




.png)


You may be reading this after a colonoscopy, a pathology call, or a long week of tests that started with something that didn’t seem dramatic enough to be cancer. Maybe it was fatigue. Maybe your doctor found anemia. Maybe you kept telling yourself the abdominal discomfort would pass.
Then someone said the words ascending colon cancer.
That diagnosis can feel strange and disorienting because many people know the term “colon cancer” but haven’t heard much about the ascending colon, the right-sided part of the colon where this cancer begins. Families often ask the same questions right away. Where exactly is it? Why didn’t it cause clearer symptoms? Does “right-sided” matter? What treatments make sense if standard options feel too harsh or haven’t worked?
It does matter. And understanding why it matters can make the next decisions less overwhelming.
Navigating Your Ascending Colon Cancer Diagnosis
A common story goes like this. A person feels more tired than usual for months. They notice less stamina climbing stairs or carrying groceries. Blood work shows anemia. That leads to more testing, then a colonoscopy, then a biopsy, and suddenly a diagnosis that seems to come out of nowhere.

If that sounds familiar, you’re not overreacting. Ascending colon cancer often doesn’t announce itself loudly. It can grow in a part of the colon where symptoms are easier to miss, so people may feel confused about how something serious developed without obvious warning.
Why this diagnosis feels different
The ascending colon sits on the right side of the abdomen. Cancers in this area are part of what doctors call right-sided colon cancers. They don’t always behave like cancers on the left side of the colon.
That difference affects three things:
- Symptoms: right-sided tumors may cause subtle problems such as fatigue or anemia rather than early visible bleeding.
- Biology: these tumors often have a different molecular pattern than left-sided cancers.
- Treatment choices: surgery, chemotherapy, immunotherapy, and targeted therapy may be weighed differently based on the tumor’s stage and biomarker profile.
You do not need to understand everything at once. You need a clear explanation of what your own tumor is doing and what options fit that reality.
What patients and families usually need first
Most families don’t need more medical jargon on day one. They need a roadmap.
That roadmap usually starts with a few practical questions:
- Where is the tumor and how deep has it grown?
- Has it reached lymph nodes or spread elsewhere?
- What does the pathology show beyond the basic diagnosis?
- Were molecular tests done, including MSI or MMR status and mutation testing when appropriate?
- What is the goal of treatment right now, cure, control, symptom relief, or some combination?
Those questions shift the conversation from fear to action.
A steadier way to think about the next steps
Cancer care can feel like a blur because many decisions arrive quickly. But most plans become easier to follow once you break them into pieces: anatomy, symptoms, testing, stage, biology, then treatment.
That’s especially important in ascending colon cancer, because generic advice about “colon cancer” can miss what’s distinctive about a right-sided tumor. When you understand those differences, it becomes easier to ask focused questions and recognize where newer, more personalized treatments may offer real hope.
Understanding Your Colon's Anatomy and Cancer's Origin
Think of the colon as the final stretch of a long processing system. Food moves through the small intestine first, where most nutrients are absorbed. What remains enters the large intestine, where water is removed and waste is gradually formed into stool.
The ascending colon is the first major upward segment of the large intestine. It sits on the right side of the abdomen and carries contents upward before they turn across the body through the transverse colon.

Where ascending colon cancer begins
Cancer starts when a group of cells stops following the body’s normal rules. Healthy colon cells grow, do their job, and are replaced in an orderly way. Cancer cells keep dividing when they shouldn’t. Over time, they can form a polyp or mass, invade the colon wall, and sometimes spread beyond it.
In the ascending colon, this process can be easy to miss early. The stool in the right colon is more liquid than it is farther downstream, so a growth can become fairly large without causing the kind of blockage that often alerts people to left-sided disease.
Why right-sided location matters
This isn’t a rare corner case. The ascending colon represents about 15 to 20% of all colon cancer cases in major markets like the United States and Europe, and colorectal cancer remains a major public health burden. SEER lists colorectal cancer as the third most common cancer, with an incidence rate of 37.1 new cases per 100,000 men and women annually. SEER also reports a lifetime risk of 1 in 25 for men and 1 in 26 for women. Screening has made a real difference, with 72.6% of US adults ages 50 to 75 screened by 2023, up from 38.2% in 2000. At the same time, early-onset colorectal cancer has risen, now making up 20% of diagnoses, up from 11% in 1995, with incidence in young adults rising from 4.5 to 9.4 per 100,000 by 2022 according to SEER colorectal cancer statistics.
That broader picture helps explain why screening matters so much. When doctors find and remove polyps during colonoscopy, they can prevent some cancers before they ever form.
For readers who want a broader overview of the disease itself, this guide to colon cancer care and diagnosis can be a helpful companion.
A simple way to picture it
A plumbing analogy can help. If the colon were a long pipe, the ascending colon would be an early vertical section on the right. A small irregularity there may not change the flow enough to be obvious. Farther left, where stool is more formed and the space can feel tighter, growths may cause more noticeable changes sooner.
Practical rule: location changes behavior. Two tumors can both be “colon cancer” and still act differently because they started in different parts of the colon.
What families often find reassuring
Many people assume cancer in one part of the colon must behave exactly like cancer in every other part. That’s not how this disease works. The tumor’s location, the way it grew, and its molecular features all shape what comes next.
That’s why a diagnosis of ascending colon cancer should lead to more specific questions than “What stage is it?” It should also lead to “What kind of right-sided tumor is this, biologically?”
Recognizing the Subtle Symptoms and Red Flags
The most frustrating part of ascending colon cancer is often how ordinary the early symptoms can seem. A person may feel run-down, short of breath on exertion, or just “off” for months before anyone suspects the colon.

That pattern isn’t imagined. Right-sided tumors often produce subtle signs rather than dramatic bowel changes early on.
What right-sided symptoms often look like
Because the ascending colon holds more liquid stool, tumors there are less likely to cause early narrowing or obvious blockage. Instead, patients often notice symptoms related to slow blood loss or a gradually growing mass.
Common warning signs can include:
- Unexplained fatigue: especially if it’s new, persistent, or out of proportion to daily activity
- Iron-deficiency anemia: often found on blood work before the cancer is diagnosed
- Occult bleeding: bleeding that isn’t visible in the stool
- Abdominal discomfort or fullness: often vague rather than sharp
- Unintentional weight loss: not always dramatic, but noticeable over time
- Reduced exercise tolerance: feeling winded or weak more easily than usual
In younger patients, this can be even more misleading. Ascending colon tumors may present with anemia rather than obvious bleeding, which can delay diagnosis.
How this differs from left-sided colon cancer
Left-sided colon cancers more often cause what people think of as “classic colon symptoms.” That contrast matters because it explains why some right-sided cancers are found later.
| Tumor location | Symptoms more likely to appear early |
|---|---|
| Ascending or right-sided colon | Fatigue, anemia, hidden blood loss, vague abdominal symptoms |
| Left-sided colon | Visible blood in stool, more noticeable bowel habit change, narrowing symptoms |
The location changes the signal. Right-sided disease can stay quieter longer.
When symptoms are vague, people often doubt themselves. If anemia, fatigue, or persistent abdominal symptoms don’t have a clear explanation, it’s reasonable to ask whether the colon has been fully evaluated.
When to push for a fuller workup
Readers often ask when a symptom stops being “probably nothing” and becomes something worth chasing. There isn’t one perfect threshold, but these patterns deserve attention:
- Symptoms that persist: if fatigue, abdominal discomfort, or weight loss doesn’t resolve
- Abnormal labs: especially iron-deficiency anemia without a clear cause
- Symptoms that stack together: for example, fatigue plus anemia plus reduced appetite
- Family concern: loved ones often notice declining energy or appearance before the patient does
A short educational overview may help as you compare symptoms and next steps:
Why people get confused
Many non-cancer conditions can also cause tiredness, abdominal discomfort, or anemia. That overlap is exactly why ascending colon cancer can hide in plain sight. It doesn’t mean your doctors missed something obvious. It means the disease often doesn’t behave in an obvious way.
That said, persistent symptoms deserve respect. If you or someone you love has ongoing anemia or fatigue without a satisfying explanation, asking direct questions is not overreacting. It’s good medical self-advocacy.
Your Diagnostic Journey From Suspicion To Staging
A common moment in clinic goes like this. Someone comes in expecting to discuss anemia, fatigue, or a scan result, and by the end of the visit they are hearing words like colonoscopy, biopsy, staging, and molecular testing. That sudden shift can feel overwhelming. What helps is knowing that the workup follows a clear sequence. Each step answers a different question, and together those answers show not only whether cancer is present, but how a right-sided colon cancer may behave.
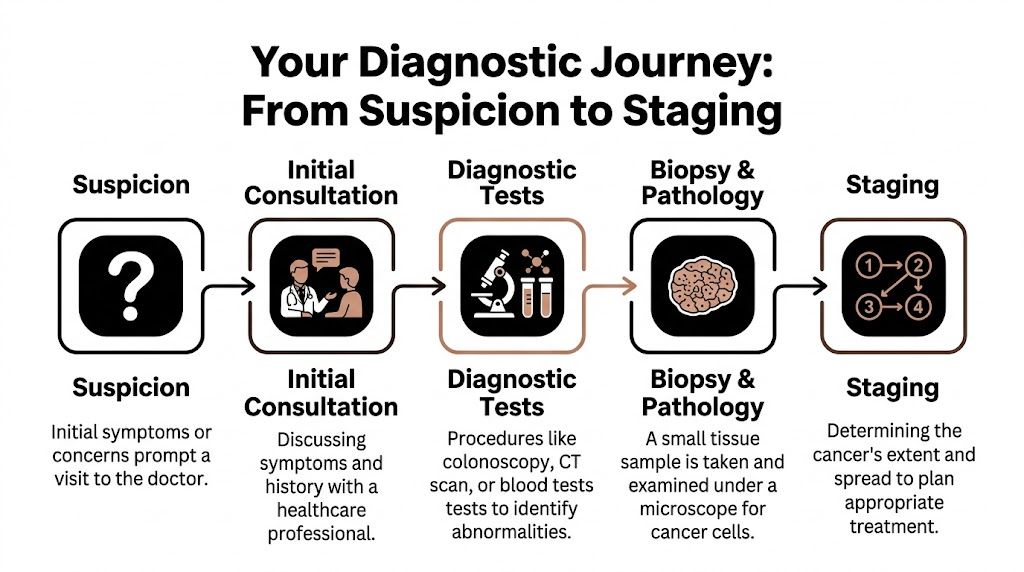
The first steps after suspicion
Doctors usually begin by confirming the problem from two angles. One angle is direct visualization of the colon. The other is a wider look at the rest of the body.
That often means:
Colonoscopy
This lets the gastroenterologist inspect the inside of the colon directly. If they see a suspicious mass or ulcer, they can take samples during the same procedure.Biopsy and pathology
The biopsy answers the basic question of diagnosis. The pathologist then adds detail about the tumor type and features that may affect treatment choices.CT imaging
CT scans of the chest, abdomen, and pelvis help show whether the cancer appears limited to the colon or has reached lymph nodes, the liver, the lining of the abdomen, or other organs.Blood work, including CEA
CEA is not a screening test, and a normal result does not rule cancer out. Still, it can be useful later as a reference point when your team monitors response or watches for recurrence.
If you want a plain-language guide to what stage labels mean, this overview of colon cancer stages can make pathology and scan reports easier to read.
How staging works in plain language
Staging is the medical version of a map. It tells your team where the tumor started, how far it has grown locally, whether nearby lymph nodes are involved, and whether any cancer cells have set up elsewhere.
Doctors usually describe this with the TNM system:
- T describes how far the tumor has grown into or through the wall of the colon
- N describes whether nearby lymph nodes or tumor deposits are involved
- M describes whether the cancer has spread to distant sites
For ascending colon cancer, this map matters in a very practical way. The right colon sits in a part of the abdomen where the anatomy is not identical to the left side. Some of the posterior surface is fixed against the back of the abdomen rather than fully wrapped in serosa, which can affect how the tumor spreads locally and how surgeons judge margins. That is one reason right-sided cancers deserve their own lens rather than generic colon cancer advice.
Why the pathology report matters so much
Families often look for the stage first. That makes sense. But stage is only the headline.
The pathology report is more like the full weather forecast. Two patients can both have stage II disease, yet one may be watched closely after surgery while the other is advised to consider chemotherapy. The difference often comes from details inside the specimen and from the tumor’s biology.
Pathology may include:
- Lymphovascular invasion
- Perineural invasion
- Poor differentiation
- Tumor deposits
- MSI or MMR status
- CEA level before surgery
Those features help doctors estimate risk more accurately, especially in stage II disease where treatment decisions are often less straightforward.
A stage label summarizes the extent of disease. The pathology and biomarker details explain the tumor’s personality.
Why MSI and molecular testing matter more in right-sided tumors
This point is especially important in ascending colon cancer. Right-sided tumors are more likely than left-sided tumors to carry biological features that change treatment decisions, including MSI-H or dMMR status. That can matter at several points in care.
In earlier-stage disease, MSI-H or dMMR can be associated with a different prognosis and can influence whether standard adjuvant chemotherapy is likely to help. In advanced disease, the same finding may open the door to immunotherapy, which has changed the outlook for some patients with metastatic right-sided colon cancer.
Doctors may also order molecular testing for markers such as KRAS and BRAF, particularly if the disease is advanced or if treatment choices are becoming more personalized. This is one of the places where the biology of ascending colon cancer becomes highly relevant. The location is not just a map coordinate. It often reflects a different molecular pathway.
A few staging details your team may mention
Some staging terms sound cryptic at first, but they become easier once you know the pattern.
- T1 through T4 describe how far the tumor has grown through the bowel wall and into nearby structures
- N categories describe whether cancer is found in regional lymph nodes or as tumor deposits
- M1 means distant spread is present, and subcategories help describe where that spread is seen, including the peritoneum
Specialty guidance also notes several practical points that matter in right-sided colon cancer care: the ascending colon is about 15 to 20 cm long, part of it lies retroperitoneally, T stage is assigned by depth of invasion, N stage depends on the number of involved nodes or tumor deposits, and findings such as high preoperative CEA, lymphovascular invasion, and additional lesions found on CT colonography can affect prognosis or treatment planning, as summarized in the ASCRS colon cancer management guidance.
Questions worth bringing to your next visit
- Was the tumor fully staged with CT imaging?
- What is the exact T, N, and M category?
- Did the pathology show lymphovascular or perineural invasion?
- What was the pre-treatment CEA?
- Was MSI or MMR testing done?
- Should molecular testing for KRAS, BRAF, or related markers be ordered now?
These questions often make the conversation more concrete. Concrete information tends to lower fear, because it turns uncertainty into decisions your team can make.
Standard and Advanced Treatment Pathways
Treatment for ascending colon cancer usually begins with the basics. Then it becomes more personalized. That order matters because many patients hear about chemotherapy first and assume the path is fixed. It often isn’t.
The standard backbone
For localized disease, surgery is often the main treatment. In the ascending colon, that usually means removal of the tumor with the appropriate segment of colon and nearby lymph nodes. The goal is to remove all visible disease with clear margins and accurate nodal assessment.
After surgery, some patients need adjuvant chemotherapy and some do not. That decision depends on stage, pathology findings, and biomarker results. In early-stage disease, doctors pay close attention to risk features such as lymphovascular invasion, perineural invasion, tumor budding, and poor differentiation.
The value of early detection is clear in outcomes data. SEER benchmarks cited in the NCBI review report 5-year survival of 90.9% for localized disease and 73.4% for regional disease in colorectal cancer, reinforcing the importance of finding and treating disease before it spreads, as summarized in the NCBI review on colon cancer.
Why right-sided tumors often need a different lens
Ascending colon cancers are not just left-sided cancers in a different location. Many follow a distinct molecular route. The NCBI review notes that the CIMP pathway appears in about 15% of cases, often linked to a serrated polyp origin and co-occurring KRAS or BRAF mutations. Within that group, MSI-H tumors can have a better prognosis than hypermethylated tumors that are not MSI-H.
That biology affects treatment.
A right-sided tumor may be less likely to benefit from the same sequence of drugs that works well for a left-sided tumor. That’s why molecular testing is not a luxury in advanced disease. It’s part of choosing rational therapy.
How immunotherapy fits
When a tumor is MSI-H, immunotherapy may become one of the most important options. The basic idea is simple. Some tumors carry features that make them more visible to the immune system once immune “brakes” are released. Drugs such as pembrolizumab are designed to help the immune system recognize and attack those cancer cells more effectively.
For treatment-resistant disease, the reviewed data describes pembrolizumab for MSI-H tumors with objective response rates of 40 to 50% in that context, while also emphasizing lower-toxicity strategies.
If your cancer is advanced or has returned, ask a direct question. “Do we know whether this tumor is MSI-H, dMMR, KRAS-mutated, BRAF-mutated, or KRAS-wildtype?” Those answers can change the menu of treatment options.
Targeted therapy and why the marker matters
Some treatments are chosen because they block a specific growth signal the tumor relies on.
A few examples from the reviewed evidence:
- KRAS-wildtype tumors: anti-EGFR therapy such as cetuximab may play a role after certain chemotherapy combinations.
- BRAF V600E tumors: right-sided cancers are more likely to carry this marker, and targeted combinations such as encorafenib and binimetinib may be considered in the appropriate setting.
- Treatment-resistant disease: lower-dose or metronomic approaches may be used to reduce toxicity while continuing disease control efforts.
The same NCBI review cites the BEACON trial, where BRAF V600E disease treated with a triplet approach plus encorafenib/binimetinib showed median overall survival of 9 months versus 5.4 months in the comparison reported there.
For readers trying to understand common systemic drugs before discussing combinations, this overview of chemotherapy drugs for colon cancer can make those names easier to follow.
A practical treatment map
Different patients move through treatment in different ways, but the broad map often looks like this:
| Situation | Common treatment focus |
|---|---|
| Localized tumor | Surgery first, then decide on chemotherapy based on stage and risk features |
| Stage II with high-risk features | Careful review of pathology, MSI/MMR results, and whether adjuvant treatment adds value |
| Node-positive disease | Surgery plus systemic therapy is commonly considered |
| Metastatic or treatment-resistant disease | Biomarker-driven treatment, symptom control, and balancing efficacy with tolerability |
Where lower-toxicity care becomes important
Some patients can tolerate aggressive multi-drug treatment. Others can’t, or they’ve already had enough toxicity that quality of life becomes central to every decision. That’s where lower-dose regimens, treatment spacing, infusion planning, and supportive care become just as important as the drug list itself.
After surgery, daily logistics also matter more than people expect. Patients and caregivers often need practical help with mobility, bathing, wound protection, and home setup. A simple guide on recovering from surgery at home can make that period safer and less stressful.
The deeper point
The best treatment plan for ascending colon cancer is rarely “generic colon cancer care.” It’s a plan built from stage, anatomy, pathology, biomarkers, symptoms, prior treatment, and tolerance. That’s especially true when disease is advanced or standard approaches have already been used.
Understanding Your Prognosis and Future Outlook
Patients often hear the word prognosis and feel as if a final judgment has been handed down. That’s understandable, but it’s not the most useful way to think about it.
Prognosis is better understood as a decision-making tool. It helps doctors estimate risk, choose treatment intensity, and identify where newer therapies may matter most. It does not tell you exactly what will happen to one individual person.
Why right-sided cancers have worried doctors
Right-sided tumors, including ascending colon cancer, have historically raised concern because they often carry different biology and can be harder to detect early. A reviewed summary notes that right-sided tumors are more common in older patients and women and are more often MSI-H, BRAF-mutated, and HER2-amplified, with 5-year survival around 60% versus around 70% for left-sided tumors in the comparison cited there. The same summary notes that for MSI-H right-sided metastatic colorectal cancer, immunotherapy response rates have reached 40 to 50%, while MSS tumors had response rates of under 10% in the comparison discussed in the reviewed article on right-sided colorectal cancer challenges.
That sounds sobering, but it also shows something important. Biology can open doors. The same tumor features that once signaled a poorer outlook may now point toward more specialized treatment strategies.
What should shape your outlook today
A realistic prognosis discussion should include more than a stage number. It should also include:
- Tumor biology: MSI-H, KRAS, BRAF, HER2, and other markers can affect treatment options
- Pattern of spread: where the cancer has gone matters
- Symptoms and functional status: treatment has to fit the person, not just the scan
- Prior treatment history: what has worked, what caused toxicity, and what remains available
- Access to modern care: biomarker-driven care and clinical trial review can widen options
“What does my prognosis mean for treatment choices right now?” is often a better question than “What are my odds?”
Supportive care changes the picture too
Prognosis is not only about drugs. Nutrition, symptom control, hydration, mobility, treatment timing, and recovery support can influence how well someone tolerates therapy and whether they can stay on it.
Many patients benefit from structured, practical food planning during treatment. If you want ideas specific to cancer care needs, this resource on cancer-specific nutritional guidance may help you think through meals when appetite and energy are inconsistent.
Why hope should be concrete
Hope is most useful when it’s specific. Specific hope sounds like this: we have more than one line of treatment to discuss; we know the tumor’s markers; we can adjust intensity; we can manage symptoms better; we can look at clinical trials early instead of late.
That kind of hope is not denial. It’s strategy.
How Hirschfeld Oncology Can Help Chart Your Path
A diagnosis like ascending colon cancer often leaves families juggling two problems at once. First, the disease itself is complex. Second, the medical system can feel fragmented, especially when you need quick answers about biomarkers, treatment tolerance, symptom control, and whether there are options beyond a standard script.
That’s where a focused oncology consultation can help.
When a more tailored approach matters most
Some patients need a fresh review because the cancer is stage 4, has progressed after earlier treatment, or is causing symptoms that make aggressive therapy hard to tolerate. Others need help earlier, especially when pathology shows a right-sided tumor with features that may call for more individualized planning.
That need is becoming more urgent as the patient population changes. A reviewed summary on early-onset colorectal cancer notes that 20% of cases now occur under age 55, up from 11% in 1995, and that this group is projected to reach 10.9% of colon cancers in young adults by 2030. It also notes an estimated population attributable fraction of about 30% for obesity in the rise of early-onset disease, alongside alcohol and other biologic drivers, as discussed in the Fred Hutch review of early-onset colon cancer trends.
For younger patients and for anyone with subtle right-sided symptoms, delays can happen because the presentation may not look like the classic picture people expect.
What a comprehensive review should include
A meaningful second opinion or treatment-planning visit should look closely at the whole picture, not just the latest scan.
That usually means reviewing:
- Pathology in detail: including MSI/MMR and other biomarker data
- Prior treatment exposure: what was given, what worked, and what caused side effects
- Current goals: cure if possible, disease control, symptom relief, or preserving quality of life
- Tolerance and logistics: infusion schedule, neuropathy risk, fatigue, appetite, caregiver support
- Wellness factors: weight changes, alcohol use, inflammation, nutrition, and recovery planning
Why this matters for advanced care
Patients with right-sided or treatment-resistant disease often need plans that balance two truths at once. The cancer may require advanced treatment, and the patient may need something less toxic, not more punishing.
That can mean discussing immunotherapy when biomarkers fit, targeted therapy when mutations point in that direction, or carefully adjusted dosing when standard-intensity treatment is too hard on the body.
The right plan is not always the most aggressive plan. It’s the plan that matches the tumor’s biology and the patient’s real life.
A steadier next step
Families often feel better after a visit that turns scattered records into a coherent strategy. Even when the situation is serious, clarity lowers fear. It tells you what is known, what is still missing, and what options are reasonable now.
If you’re in Brooklyn, Williamsburg, Bushwick, or elsewhere in New York City, that kind of clarity can be the difference between feeling stuck and feeling prepared.
If you or someone you love is facing ascending colon cancer and wants a careful review of biomarker testing, immunotherapy options, low-dose chemotherapy strategies, targeted treatments, or supportive outpatient infusion care, consider scheduling a consultation with Hirschfeld Oncology. The goal isn’t just to name treatments. It’s to build a plan that fits the cancer, the person, and the life that treatment has to work within.
.png)
.png)




