




.png)


Yes, a rash can be a sign of cancer in some cases, including skin cancer, certain blood cancers, and internal tumors that trigger skin changes. But most rashes are not cancer, and the helpful question isn't "Is every rash dangerous?" It's "What kind of rash is acting differently from an ordinary one?"
If you're reading this because you've had a patch of skin that won't go away, keeps coming back, or just doesn't seem to fit the usual eczema or allergy pattern, that concern is understandable. The good news is that there are specific clues doctors use to sort out a common rash from one that needs a closer look. Once you know those clues, the next step feels much less mysterious.
That Persistent Rash What It Could Mean
A very common story starts like this. You notice a red, itchy, or scaly patch. You try moisturizer, an over-the-counter cream, or you wait for it to settle down. Instead of fading, it stays put. Sometimes it slowly changes. Sometimes it bleeds, thickens, or shows up in a place that seems unusual.
That doesn't automatically mean cancer. In day-to-day practice, most rashes are still things like irritation, eczema, psoriasis, fungal infections, allergic reactions, or medication effects. But some skin changes deserve more respect because they don't behave like a routine rash.
Three different ways cancer and rashes can be connected
Doctors usually think about this question in three distinct categories:
- The rash is a skin cancer. A lesion may look like a rash at first, but the abnormal cells are in the skin itself.
- The rash reflects a blood cancer involving the skin. Some lymphomas and leukemic conditions can appear first as rash-like patches or widespread redness.
- The rash is a signal from a cancer somewhere else in the body. In these cases, the skin isn't the primary site of cancer. It's reacting to hormones or other substances made by a tumor.
That distinction matters because each category has a different pattern, a different workup, and a different treatment path.
Practical rule: A rash that persists, evolves, or ignores standard treatment deserves a professional exam, even if it doesn't look dramatic.
What usually makes doctors pause
A concerning rash often stands out by behavior more than appearance alone.
- It persists: It doesn't fade the way a typical irritation should.
- It changes: It grows, becomes shinier, crusts, bleeds, or spreads in a specific pattern.
- It resists treatment: Moisturizers, topical steroids, or routine skin care don't help.
- It appears with other symptoms: Weight loss, fatigue, sores, lumps, or a general sense that something isn't right.
The goal isn't to make you inspect every freckle with fear. It's to help you notice when a skin change is asking for more than guesswork.
When the Rash Is the Cancer Direct Skin Involvement
A common real-world scenario goes like this. You notice a rough patch on the arm or face, assume it is dry skin, and give it time. Weeks pass. Then months. It still has not cleared.
Sometimes that kind of stubborn skin change is concerning for a simple reason. The abnormal cells are in the skin itself.
Skin cancer is common. One in five Americans will develop skin cancer during their lifetime, and non-melanoma skin cancers such as basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) can look like persistent rashes, scaly patches, or pearly bumps that do not respond to standard treatments, according to Potozkin + Ellis on skin cancer that masquerades as common conditions.

Basal cell and squamous cell cancers can look surprisingly ordinary
This is one of the easiest places to get misled. Many skin cancers do not announce themselves with dramatic pain or a shocking appearance.
A basal cell carcinoma often appears as a shiny bump, a pink spot, or a sore that heals partway and returns. A squamous cell carcinoma may look more like a rough red patch, a crusted area, or a thickened scaly spot. To a patient, and sometimes even to a non-specialist at first glance, these can resemble eczema, irritation, or a rash from friction.
The clue is often their behavior over time. A harmless rash usually settles down when the trigger is removed or the skin is treated. A cancerous lesion tends to hold its ground. It lingers in one area, slowly changes, and may start to bleed, crust, or feel tender.
Melanoma usually behaves differently
Melanoma is less likely to present as a classic rash. It more often shows up as a changing mole or a new dark spot that does not fit the pattern of your other moles.
Doctors often use the ABCDE rule to teach what to watch for:
- Asymmetry
- Border irregularity
- Color variation
- Diameter greater than 6 mm
- Evolving
That last word, evolving, often matters most. In clinic, change over time is one of the strongest reasons to stop guessing and examine the spot closely.
Some cancers that start in the skin can mimic inflammatory rashes
Direct skin involvement is not limited to the more familiar sun-related skin cancers. Some cancers arise from immune cells in the skin and can look rash-like for quite a while.
One important example is mycosis fungoides, the most common form of cutaneous T-cell lymphoma. Early on, it may appear as flat, itchy patches that resemble eczema or psoriasis. These areas often show up on parts of the body that do not get much sun, such as the buttocks or trunk. They can persist and slowly evolve.
For this reason, an experienced evaluation matters. At an advanced oncology clinic such as Hirschfeld Oncology, the question is not just, "What does this look like today?" The better question is, "What pattern has it followed, and what diagnosis would explain that pattern?" That step-by-step approach helps separate common skin conditions from the smaller group of cases that need biopsy, staging, or specialized cancer care.
A related condition called Sézary syndrome is much less common but more aggressive. It can cause diffuse redness and itching over most of the body. When a rash is this widespread, persistent, and paired with other signs that something is wrong, doctors broaden the workup quickly.
A skin change that stays in one place, keeps returning, or gradually becomes more noticeable deserves a professional exam. The goal is not panic. The goal is clarity.
When a Rash Signals a Deeper Cancer Paraneoplastic Syndromes
A second kind of connection is less intuitive. The rash isn't the cancer itself. It's more like a smoke signal from a tumor somewhere else in the body.

The skin can react to chemicals made by a tumor
This is called a paraneoplastic syndrome. In plain language, a cancer in one organ can release hormones or other substances that affect tissues far away. The skin may be the first place that reaction becomes visible.
One of the clearest examples comes from a rare pancreatic neuroendocrine tumor called a glucagonoma. In this setting, excess glucagon can trigger necrolytic migratory erythema, usually shortened to NME.
A concrete example called necrolytic migratory erythema
In pancreatic neuroendocrine tumors, specifically glucagonomas, NME affects up to 70% to 90% of patients and may appear 1 to 2 years before tumor diagnosis in 30% of cases, according to Healthgrades on skin signs of pancreatic cancer. The rash often shows up as blistering plaques on the limbs and perineum.
Those details matter because NME doesn't behave like a simple allergic breakout. It tends to be unusual in both appearance and pattern. It can involve red inflamed areas with blistering and healing in one part while new areas appear nearby.
Here is a short video that helps put the idea of cancer-related skin changes into context:
Why this category confuses people
People naturally assume a rash must come from a skin problem. Paraneoplastic rashes break that rule. The skin may be reacting to an internal process rather than a problem that started in the skin itself.
That can make the symptoms feel disconnected. A person may focus on creams, soaps, and detergents when the underlying issue is hormonal or metabolic.
- Direct skin cancer: The abnormal cells are in the skin lesion.
- Paraneoplastic rash: The skin is reacting to a tumor located elsewhere.
- Treatment implication: The rash often improves only when doctors address the underlying cancer.
If a rash has a strange pattern, keeps recurring, and travels with other unexplained symptoms, your doctor may look beyond dermatology alone.
This is one reason cancer care often involves both dermatology and oncology. The skin can provide an early clue, but the diagnosis may depend on connecting that clue to the rest of the body.
A Visual Guide to Cancer-Related Rashes and Red Flags
Some readers want examples. Others want a clean framework. This section is for both.
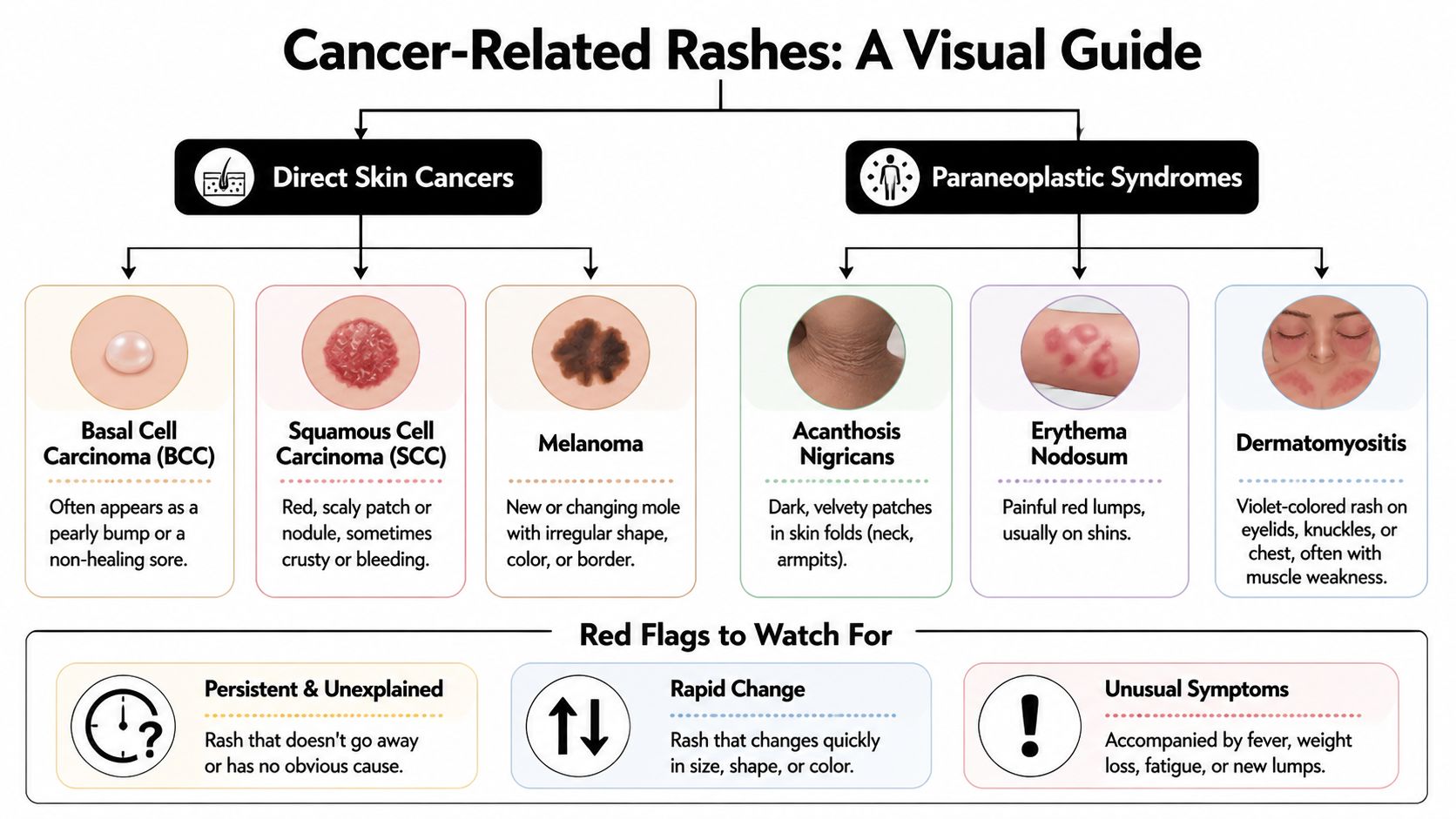
Common patterns of cancer-related skin changes
| Rash Name / Type | Typical Appearance | Commonly Associated Cancers |
|---|---|---|
| Basal cell carcinoma | Pearly bump, non-healing sore, sometimes shiny | Skin cancer |
| Squamous cell carcinoma | Red scaly patch, crusted or rough nodule | Skin cancer |
| Melanoma | New or changing pigmented spot, irregular shape or color | Skin cancer |
| Mycosis fungoides | Itchy patch or plaque that can resemble eczema or psoriasis | Cutaneous T-cell lymphoma |
| Sézary syndrome | Widespread itchy red rash over much of the body | Aggressive cutaneous T-cell lymphoma |
| Necrolytic migratory erythema | Blistering, inflamed plaques that can migrate or recur | Glucagonoma, a pancreatic neuroendocrine tumor |
| Leukemia cutis or related leukemia-associated skin changes | Petechiae, purpura, or rash-like lesions | Leukemia |
| Kaposi sarcoma | Deep red or purple lesions | Vascular tumor, often in immunocompromised patients |
| Acanthosis nigricans | Dark, velvety patches in skin folds | Can be associated with internal malignancy in some settings |
| Dermatomyositis-type rash | Violet or red-violet rash on eyelids, knuckles, or chest | Can be associated with underlying malignancy |
Red flags worth acting on
You don't need to identify the exact diagnosis yourself. You only need to know when a rash isn't behaving normally.
- Persistent and unexplained: It stays despite routine treatment and there's no clear trigger.
- Rapid change: It changes in size, shape, color, thickness, or surface.
- Bleeding or oozing: Especially when the area began as a patch that seemed harmless.
- Odd color signals: Deep red, purple, or mixed-color lesions deserve attention.
- Whole-body clues: Fever, fatigue, weight loss, swollen nodes, sores, or new lumps alongside the rash.
One helpful way to think about it
A routine rash usually makes sense in context. Maybe you changed soaps, started a new medication, got dry skin in winter, or have a history of eczema. A concerning rash often feels out of proportion, persistent, or disconnected from the usual explanations.
That's when a clinician stops asking, "What cream should we try next?" and starts asking, "Should we biopsy this, or should we look for something deeper?"
Distinguishing Cancerous Rashes from Common Skin Issues
This is the part many people need most. Most itchy, flaky, red skin changes are still far more likely to be ordinary skin conditions than cancer.

What common rashes usually do
Eczema, psoriasis, hives, and contact dermatitis often follow recognizable patterns.
- Eczema: Often itches intensely, flares with dryness or irritants, and may improve with moisturizers or topical steroids.
- Psoriasis: Often forms thicker scaly plaques and tends to recur in familiar body areas.
- Hives: Usually come and go quickly, often shifting location.
- Contact dermatitis: Often tracks with exposure to a product, metal, plant, or fabric.
If your symptoms fit an allergy pattern, practical background reading like Salus Natural Medicine on allergies can help you think through common triggers and reactions before you panic.
What tends to make doctors more suspicious
The issue isn't that cancerous rashes always look dramatic. It's that they often fail the common-rash test.
| Feature | More typical of common skin conditions | More concerning for cancer-related change |
|---|---|---|
| Timing | Comes and goes | Persists or slowly worsens |
| Response to creams | Often improves | Often doesn't improve |
| Distribution | May be widespread or linked to exposure | May stay localized or follow an unusual pattern |
| Surface behavior | Itchy, inflamed, flaky | May become shiny, crusted, bleed, thicken, or ulcerate |
| Associated clues | Allergy history, irritant exposure, seasonal flares | Weight loss, fatigue, sores, lumps, unexplained progression |
One important source of confusion in cancer care
Some rashes in people with cancer aren't caused by the cancer at all. They may come from treatment. Targeted therapy, for example, can cause skin side effects that look alarming but mean something very different clinically. If that's relevant to you, this overview of targeted cancer therapy side effects gives useful context.
The question isn't only "What does it look like?" It's also "How has it behaved over time?"
That's why doctors ask about timing, treatments tried, body location, and whether the rash has evolved. Those details often matter more than a phone photo taken on a single day.
The Diagnostic Journey What to Expect from Your Doctor
You notice a rash that has stayed longer than it should. You have tried creams, changed soaps, maybe even told yourself it is probably nothing. By the time you make the appointment, the hardest part is often the uncertainty.
A good evaluation turns that uncertainty into a series of clear questions.
At a clinic that sees complex cancer cases, including Hirschfeld Oncology and its dermatology and pathology partners, the goal is not to label every unusual rash as cancer. The goal is to sort out what kind of connection, if any, may be present. Is the skin itself the main problem? Is the rash a clue to a blood cancer? Or is it a skin signal from a cancer elsewhere in the body? That framework helps doctors choose the right tests instead of guessing.
The first visit usually starts with the story
Doctors look at a rash the way a mechanic listens to an engine. The sound matters, but the history often tells you more. A rash that appeared after a new detergent points in one direction. A patch that has slowly thickened, spread, or stopped responding to standard treatment points in another.
Expect questions like these:
- When did it start, and how has it changed over time?
- Does it itch, hurt, bleed, crust, or ulcerate?
- What treatments have you already tried, and what happened?
- Is it staying in one place or appearing in several areas?
- Have you had fevers, weight loss, swollen nodes, fatigue, or other new symptoms?
- Do you have a history of eczema, psoriasis, skin cancer, heavy sun exposure, or another cancer?
The physical exam may be focused or broad. If one spot looks suspicious, your doctor may examine the rest of the skin too, because pattern and distribution can change the meaning of what they see.
Why a biopsy is often the turning point
Some rashes can be identified by appearance and history. Others cannot. Early mycosis fungoides is a classic example because it can resemble eczema or dermatitis for a long time.
That is why biopsy matters. It gives the pathologist actual tissue to examine under the microscope, including whether abnormal lymphocytes or other cancer-related changes are present.
A biopsy does not mean your doctor thinks cancer is certain. It means the rash has raised a question that only tissue can answer.
Usually, the sample is small and done with local numbing medicine. Patients often worry that biopsy is a major procedure. In many cases, it is a brief office procedure with mild soreness afterward.
What happens after the biopsy depends on what the tissue shows
If the findings fit a common inflammatory skin condition, treatment may shift back toward dermatology care with a clearer plan. If the biopsy suggests skin cancer, a cutaneous lymphoma, leukemia-related involvement, or a paraneoplastic process, the next step is to define the full picture, not just the skin finding.
That may include:
- Blood tests to look for signs of a blood disorder or systemic inflammation.
- Imaging if there is concern about disease outside the skin.
- Special pathology review when the pattern is subtle or uncommon.
- Coordinated care between dermatology, oncology, and other specialists.
This step-by-step approach is a big part of how advanced oncology clinics handle difficult cases. The question is not only, "What is this rash?" It is also, "What does this rash tell us about the rest of the body?"
If you are preparing for that kind of evaluation, this guide to what to expect at a first oncology appointment can help the visit feel more predictable.
What you can do before the appointment
Small details help more than people expect.
- Write a short timeline. Note when the rash began and how it has evolved.
- List everything you tried. Include prescription creams, over-the-counter products, antibiotics, antifungals, and steroids.
- Bring photos from earlier stages. A rash may look different in clinic than it did two weeks ago.
- Note other body changes. Fatigue, swollen glands, fevers, mouth sores, night sweats, or new lumps can matter.
You do not need to arrive with a diagnosis. You just need to bring the clues. That gives your doctor a better chance of finding the right explanation quickly.
How Hirschfeld Oncology Can Help Chart Your Path Forward
When a rash turns out to be connected to a complex or advanced cancer, the next step isn't just "treat the skin." Doctors need to treat the underlying disease while also making daily life more manageable.
That dual focus matters. A painful or persistent skin problem can affect sleep, concentration, confidence, and willingness to continue treatment. Good oncology care takes those effects seriously instead of treating them as a side note.
A thoughtful plan usually works on two tracks
The first track is cancer control. Depending on the diagnosis, that may involve immunotherapy, targeted therapy, low-dose chemotherapy, or another personalized regimen designed around the biology of the tumor and the patient's goals.
The second track is symptom support. That can include itch relief, wound care, infection prevention, treatment adjustments, and coordination with dermatology and infusion teams.
Why specialized input can matter
People with treatment-resistant disease or advanced-stage diagnoses often need more than a standard template. They may need a team that can weigh emerging options, monitor tolerability closely, and adjust strategy when the first plan stops working.
For patients seeking that level of outpatient oncology support in New York City, Hirschfeld Oncology's Brooklyn cancer center overview shows how a community-based practice can combine access, experience, and individualized care.
Good cancer care doesn't separate disease control from quality of life. It addresses both at the same time.
Families often need guidance too. Skin findings can be frightening because they're visible every day. Clear explanations, close follow-up, and a realistic treatment plan can reduce that sense of chaos and help everyone focus on the next right step.
Frequently Asked Questions About Rashes and Cancer
Is an itchy rash usually cancer?
No. Most itchy rashes are not cancer. Itch by itself is common in allergies, eczema, dry skin, and irritation. Doctors get more concerned when the rash persists, changes, or doesn't respond to appropriate treatment.
Can skin cancer really look like eczema?
Yes, it can. Some basal cell and squamous cell cancers can resemble a stubborn patch of dermatitis. That's one reason a rash that stays fixed and doesn't improve should be examined.
If a rash comes and goes, is that reassuring?
Usually, yes. Many ordinary rashes flare and settle. Cancer-related skin lesions are often more persistent or progressively changing. Still, recurring unusual rashes should be discussed with a clinician.
Does a biopsy mean my doctor thinks I definitely have cancer?
No. A biopsy means the doctor needs a tissue diagnosis because the appearance alone isn't reliable enough.
Should I see a dermatologist or an oncologist first?
A primary care doctor or dermatologist is the best first stop. If testing suggests cancer, oncology becomes part of the team quickly.
If you're dealing with a persistent rash alongside a cancer diagnosis, or you've been told a skin change may be related to an advanced or treatment-resistant tumor, Hirschfeld Oncology offers compassionate, individualized care for patients in Brooklyn and across New York City. Their team focuses on thoughtful treatment planning, close monitoring, and options designed to balance effectiveness with quality of life.
.png)
.png)




