




.png)


You're probably in one of two places regarding an alternative to tamoxifen. You're either taking it and feeling like the treatment is asking too much of your day-to-day life, or you've been told your cancer may need a different endocrine strategy. Both situations are common in practice, and neither means you've failed treatment.
For many people with hormone receptor-positive breast cancer, tamoxifen is the first endocrine therapy they hear about. It has earned that place. But it isn't the only option, and it isn't always the best fit forever. Menopausal status, recurrence risk, side effects, and signs of resistance all matter.
Patients often tell me they feel caught between two fears: staying on a drug that feels miserable, or changing course and worrying they'll lose protection. That tension is real. Good oncology care doesn't dismiss it. It works through it carefully, using evidence, symptom management, and honest discussion about trade-offs.
If you want a broader overview of breast cancer care and treatment pathways, this conversation fits inside that bigger picture. Endocrine therapy is one piece of care, but for many HR+ cancers, it's a foundational one.
Navigating Your Hormone Therapy Journey
A common clinic conversation starts like this: "I was told tamoxifen was standard, so why am I already asking about something else?" Usually, the reason is practical. The hot flashes are relentless. Sleep is poor. Mood feels off. Or the pathology, menopausal status, and recurrence risk make a different strategy more appropriate from the beginning.
Sometimes the question comes later. A person has done everything right, taken endocrine therapy as prescribed, shown up for visits, pushed through side effects, and then hears that the cancer may no longer be responding the way it once did. That can feel like the floor shifting under you. It isn't a sign that there are no next steps. It means the treatment plan needs a more precise match.
The best endocrine plan is not the most familiar one. It's the one that fits the biology of the cancer and the life of the person taking it.
That may mean staying with tamoxifen and managing side effects more aggressively. It may mean moving to an aromatase inhibitor. For some postmenopausal women focused on risk reduction, raloxifene enters the discussion. For people dealing with resistance in advanced disease, newer endocrine approaches and targeted combinations may matter more than a simple switch from one pill to another.
What helps most is treating this as a decision process, not a test you have to pass. Ask why a drug is being recommended. Ask what problem it's solving. Ask what would make your oncologist change course. Those questions lead to better care.
Why You Might Need an Alternative to Tamoxifen
Most searches for an alternative to tamoxifen come from two real-world problems. The first is tolerability. The second is resistance.

When side effects start to run your life
Even when tamoxifen is the right drug on paper, some people struggle to stay on it comfortably. The issue isn't just inconvenience. If side effects disrupt sleep, mood, sexual health, daily function, or confidence in treatment, adherence can suffer.
A few concerns come up repeatedly in clinic:
- Hot flashes and night sweats: These can interfere with sleep and make daytime fatigue worse.
- Mood changes: Some patients describe feeling unlike themselves, even when outside stress hasn't changed.
- Blood clot risk: This is one reason some people need a different plan.
- Uterine concerns: Tamoxifen has a different gynecologic risk profile than some alternatives.
Quality of life isn't a soft endpoint. If a person can't realistically stay on a medication, the "best" treatment on paper may not be the best treatment in practice.
When the cancer stops listening
Resistance is harder to see, because you can't feel it happening. The basic idea is simple: tamoxifen blocks the estrogen receptor, but cancer cells can sometimes find ways around that blockade. Over time, the tumor may rely on alternate growth signals or change how it uses the receptor.
I often explain it this way. Tamoxifen locks one door. Some cancers eventually learn to use a side entrance.
That doesn't mean endocrine therapy is over. It means the next move may need a different mechanism, a stronger endocrine backbone, or a targeted partner drug.
Practical rule: If you're having major side effects or your cancer has progressed on endocrine therapy, don't frame the visit as "Should I just stop?" Frame it as "What's the next endocrine strategy, and what problem is it meant to solve?"
What usually doesn't work
What doesn't work is silent suffering, missed doses without telling your team, or assuming there are only two choices: endure tamoxifen or abandon hormone therapy entirely. There are often intermediate options, supportive medications, schedule adjustments, and alternative endocrine approaches that can preserve both effectiveness and livability.
Aromatase Inhibitors for Postmenopausal Women
For many postmenopausal women with HR+ breast cancer, the most established alternative to tamoxifen is an aromatase inhibitor, usually anastrozole, letrozole, or exemestane. These drugs don't just block the estrogen receptor. They reduce estrogen production outside the ovaries, which matters after menopause because estrogen is still made in other tissues.
Why this approach became standard
The evidence behind AIs is strong. In a large pooled analysis from the Early Breast Cancer Trialists' Collaborative Group, 31,920 postmenopausal women had a 21% lower recurrence risk with aromatase inhibitors compared with tamoxifen, and the 5-year absolute recurrence risk fell from 10.1% with tamoxifen to 6.9% with an aromatase inhibitors, a 3.2 percentage point difference, as summarized in this review of tamoxifen alternatives and aromatase inhibitor data.
That kind of evidence is why many postmenopausal patients hear about anastrozole, letrozole, or exemestane early in treatment planning. The recommendation isn't based on novelty. It's based on recurrence reduction.
The trade-offs patients actually feel
Aromatase inhibitors solve one problem and can create another. They often avoid some of tamoxifen's specific risks, but they can be harder on joints, muscles, and bone health. In practice, the question isn't whether AIs have side effects. They do. The question is whether those effects can be anticipated and managed well enough for the treatment to remain workable.
Useful conversations include:
- Joint and stiffness symptoms: Some people do fine. Others feel older overnight. Early reporting matters.
- Bone health: If someone already has osteopenia or fracture concerns, that affects planning.
- Exercise and symptom support: Strength training, mobility work, and symptom-directed supportive care can make a meaningful difference for some patients.
- Menopause symptom overlap: People already dealing with postmenopausal symptoms may need a broader symptom plan, including nonhormonal strategies. Some patients also ask about natural remedies for menopause symptoms as part of a supportive care discussion.
An aromatase inhibitor isn't automatically easier than tamoxifen. It's often more effective for the right patient, but it has its own maintenance work.
Which AI is best
There usually isn't one universally "best" AI. Anastrozole, letrozole, and exemestane are all familiar options in oncology practice. The most suitable choice often comes down to prior tolerance, symptom pattern, comorbidities, and whether a patient has already tried one drug in the class. If one AI causes troublesome side effects, switching within the class can sometimes help.
For postmenopausal women asking for an alternative to tamoxifen, this is often the most evidence-based place to start.
Treatment Options for Premenopausal Women
Premenopausal women need a different conversation. The ovaries are still the main source of estrogen, so an aromatase inhibitor by itself usually isn't enough. That's why tamoxifen historically became the default endocrine therapy in this setting.
The modern alternative is more nuanced: ovarian function suppression combined with an aromatase inhibitor. Ovarian suppression lowers estrogen production from the ovaries, and then the AI reduces estrogen made elsewhere. Together, that can be a stronger endocrine approach for selected higher-risk patients.
What ovarian suppression changes
Ovarian function suppression is often done with medication. In practice, patients usually experience it as an intentional move into a low-estrogen state. That's the point therapeutically, but it's also why side effects can feel substantial.
This approach isn't for everyone. It asks more of the patient physically, and sometimes emotionally, than tamoxifen alone. But for some women, especially those with features that justify more intensive endocrine therapy, it deserves a direct discussion.
What the evidence supports
In the EBCTCG analysis summarized by Oxford Population Health, switching from tamoxifen to an AI in women receiving ovarian suppression reduced breast-cancer recurrence by 21% overall, with the biggest effect during the first five years when treatments differed. The absolute 5-year recurrence risk fell from 10.1% with tamoxifen to 6.9% with an AI, according to Oxford Population Health's summary of aromatase inhibitors with ovarian suppression in premenopausal women.
That doesn't mean every premenopausal patient should intensify therapy. It means tamoxifen isn't the only serious option.
How to think about the trade-off
For a younger patient, the choice often comes down to balancing recurrence risk against treatment burden.
A few practical questions help:
- How high is the baseline risk? Higher-risk disease often pushes the discussion toward stronger endocrine suppression.
- What symptoms are acceptable, and for how long? Some patients are willing to trade more side effects for added recurrence reduction. Others aren't.
- Would treatment-induced menopause create major quality-of-life issues? Fertility goals, sexual health, sleep, and mood all matter.
For premenopausal women, the key question usually isn't "tamoxifen or not?" It's "Is tamoxifen enough for my level of risk?"
That question is worth asking plainly.
Comparing Your Hormone Therapy Options
A side-by-side comparison often makes the choice easier to discuss. These therapies aren't interchangeable. They serve different patients and different goals.
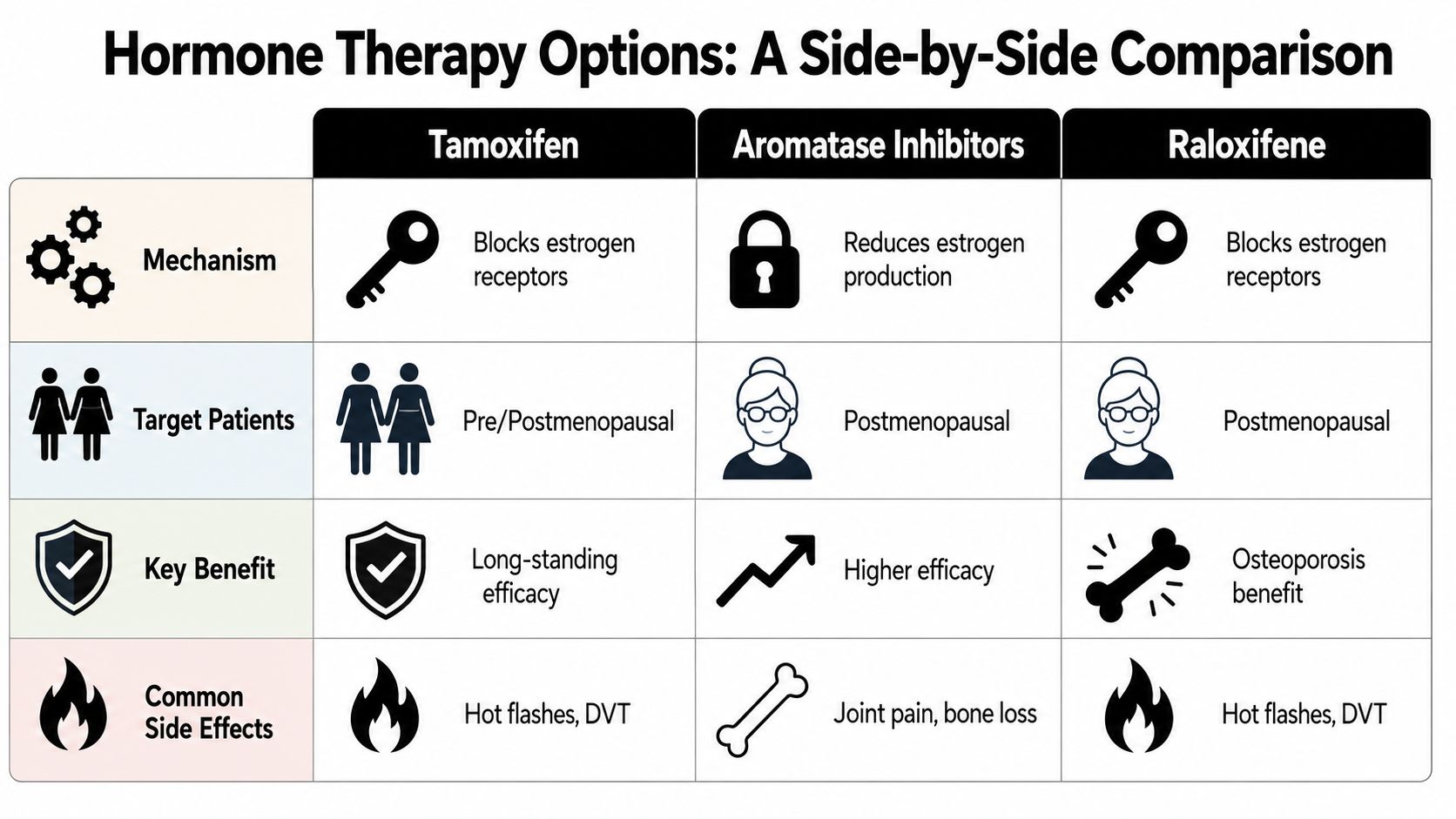
| Option | Main role | Best fit | Core mechanism | Main watch-outs |
|---|---|---|---|---|
| Tamoxifen | Treatment and prevention in appropriate settings | Premenopausal or postmenopausal patients, depending on context | Blocks estrogen receptors | Hot flashes, clot risk, uterine concerns |
| Aromatase inhibitors | Treatment | Most often postmenopausal women, or premenopausal women with ovarian suppression | Lowers estrogen production | Joint symptoms, bone health concerns |
| Raloxifene | Risk reduction, not the usual curative treatment substitute | Postmenopausal women | Selective estrogen receptor modulation | Hot flashes, clot risk, but a different uterine safety profile than tamoxifen |
Where raloxifene fits
Raloxifene is often misunderstood in this discussion. It is a real alternative to tamoxifen, but usually in the setting of breast cancer risk reduction for postmenopausal women, not as the standard replacement for endocrine treatment of established breast cancer.
Key distinction: Raloxifene became an FDA-approved alternative to tamoxifen for breast cancer risk reduction in postmenopausal women, and unlike tamoxifen, it does not increase the risk of endometrial and uterine cancers while still carrying a lower clot risk than tamoxifen, as described by Mayo Clinic's review of breast cancer prevention medicines.
Mayo Clinic also notes that raloxifene is typically taken once daily for five years in that prevention setting. That matters because some patients searching for an alternative to tamoxifen are really asking a prevention question, while others are asking a treatment question. Those are not the same conversation.
A practical summary
If you want the short version:
- Tamoxifen remains a validated standard with a long track record.
- Aromatase inhibitors are the most evidence-backed alternative for many postmenopausal patients.
- Raloxifene belongs mainly in risk-reduction discussions for postmenopausal women.
For a broader overview of how these drugs fit into endocrine care, this guide to cancer hormone therapy is useful background reading.
Beyond Standard Hormonal Therapy
When standard endocrine therapy stops working well enough, the conversation changes. At that point, asking for an alternative to tamoxifen may be too narrow. The better question is whether the cancer now needs a different endocrine class, a targeted add-on, or a clinical trial.

When endocrine resistance becomes the main issue
In resistant HR+ disease, clinicians often look beyond a simple swap between tamoxifen and an aromatase inhibitor. Combination strategies with CDK4/6 inhibitors such as palbociclib, ribociclib, and abemaciclib have become part of how many advanced cases are managed. Other targeted pathways may matter in selected tumors as well.
The point for patients is this: progression on one endocrine therapy doesn't close the door on hormone-driven treatment. It often means the biology needs to be approached more intelligently.
Why oral SERDs matter
A newer area of interest is the rise of oral SERDs, or selective estrogen receptor degraders. Instead of blocking the receptor, these drugs are designed to degrade it. That difference is especially important in resistance discussions, where the receptor itself may have changed in ways that make older strategies less effective.
One of the emerging names patients may hear is giredestrant. In a 2025 report on the lidERA breast cancer trial, giredestrant reduced any recurrence by 30% and distant or metastatic recurrence by 31% versus tamoxifen or an aromatase inhibitor, with 92.4% recurrence-free survival at three years compared with 89.6% for standard hormonal therapy, according to Breastcancer.org's report on the lidERA trial.
That doesn't make giredestrant the current answer for everyone. It does show why patients with resistant disease, high-risk early disease, or limited tolerance for standard options should ask whether a trial is relevant now rather than later.
If standard endocrine therapy is failing, the most useful appointment question may be, "What mechanism of resistance are we treating, and is there a trial that matches it?"
When to ask about clinical trials
Ask early if:
- Your cancer progressed on endocrine therapy: That often signals a need for a different strategy, not just a different brand name.
- Your side effects are limiting standard treatment: A trial may offer another route when usual options aren't tolerable.
- You have high-risk disease and want to know what's coming next: Future practice often begins with such cases.
- Your oncologist mentions tumor mutations or resistance markers: Those details may open doors to more personalized options.
If you want to understand how trial participation works in practice, this overview of clinical trials for breast cancer is a good place to start.
How to Decide with Your Oncologist
The right endocrine plan usually becomes clearer when the discussion gets specific. Not "What do people usually take?" but "What makes sense for my cancer, my menopause status, my side effects, and my goals?"
Bring questions that force the decision to become individualized.
Questions worth taking into the visit
- About fit: Am I a good candidate for tamoxifen, an aromatase inhibitor, ovarian suppression plus an AI, or something beyond standard endocrine therapy?
- About side effects: Which problems should I expect, which ones can be treated, and which ones would make you change the plan?
- About resistance: Do you think my cancer is still endocrine-sensitive, or are we seeing signs that it's bypassing hormone therapy?
- About monitoring: How will we know this treatment is working, and what changes would trigger a switch?
- About next-generation options: Should I be asking about oral SERDs, CDK4/6 inhibitors, or a clinical trial?
- About tumor biology: Is there any role for additional tumor testing that could help guide the next step?
What a good decision usually sounds like
A strong plan sounds concrete. It names the drug, why it's being chosen, what benefit it's expected to offer, what trade-offs matter most, and what the backup plan is if it doesn't work or isn't tolerable.
A weak plan sounds vague. "Let's just try this" isn't enough when someone is dealing with recurrence fears, major symptoms, or progression on prior therapy.
You don't need to walk into the appointment knowing the answer. You do need to leave knowing the reasoning.
If you're considering an alternative to tamoxifen because side effects are wearing you down, say that directly. If you're worried because the cancer has progressed, say that directly too. Both concerns deserve a precise response.
If you want a more personalized review of endocrine therapy options, resistance patterns, or whether newer treatment strategies may fit your case, Hirschfeld Oncology offers compassionate, research-informed guidance for patients facing complex breast cancer decisions. A thoughtful consultation can help clarify what standard options still make sense, when it may be time to look beyond them, and which questions to bring to the next treatment decision.
.png)
.png)




