




.png)


If you're reading this, you may already be seeing changes that feel frighteningly fast. A loved one who was talking a week ago may now sleep most of the day. Eating may have become difficult. Words may come out mixed up, or not come at all. Families often tell me the hardest part isn't only the sadness. It's not knowing what is expected, what is urgent, and how to help without causing more distress.
Brain cancer final stages often look different from the end of life in other cancers. The decline is usually driven by changes in brain function. That means families may see more drowsiness, confusion, swallowing trouble, weakness, personality change, or seizures, rather than a slow decline centered mainly on other organs. Understanding that pattern can make the days ahead less chaotic.
What follows is meant to be practical. It won't remove the grief, but it can help you recognize what's happening, make decisions earlier, and focus on comfort in a way that honors the person you love.
An Introduction for Patients and Families
Searching for information on the final stages of brain cancer takes immense courage. Individuals often seek these details late at night, following a difficult conversation, a sudden setback, or a day when a clear change has occurred. If that is where you find yourself right now, your fear is entirely understandable.
One of the most painful parts of this stage is uncertainty. Families often wonder whether more sleep means the end is near, whether less eating is a choice or part of the disease, and whether they should call the oncologist, hospice, or 911. Those questions are common, and asking them doesn't mean you're giving up. It means you're trying to care well.
Why this stage feels so different
In advanced brain cancer, the person is often changing because the brain is under pressure and losing function in specific areas. That can affect wakefulness, swallowing, speech, movement, memory, and behavior. So the final stage is often less about one dramatic moment and more about a series of neurologic losses that can unfold over days to weeks, and sometimes unevenly.
A person may still recognize a voice even when they can't answer. They may stop wanting food because swallowing has become hard, not because they're refusing comfort. They may seem restless or confused because the brain is struggling, not because they're upset with you.
You don't need to have every answer today. You need a clear plan for comfort, safety, and support.
What families usually need most
Most caregivers need three things at this point:
- A plain-language roadmap so changes feel less mysterious.
- A symptom plan for seizures, swallowing trouble, agitation, pain, and sleepiness.
- Practical support for the emotional and logistical strain of caregiving.
If you also need broader help with coping, transportation, finances, or caregiver support, these cancer patient resources and support tools can help you identify what to ask for and where to start.
Understanding the Final Stages of Brain Cancer
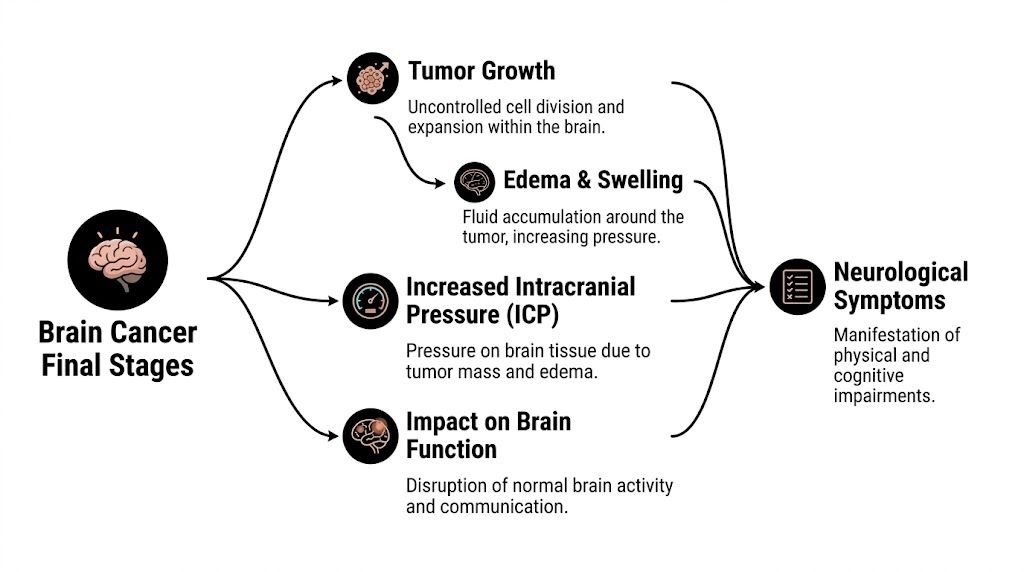
In the final stage, the main problem is usually progressive neurologic failure. The tumor grows, and the tissue around it may swell. That swelling, often called edema, raises pressure inside the skull. Unlike other parts of the body, the brain doesn't have extra room to expand, so even modest increases in pressure can interfere with alertness, movement, speech, and swallowing.
A simple way to think about it is this. The brain is like a crowded control center inside a fixed box. When a tumor and swelling take up more space, the control center can't send clean signals. That's why families often notice a sequence of changes rather than one isolated symptom.
What this decline commonly looks like
In a study of high-grade glioma patients at the end of life, progressive drowsiness or loss of consciousness occurred in 87%, difficulty swallowing in 71%, focal neurologic deficits in 51%, and seizures in 45% according to this end-of-life glioma study. Those numbers matter because they show a pattern. People often become sleepier, less able to eat safely, and less able to move or communicate as brain function declines.
That pattern is different from what many families expect. They may assume headaches or pain will be the main issue. Sometimes they are. But in brain cancer final stages, the more defining changes are often these:
- Increasing sleepiness: The person may spend most of the day asleep and be harder to wake.
- Swallowing problems: Pills, water, and food may trigger coughing, pocketing food, or refusal because swallowing feels unsafe.
- Focal deficits: One arm or leg may weaken, speech may become slurred, or one side of the face may droop.
- Seizures: These may be dramatic, but they can also be subtle, such as staring, lip-smacking, or sudden unresponsiveness.
Why families often feel unprepared
General end-of-life checklists don't always capture the brain-specific nature of this decline. That's why it helps to review both practical end-of-life signs caregivers may notice and broader guidance on comforting families during hospice when the changes start accelerating.
Practical rule: Worsening swallowing and decreasing alertness are often signs that daily care needs are about to increase quickly.
A person may still have meaningful moments. A good morning doesn't cancel a larger decline. Brain cancer can fluctuate. Families often feel confused when someone seems more awake for a few hours and then much worse by evening. That's common, and it doesn't mean anyone caused the setback.
Navigating Prognosis and Individual Timelines
The question families usually ask, or sometimes immediately, is, "How long?" It's an understandable question, but it rarely has a clean answer in brain cancer final stages. Doctors often speak in ranges because prognosis depends on far more than the word "brain cancer."
Why timelines vary so much
Tumor type matters enormously. For glioblastoma, one of the most aggressive brain cancers, the 5-year relative survival is about 5.7%, and survival is commonly 12 to 18 months after diagnosis, though the range is wide, as summarized by Roswell Park's brain cancer survival overview. Those figures are useful for context, not prediction.
Other tumors behave very differently. Some progress quickly. Others move more slowly or respond for longer periods. Age, tumor biology, treatment response, and the person's overall condition all shape what happens next.
Here is the key point families often need to hear more than once: population averages are not personal deadlines.
How to use prognosis without letting it control everything
A prognosis is best used as a planning tool. It helps families decide when to prioritize time together, when to simplify treatment goals, and when to bring in more support at home. It shouldn't be treated as a countdown clock.
When your medical team gives a range such as "weeks to months," they're usually combining several observations:
- How quickly function is changing
- Whether the person can still swallow safely
- How much time is spent awake
- Whether seizures, confusion, or weakness are worsening
- Whether treatment is still helping
Hospice and palliative care aren't signs that the team is stepping back. They're signs that the team is matching care to what the body is doing now.
Families sometimes delay comfort-focused care because it feels emotionally loaded. In practice, earlier support often means better symptom control, fewer frantic decisions, and more time spent at home in a calmer way. When the likely trajectory is shortening, choosing comfort isn't surrender. It's a medical decision to protect dignity and reduce suffering.
Shifting to Comfort with Palliative and Hospice Care
There comes a point when the most important question is no longer, "What else can treat the tumor?" It becomes, "What will make this person safest and most comfortable now?" That's the heart of palliative and hospice care.
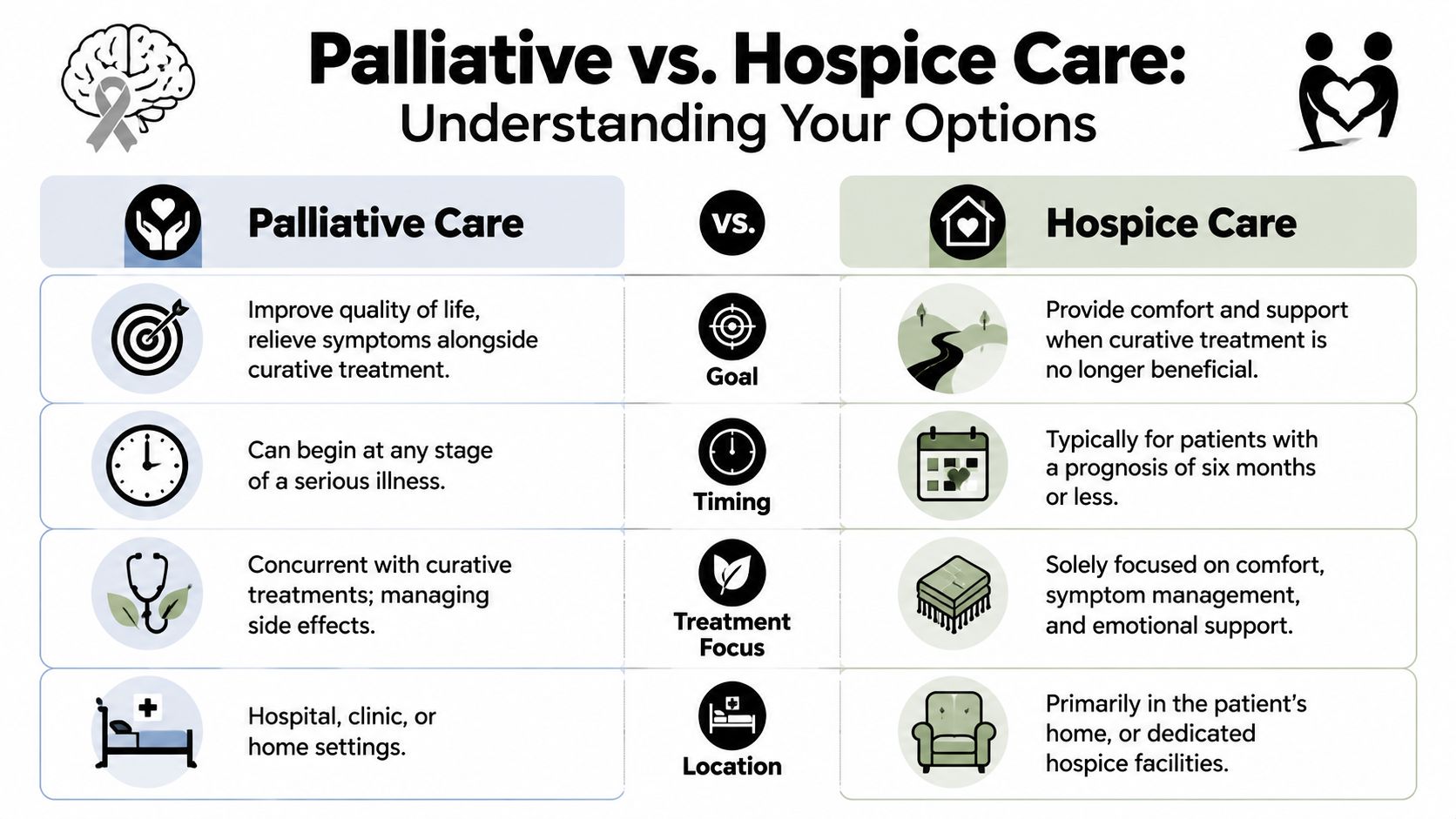
The difference in plain language
Palliative care helps with symptoms and quality of life during serious illness. It can be added alongside treatments. Hospice care is used when treatment is no longer controlling the cancer and the focus shifts fully to comfort.
Mayo Clinic notes that in end-stage brain cancer, care shifts toward comfort and safety, and hospice is often considered when life expectancy is estimated at six months or less, with care centered on symptoms such as swelling, seizures, and pain, as described in this Mayo Clinic guide to grade 4 brain cancer end-stage care.
Families often need to hear what hospice does. Hospice doesn't mean "nothing." It means active care with different goals.
- Nursing support: Monitoring symptoms, adjusting comfort plans, and helping families know what's expected.
- Medication guidance: Managing swelling, seizures, pain, agitation, and respiratory changes.
- Home equipment: Helping arrange practical items that make care safer and easier.
- Emotional and spiritual support: Supporting both the patient and the people caring for them.
For families who want a basic orientation before enrolling, this guide to hospice for families can make the process feel less unfamiliar.
A concise side-by-side explanation can also help when relatives disagree about next steps. This overview of palliative care and hospice differences is useful when family members are using the terms interchangeably.
Later in the decision process, some families find it helpful to watch a short video together and pause to talk through concerns.
When to ask for hospice now, not later
Consider asking for a hospice evaluation if you're seeing several of these changes at once:
- More bedbound time: The person needs much more help getting up, turning, or using the bathroom.
- Less safe swallowing: Pills or sips of water are increasingly difficult.
- Longer sleeping periods: Waking becomes harder, and conversations are brief or absent.
- Fast cognitive decline: Confusion, disorientation, or reduced interaction is becoming the norm.
Earlier hospice involvement often gives families more support, not less hope.
Practical Symptom Management for Better Quality of Life
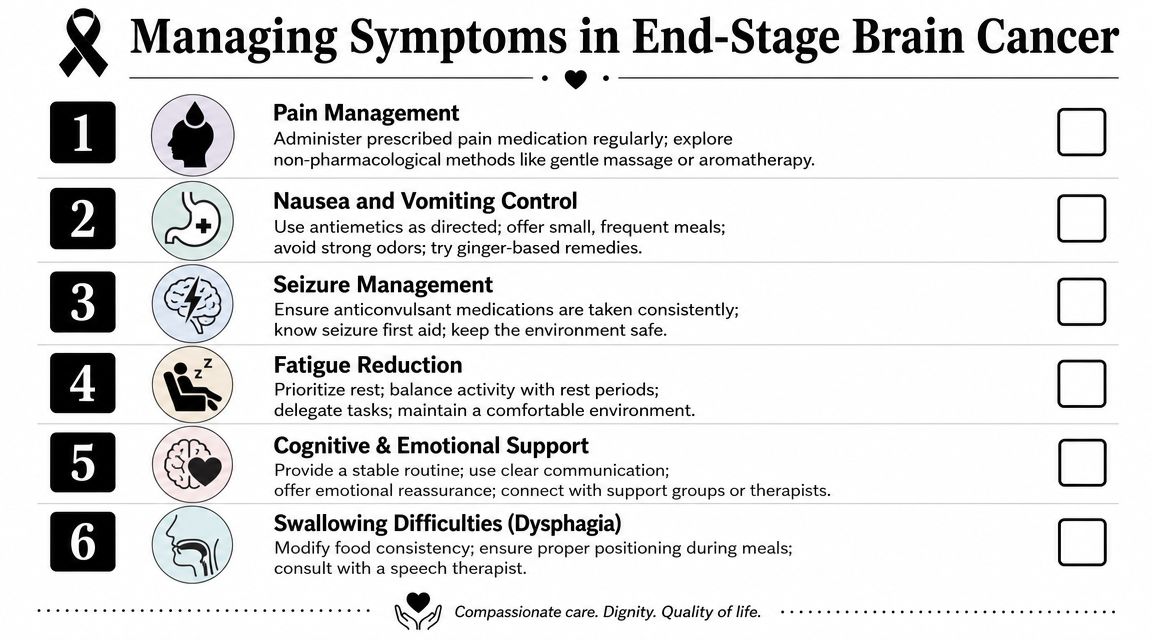
Families usually don't need abstract advice at this point. They need to know what to do at 2 a.m. when the person won't swallow a pill, becomes suddenly agitated, or seems too sleepy to eat. Good symptom management starts with accepting that comfort, not forcing normal routines, is the priority.
What helps most at home
A calmer home setup often matters as much as medication timing. Lower noise. Keep lighting soft. Limit the number of people talking at once. Use short sentences and one-step instructions.
If swallowing is difficult, don't push full meals because that was the old routine. Offer comfort in smaller ways.
| Situation | What families can try |
|---|---|
| Trouble swallowing | Sit the person upright, offer small sips or tiny bites only if they're awake enough, and stop if coughing starts |
| Increasing sleepiness | Time care for wakeful moments, cluster tasks, and let rest take priority |
| Weakness or imbalance | Keep pathways clear, use close supervision during transfers, and avoid rushing |
| Confusion or aphasia | Use simple questions, a calm tone, and reassurance more than correction |
Seizures, agitation, and communication
Seizures can be frightening, especially if they happen at home. During a seizure, protect the person from injury, turn them to the side if you can do so safely, and don't put anything in their mouth. Afterward, many people are sleepy or confused. That doesn't necessarily mean a new catastrophe occurred, but it does mean the care team should know if seizures are increasing or changing.
Agitation is also common. Sometimes it looks like picking at sheets, trying to get out of bed, or seeming afraid. Families often respond by arguing, correcting, or asking too many questions. A better approach is quieter and simpler.
- Use reassurance first: "You're safe. I'm here."
- Reduce stimulation: Turn off the television and lower the room noise.
- Check for discomfort: Positioning, bladder needs, constipation, or medication timing may be contributing.
- Call for medication advice: Hospice or the palliative team can often adjust the plan.
Communication may fade before awareness does. A person who can't speak much may still hear your voice and respond to touch or familiar music. Keep talking normally. Say who you are. Say what you're doing. Offer comfort, not tests.
Try not to measure connection only by words. Many patients remain comforted by tone, touch, and presence even when speech is limited.
Food and fluids near the end
Reduced appetite is one of the hardest changes for families to accept. Feeding someone is such a basic act of love that less eating can feel wrong. But near the end of life, the body often doesn't process food and fluids the way it once did. Forcing intake can increase distress, coughing, or choking.
Focus on comfort instead:
- Mouth care matters: Moisturizing the lips and mouth often brings more relief than urging food.
- Offer, don't insist: Let the person's alertness guide what is safe.
- Ask about medication forms: If pills become hard to swallow, the care team may suggest alternatives.
Essential Conversations and End-of-Life Decisions
A family often reaches this stage in pieces, not all at once. One daughter notices more confusion. A spouse sees that walking to the bathroom now takes two people. A son hears coughing after every sip of water. Nobody wants to say, "I think we're nearing the end," because saying it out loud can feel like causing it.
A day that changes the conversation
Morning may begin with a small shock. Your loved one doesn't want breakfast and can't follow a familiar conversation. By afternoon, they're sleeping through most questions. At dinner, they cough on water and turn away from food. That kind of day is often the moment families realize they need more than encouragement. They need decisions.
In this moment, clear, gentle questions help:
- "If things change quickly, what would feel most important to you?"
- "Would you want to stay home if possible?"
- "Who should speak for you if you can't speak for yourself?"
Palliative care experts emphasize that rapid changes in cognitive function or a steep functional decline are reasons to revisit advance care plans and consider hospice, and that these conversations should happen early and then be revisited at key milestones, as outlined in this palliative care guidance for glioblastoma.
What decisions matter most
You don't need a perfect script. You do need clarity on a few major issues.
- Decision-maker: Make sure the family knows who the medical decision-maker is.
- Care setting: Decide whether the priority is staying at home, going to the hospital for reversible problems, or avoiding emergency transfers when possible.
- Emergency threshold: Ask the team which changes should trigger a hospice call and which require emergency services.
- Personal wishes: Some people want quiet, familiar music, prayer, or certain people nearby. Those preferences matter.
For families who also need help understanding formal planning and legal roles, especially when someone may lose decision-making capacity, this Law Office of Bryan Fagan end-of-life guidance offers a general explanation of how guardianship and planning can intersect.
The best time to talk is before a crisis, but the second-best time is today.
These conversations aren't only about paperwork. They're also about reducing regret. When families know the person's wishes, they suffer less second-guessing later.
How Hirschfeld Oncology Supports Patients and Families in NYC
In New York City, care can be medically advanced and still feel fragmented. Families may have specialists in different systems, pharmacies with delays, home care questions, and work or transportation pressures layered on top of grief. End-stage cancer care often fails not because help doesn't exist, but because coordination breaks down.
Research on brain-tumor care highlights that the burden on families is often not only medical. Financial concerns, caregiver strain, and access barriers can shape the final stage just as powerfully as symptoms themselves. That same need for coordinated support is emphasized in this study on psychosocial and practical burdens in brain tumor care.

That is where a practice-based team can help steady the process. In the NYC setting, families often need help with symptom review, treatment reassessment, palliative coordination, and practical next steps when the situation changes quickly. Hirschfeld Oncology provides outpatient oncology care in Brooklyn and works with patients and families who need close monitoring, collaborative decision-making, and support that takes quality of life seriously.
What support should look like in real life
A useful cancer team in this phase helps families do things such as:
- Clarify priorities: Are you still pursuing treatment, or has the focus shifted primarily to comfort?
- Coordinate services: Palliative care, hospice, social work, infusion planning, and outside specialists need to work from the same plan.
- Reduce avoidable crises: Families need someone to call before a symptom becomes an emergency room visit.
- Support caregivers: The caregiver's capacity matters. If the plan is unrealistic, it won't hold.
For patients and families in Brooklyn, Williamsburg, Bushwick, and nearby neighborhoods, local access matters because changes can happen quickly in brain cancer final stages. A team that communicates clearly and helps organize the next step can make an overwhelming period more manageable.
If you or someone you love is facing advanced cancer and needs help thinking through symptoms, goals of care, or next steps, Hirschfeld Oncology offers educational resources and a path to consultation in NYC. The right support can help you make decisions with more clarity, more comfort, and less confusion.
.png)
.png)




