will help during the first 100 days. Not in theory. By name. By schedule. By task.
Questions worth bringing to your next visit
- What matters most in my case, lowering relapse risk or lowering treatment-related risk
- How likely is it that I'll need prolonged monitoring or immune-suppressing medication
- What would recovery look like at home, not just in the hospital or clinic
- If complications happen, what are the most common ones you want my family to watch for
- How does this recommendation fit my quality-of-life priorities
A good transplant conversation should leave you with more than a recommendation. It should leave you with a plan you understand and can live with.
Common Questions and Expert Guidance
How is a donor found for an allogeneic transplant
Your transplant team looks for a compatible donor based on tissue matching. That process may involve relatives first, then volunteer donor registries if needed. Patients often assume “no sibling match” means “no transplant,” but that isn't always true. The team can explain what kind of donor match they're seeking and what alternatives exist.
What does long-term recovery really look like
Recovery usually happens in stages. Blood counts may recover before stamina does. Appetite, sleep, concentration, and physical strength can take much longer to normalize. For allogeneic recipients, long-term follow-up may also include watching for chronic immune complications.
Can I work or travel after transplant
Sometimes yes, but not quickly and not predictably. The answer depends on your blood counts, infection risk, medications, energy level, and whether you're dealing with complications such as GVHD. It helps to think in terms of milestones rather than dates.
Should I bring family to every major transplant visit
If possible, yes. A second set of ears matters. Transplant decisions involve timing, medication schedules, warning signs, and logistics that are hard to absorb alone when you're under stress.
No article can tell you which transplant is right for you. It can help you ask better questions, understand the language, and recognize that allogeneic vs autologous is not just a clinical fork in the road. It's a choice about risk, recovery, and what kind of future you're trying to protect.
If you're facing a complex cancer diagnosis and want a thoughtful, individualized discussion of your options, Hirschfeld Oncology offers patient-centered guidance grounded in careful risk-benefit review, quality-of-life priorities, and advanced treatment planning. A consultation can help you understand whether transplant-related strategies, immunologic approaches, or other personalized therapies fit your specific disease, goals, and tolerance for treatment.
.png)
.png)




