




.png)


A diagnosis often arrives in fragments. A scan result. A biopsy call. A new word you didn't expect to hear, like adenocarcinoma or squamous cell carcinoma. By the time you get home, you may know that something serious is happening, but not yet understand what that label means for treatment, prognosis, or the next appointment.
That uncertainty is hard on patients and families alike. Patients and their families don't need more medical jargon. They need a clear explanation of what kind of esophageal cancer they're dealing with, why that type matters, and how it changes the path forward. The details matter because esophageal cancer types are not interchangeable diagnoses. They can arise from different cells, reflect different risk factors, and lead your oncology team toward different treatment decisions.
Navigating Your Esophageal Cancer Diagnosis
When you first hear “esophageal cancer,” it can sound like a single disease with a single plan. In practice, your doctors are sorting out several different questions at once. What type is it? Where in the esophagus did it start? How deep has it grown? Has it spread? Are you strong enough for surgery, or would another approach fit better?
Those questions aren't academic. They shape real decisions about whether you may need surgery, chemotherapy, radiation, endoscopic treatment, or some combination of them. They also influence how your doctors think about symptom control, nutrition support, and what to do if the cancer is advanced or stops responding to standard therapy.
The first report that matters most
For many families, the biopsy report feels dense and frightening. But one line in that report is often the key that reveals the rest of the conversation: the histology, or cell type.
The two labels you'll hear most often are:
Adenocarcinoma
Cancer arising from gland-like cells, usually near the lower esophagus where it meets the stomach.Squamous cell carcinoma
Cancer arising from the flat lining cells of the esophagus.
A patient may ask, “Isn't cancer just cancer?” It's a fair question. The answer is no. These two cancers can behave differently enough that doctors often think of them as related but distinct diseases.
Practical rule: When you meet your oncology team, ask them to state your diagnosis in one full sentence, including the cancer type, location, and stage if known.
What your family should focus on right now
In the first days after diagnosis, try to narrow the flood of information to a few essentials:
- Confirm the exact type from the pathology report.
- Learn the location of the tumor in the esophagus.
- Ask what staging tests are still needed.
- Discuss whether the goal is cure, disease control, or symptom relief.
- Bring someone with you to appointments so another person can take notes.
If you can answer those five points, you'll already be in a much stronger position for the decisions ahead.
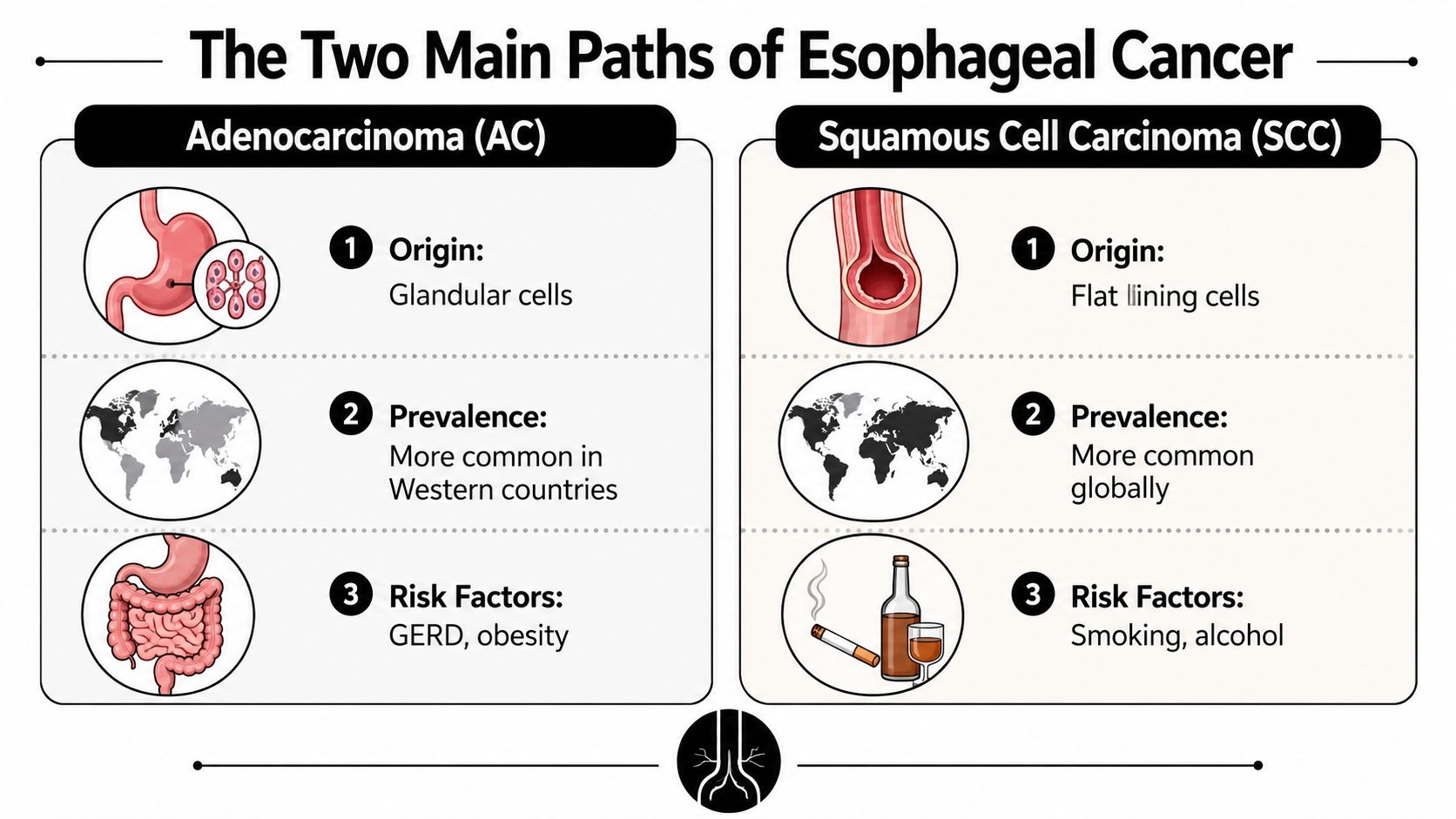
The Two Main Paths of Esophageal Cancer
Two major forms dominate discussions about esophageal cancer types: adenocarcinoma (AC) and squamous cell carcinoma (SCC). They both start in the esophagus, but they come from different cells and often follow different biological paths. A useful way to think about them is as two different trees growing in the same forest. They share the same location, but their roots, growth patterns, and care needs aren't the same.
Early on, a lot of confusion comes from hearing one general cancer name while the important details sit in the fine print. This is one reason treatment conversations can sound so specific.
Here's a visual comparison to ground the basics:
Why these two diagnoses are discussed separately
Globally, squamous cell carcinoma is the most common type and accounts for approximately 90% of all cases worldwide, while adenocarcinoma is the predominant type in high-income regions such as the United States, where it represents over 50% of cases according to the World Gastroenterology Organisation review on geographic variation in esophageal cancer.
That difference reflects more than geography. It points to different risk environments, different patient histories, and often different tumor locations.
A side-by-side view helps:
| Feature | Adenocarcinoma (AC) | Squamous Cell Carcinoma (SCC) |
|---|---|---|
| Cell of origin | Gland-like cells | Flat lining cells |
| Typical setting | More common in North America and Western Europe | More common globally |
| Common risk pattern | Chronic reflux, Barrett's esophagus, obesity, smoking | Tobacco use, heavy alcohol use, lower socioeconomic conditions |
| Usual clinical impression | Often tied to long-standing acid exposure near the lower esophagus | Often tied to injury of the esophageal lining from other exposures |
If you want a broader primer on how these pathology labels differ in cancer care, this guide on carcinoma vs adenocarcinoma can help clarify the terminology.
Later in the section, it helps to hear the concepts spoken through. This overview video gives a patient-friendly starting point:
What families usually mix up
Patients often assume risk factors tell the whole story. They don't. A person can develop one of these cancers without fitting a classic profile, and many people with reflux or smoking history will never develop esophageal cancer. Risk factors help explain patterns. They don't assign blame.
The diagnosis tells your team what the tumor is made of. That matters as much as where the tumor is located.
That's why your oncologist keeps returning to pathology, imaging, and overall health status. The cancer's biology is the starting point for everything that follows.
Understanding Adenocarcinoma From GERD to Diagnosis
For many patients in the United States, the diagnosis is adenocarcinoma. This form usually develops near the lower end of the esophagus, close to where the esophagus meets the stomach. That location is not random. It reflects a long-term process in which stomach acid repeatedly irritates the tissue.
A lot of families recognize the first part of that story because it starts with a common condition: GERD, or gastroesophageal reflux disease. People know it as acid reflux or chronic heartburn. Most reflux doesn't turn into cancer. But in some patients, years of acid exposure can change the cells lining the lower esophagus.
The step-by-step biological pathway
The progression described in clinical references is well defined. Adenocarcinoma of the esophagus typically arises in the distal esophagus at the esophagogastric junction, where acid-induced irritation progresses through a sequence of Barrett metaplasia, low-grade dysplasia, high-grade dysplasia, and then adenocarcinoma according to Medscape's esophageal adenocarcinoma overview.
In plain language, that means:
Normal lining changes first
Repeated acid exposure can push the lower esophagus to replace its usual cells with a different cell type.Barrett's esophagus comes next
This is the best-known precancerous condition in this pathway.Dysplasia means the cells are becoming abnormal
Low-grade and high-grade dysplasia are warning stages, not yet the same as invasive cancer.Adenocarcinoma is the final step in that sequence
This happens when abnormal cells gain the features of cancer and grow beyond normal control.
If your pathology mentions the gastroesophageal junction, this overview of gastroesophageal junction adenocarcinoma may help you understand why tumors in that area can raise both esophageal and stomach-related questions.
What this means in real life
A common patient story goes like this: years of heartburn, antacids used off and on, then swallowing becomes harder, or food starts to “stick.” Sometimes the person had known Barrett's esophagus. Sometimes they didn't. Sometimes reflux was obvious. Sometimes it was treated as a nuisance and not revisited until symptoms changed.
That history matters because it helps explain why your doctors ask so many questions about reflux, Barrett's esophagus, prior endoscopies, and medications for acid suppression. They aren't just gathering background. They're tracing the biology of the cancer.
When adenocarcinoma develops, the path often makes more sense once you see that it didn't appear overnight. It usually followed a chain of tissue changes over time.
Why this type changes the treatment discussion
Adenocarcinoma often leads your care team to pay special attention to the lower esophagus and gastroesophageal junction. It can also shape how surgeons, radiation oncologists, and medical oncologists define the treatment field and sequence.
For some patients, the key issue is whether the cancer is still local enough for a curative plan. For others, especially when the disease is advanced, the central question becomes how to match treatment intensity to symptoms, goals, and tolerance. Even then, understanding that the cancer came from a reflux-related pathway helps explain why this diagnosis is different from squamous cell carcinoma.
Exploring Squamous Cell Carcinoma A Different Biology
Squamous cell carcinoma starts from the flat cells that line the inside of the esophagus. That may sound like a small pathology detail, but it changes how doctors think about risk factors, tumor behavior, and the patient's history. It is not merely adenocarcinoma in another location. It is a different disease process.
Some patients find it helpful to hold the contrast in mind visually before diving into treatment terms:

How SCC differs from adenocarcinoma
Unlike adenocarcinoma, squamous cell carcinoma is tied more closely to tobacco use and heavy alcohol consumption. The earlier global review also notes a strong link to lower socioeconomic status in many developing regions, where most cases occur. That pattern helps explain why SCC remains the dominant esophageal cancer type worldwide, even though many U.S. patients now hear more about adenocarcinoma.
This cancer also tends to arise from the squamous lining itself rather than from the gland-like changes seen in reflux-related disease. That difference is why a person with SCC may have a very different background story from someone with adenocarcinoma.
Why the distinction matters clinically
Doctors don't just label SCC for completeness. They use the diagnosis to guide decision-making. The type affects how the tumor is interpreted, how treatment sequencing is discussed, and what evidence exists after surgery.
Families often expect one standard roadmap for every patient with esophageal cancer. In reality, the biology creates forks in the road. A recommendation that fits adenocarcinoma may not fit SCC nearly as well.
Here are a few practical points patients should know:
Risk history matters differently
In SCC, your doctors may focus more on smoking and alcohol exposure than on reflux history.Tumor location can feel different
Many SCC tumors arise away from the classic lower-esophagus reflux zone.Evidence can be less straightforward after surgery
This becomes especially important later, when the team discusses whether added treatment after surgery is supported.
A pathology label can look technical on paper, but in clinic it changes the questions your doctors ask and the choices they consider reasonable.
For patients with SCC, it's worth asking your team not only what the diagnosis is, but also how that diagnosis changes the treatment logic compared with adenocarcinoma. That question often leads to a clearer, more honest conversation.
How Cancer Type Guides Your Diagnostic Workup
Once cancer is suspected, the workup usually moves quickly. But “quickly” doesn't mean randomly. Each test answers a different question, and your cancer type helps your doctors decide what needs emphasis. The goal is to build a complete picture before major treatment starts.
This process can feel exhausting because several appointments may happen in close succession. Knowing what each step is for can make the whole experience less disorienting.
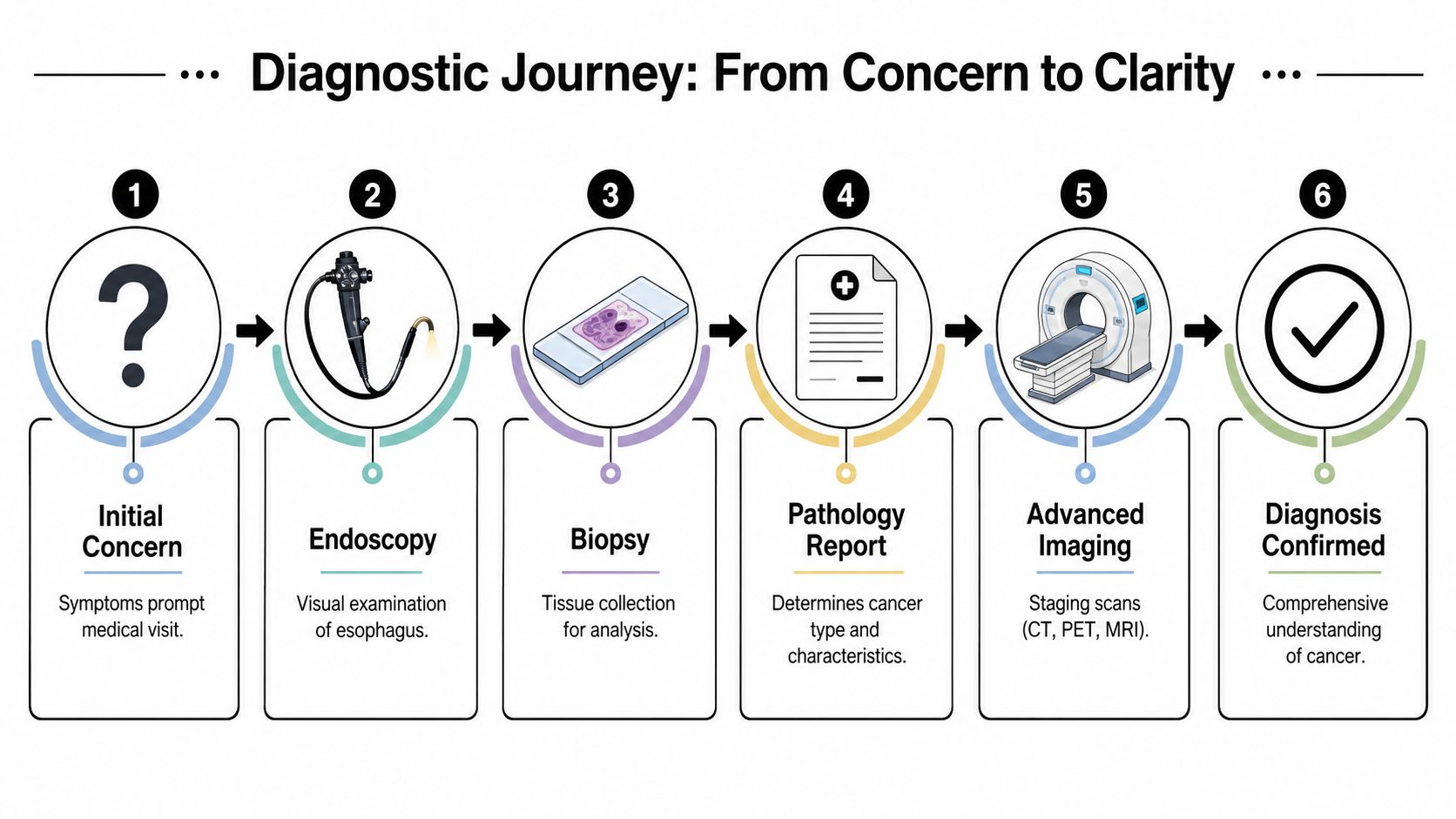
The core steps most patients go through
A typical workup often includes:
Upper endoscopy
A gastroenterologist looks directly at the esophagus and identifies the suspicious area.Biopsy
Tissue samples are taken. The diagnosis then becomes specific, not just “a mass” but a named cancer type.Pathology review
The pathologist determines whether the cancer is adenocarcinoma, squamous cell carcinoma, or a rarer subtype.Imaging
CT, PET, or other scans help show how far the cancer has spread.Fitness assessment
Your team looks at heart, lung, nutrition, and overall functional status to judge what treatment you can safely tolerate.
When surgery may not be the right first path
One of the most stressful moments comes when families ask, “If surgery isn't possible, does that mean nothing can be done?” The answer is often no. There may still be meaningful treatment options, and in some cases, less invasive ones.
According to the patient guidance summarized by Cancer Treatment Centers of America's discussion of esophageal cancer questions, for early-stage tumors classified as T1a, endoscopic mucosal resection (EMR) is often a first-line curative therapy, and NCCN guidelines recommend definitive chemoradiotherapy for medically unfit patients, although general overviews often don't explain these distinctions clearly.
That matters because “not a surgical candidate” doesn't mean the same thing in every case. A person may be medically unfit for a major esophagectomy but still eligible for:
EMR for very early disease
This is an endoscopic approach, not open surgery.Definitive chemoradiotherapy
This may be used when surgery isn't appropriate.Other endoscopic measures
These can sometimes help control disease or symptoms, depending on stage and location.
Questions that deserve a direct answer
Many families leave visits with the phrase “medically unfit” but without a real explanation. If that term is used in your case, ask your team to define it specifically.
Ask, “Is the limitation the tumor, my general health, or both?” That one question often clears up the entire discussion.
You can also ask:
- Is my tumor early enough for an endoscopic option?
- If surgery isn't advised, is the goal still cure or control?
- Which specialist should explain the non-surgical choices in detail?
Those questions can prevent a lot of misunderstanding before treatment begins.
Tailoring Treatment to Your Cancer Type and Stage
Treatment planning becomes more personal once three pieces are in place: the cancer type, the stage, and the patient's overall condition. Doctors may also look at genetic markers and other tumor features when disease is advanced or when standard treatment has stopped working. The result is not one universal recipe. It's a plan built from several moving parts.
That's why two patients with “esophageal cancer” can leave clinic with very different recommendations. One may move toward surgery after pre-treatment. Another may receive chemoradiotherapy as the main treatment. A third may need a strategy centered on symptom relief, swallowing support, and lower-toxicity systemic treatment.

What usually goes into the decision
Most treatment discussions pull from the same major categories:
| Decision factor | Why it matters |
|---|---|
| Cancer type | Adenocarcinoma and SCC often follow different evidence pathways |
| Stage | Local disease and metastatic disease require different goals |
| Performance status | A patient has to be well enough to benefit from treatment |
| Tumor markers and pathology details | These may open or close options in advanced disease |
| Patient goals | Some people prioritize maximal tumor control, others prioritize lower toxicity or swallowing relief |
If you want a broader clinical overview of how teams build these plans, this summary of esophageal cancer treatment guidelines is a useful companion resource.
A real complexity in squamous cell carcinoma
One of the hardest truths in oncology is that evidence isn't equally strong for every situation. For esophageal squamous cell carcinoma, neoadjuvant chemoradiotherapy plus surgery is standard for resectable locoregional disease, but there are no current practical guidelines suggesting postoperative treatment because large randomized trials demonstrating benefit are lacking, as discussed in this review of postoperative treatment in esophageal squamous cell carcinoma.
That gap matters. It means a patient with SCC may reach the postoperative stage and find that the next step is less clearly defined than it would be in some adenocarcinoma settings. This doesn't mean treatment has failed. It means the care team has to individualize the plan more carefully because the evidence is weaker.
Clinical reality: When evidence is thin, experience, multidisciplinary review, and careful patient selection matter even more.
What this means for advanced or resistant disease
If cancer returns, spreads, or doesn't respond the way everyone hoped, the conversation changes again. At that point, doctors may revisit pathology, scan patterns, prior treatments, and molecular markers to look for another opening. The same cancer type that shaped the first-line plan can still matter later when choosing the next step.
Patients in this setting should feel comfortable asking:
- Has the treatment goal changed since diagnosis?
- Should the pathology be reviewed again at a specialty center?
- Are there biomarker results that affect targeted therapy or immunotherapy choices?
- Is a second opinion likely to change management?
Those questions are especially important when the standard path has become uncertain. In treatment-resistant disease, clarity often comes from narrowing the goal. Longer control, less toxicity, better swallowing, fewer hospital visits, or a combination of these. A good plan is not only medically sound. It also fits the patient who has to live through it.
Key Questions to Ask Your Oncology Team
Appointments go better when you bring specific questions. Three are especially useful because they often uncover information that otherwise stays buried in the chart.
Are there rare subtypes besides AC and SCC
Yes. Most patients have adenocarcinoma or squamous cell carcinoma, but rare subtypes do exist. Ask whether your pathology showed any unusual features and whether a second pathology review would help if the findings seem unclear.
What does my cancer type mean for prognosis
Ask for a personalized answer, not a generic internet answer. Prognosis depends on much more than the label alone. Stage, response to treatment, nutrition, treatment tolerance, and whether the goal is cure or disease control all matter. If your doctor gives a broad answer, ask what factors in your case are favorable and what factors are concerning.
How should I report symptoms between visits
Be concrete. Don't say only “I'm worse.” Track swallowing problems, pain, nausea, fatigue, and weight changes in plain daily notes. Families also need support outside the clinic, especially when eating, mobility, or medication routines become difficult. For some households, resources on supportive home care for cancer patients can help organize practical day-to-day assistance.
A final question is often the most valuable: “What would you want your own family member to understand about this diagnosis right now?” It usually brings the conversation back to what matters most.
If you or a loved one is facing a new diagnosis, advanced disease, or treatment-resistant esophageal cancer, Hirschfeld Oncology offers educational guidance and consultation options focused on individualized, lower-toxicity cancer care. Their team in Brooklyn shares practical insights for patients and families who want to understand their options clearly and move forward with a plan grounded in both expertise and compassion.
.png)
.png)




