




.png)


You open the report on your phone, and the words blur together. “Poorly differentiated carcinoma.” “Adenocarcinoma.” “Consistent with epithelial origin.” Those encountering such terminology often don't feel informed. They feel frightened, confused, and suddenly aware that every word might matter.
That reaction is normal.
When families come into clinic with a new diagnosis, one of the first things I do is slow the language down. These terms aren't there to make things harder. They're there to describe what kind of cells the cancer came from, and that detail helps doctors decide what to test next, what treatments make sense, and how to judge prognosis more accurately. In complex or advanced cases, that precision becomes even more important.
A lot of online explanations stop at definitions. Patients need more than definitions. They need to know why the wording on a pathology report can change the next step in care.
Understanding Your Pathology Report
A patient once brought in a pathology report folded into quarters, with several words circled in pen. The main question wasn't unusual: “Which word am I supposed to pay attention to?”
That's often the problem. A pathology report can feel like it's written for specialists rather than for the person living through the diagnosis. Terms like carcinoma and adenocarcinoma sound similar, and that makes many people assume they mean the same thing. They don't. They're related, but not interchangeable.
Your pathology report is trying to answer a few basic questions. What tissue did this cancer start in? What does it look like under the microscope? Are there clues about where it began, especially if the cancer is advanced or found in more than one place? Those answers usually come from the biopsy, the pathologist's review, and how well lab and clinic information connect. That's one reason strong interoperability in pathology systems matters in real patient care. It helps teams pull together biopsy details, pathology findings, and clinical records without losing important context.
If you're still trying to decode the wording itself, this guide on how to read a pathology report can help you recognize the parts that tend to carry the most meaning.
The report is not the whole story. It's the first precise description of the disease.
What patients often misunderstand
Many readers see carcinoma and assume that's the final diagnosis. Often, it isn't. It may be the broad category. Adenocarcinoma is more specific.
A few practical reminders can make the report less overwhelming:
- Broad term first: Carcinoma may describe the larger family the cancer belongs to.
- Subtype matters: Adenocarcinoma tells you the tumor likely arose from gland-forming cells.
- More testing may follow: If the first biopsy is small, doctors may need additional stains or molecular testing before treatment decisions are finalized.
The Big Picture What Is Carcinoma
Carcinoma is the parent category. It refers to cancer that starts in epithelial cells. These are the cells that cover body surfaces and line many organs and internal passageways. If you want a simple mental picture, think of epithelial tissue as the body's protective lining and surface covering.
At the histology level, carcinoma arises from epithelial cells, while adenocarcinoma is a subtype that starts in glandular epithelium, as explained by Cancer Treatment Centers of America's overview of adenocarcinoma. That hierarchy is the key idea many patients miss.
Why “carcinoma” is only the starting point
When a report says carcinoma, it tells your doctors the cancer began in a major tissue category. That's useful, but it doesn't yet tell them the full subtype.
Carcinoma includes several branches. Some arise from flat lining cells. Others arise from basal-type cells in certain tissues. Adenocarcinoma belongs under this same umbrella, but it points to a different kind of epithelial cell and often a different pattern under the microscope.
Here's the simplest explanation:
| Term | What it means |
|---|---|
| Carcinoma | A broad category of cancer arising from epithelial tissue |
| Adenocarcinoma | A subtype of carcinoma arising from glandular epithelial cells |
Why doctors care about the category
The broad label helps pathologists organize what they are seeing. But treatment decisions usually need more than the parent category.
For example, two cancers can both be carcinomas and still behave very differently because they come from different epithelial lineages. That difference affects the testing path, the likely site of origin, and sometimes the kinds of drugs that are more relevant later.
Practical rule: If your report says carcinoma, ask whether the subtype has already been confirmed or is still being worked out.
That question is especially important in advanced disease, when the cancer may have spread and the original starting point is not obvious from imaging alone.
A Deeper Look What Is Adenocarcinoma
Adenocarcinoma is a type of carcinoma that starts in gland cells, which are specialized epithelial cells that make and release substances such as mucus, digestive fluids, or hormones. Because glandular tissue exists in many organs, adenocarcinoma can show up in many different parts of the body.
This is why the word appears so often in oncology. It's not rare terminology. It's a very common and very important subtype label.
According to Mayo Clinic's adenocarcinoma overview, adenocarcinoma is not a separate cancer family but one of the major carcinoma categories. The same source notes that most breast, colon, lung, and prostate cancers are adenocarcinomas, and that it accounts for more than 90% of pancreatic cancer cases. It also notes that more than 90% of stomach cancers are adenocarcinomas.
What pathologists are looking for
Under the microscope, adenocarcinoma often shows signs that the cancer is trying to form glands or produce secretions. Sometimes that pattern is obvious. Sometimes it's subtle, especially if the tumor is poorly differentiated and has lost some of the features of the original tissue.
That's where specialist pathology becomes so important. A tiny biopsy sample may not give a complete picture on first review, and doctors may need added testing to confirm whether a tumor is adenocarcinoma and where it most likely began.
Why patients hear this term so often
Adenocarcinoma comes up repeatedly because glandular tissues are common in organs where cancer is common. That includes the:
- Colon and rectum
- Pancreas
- Stomach
- Lung
- Breast
- Prostate
So if your doctor says you have adenocarcinoma, that doesn't mean you have an unusual or mysterious diagnosis. It means the pathology team has already narrowed the cancer to a more specific subtype within the larger carcinoma family.
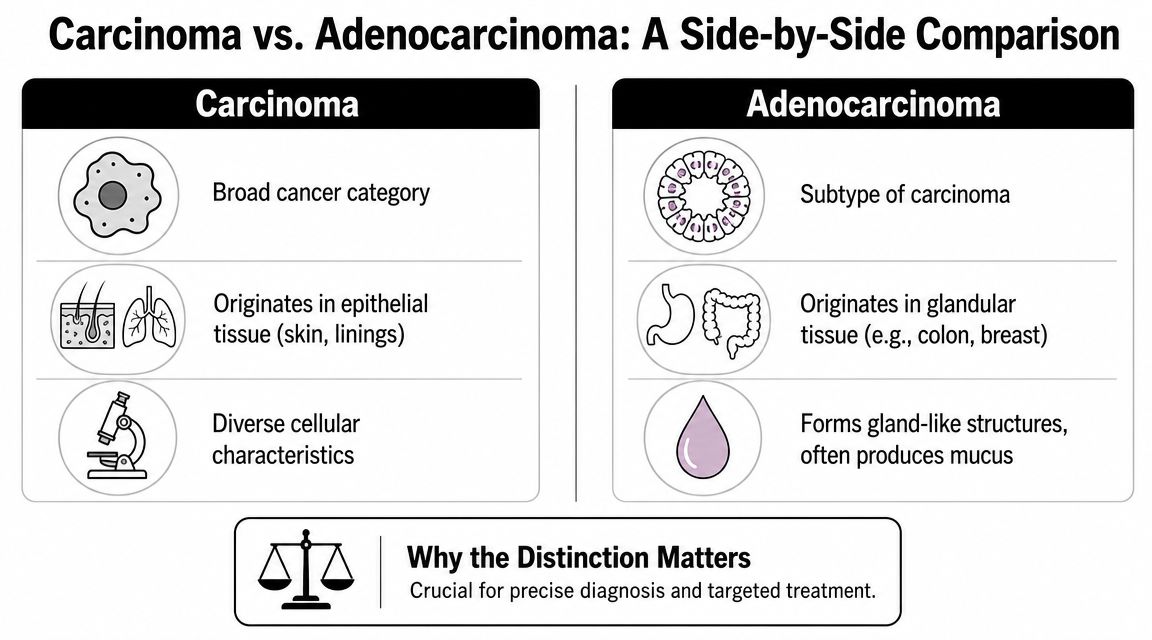
Carcinoma vs Adenocarcinoma A Side by Side Comparison
The fastest way to clear up the confusion is to compare the terms directly.
A simple comparison table
| Feature | Carcinoma | Adenocarcinoma |
|---|---|---|
| Category | Broad cancer category | Specific subtype within carcinoma |
| Cell of origin | Epithelial cells | Glandular epithelial cells |
| Microscopic clue | Can include several epithelial patterns | Often shows gland formation or secretory features |
| Typical wording on report | May be an early or broad label | More specific diagnostic classification |
| Clinical use | Helps define the tissue family | More useful for organ-specific planning and further testing |
The single most important relationship is this: all adenocarcinomas are carcinomas, but not all carcinomas are adenocarcinomas.
A lung cancer example
This distinction isn't academic. In lung cancer, histology shapes how doctors think about the disease. The CDC's report on U.S. lung cancer cell types states that in 2022, adenocarcinoma accounted for 45% of all lung cancer cases, compared with 21% for squamous cell carcinoma and 12% for small cell carcinoma. The same report notes that adenocarcinoma was the most common lung cancer type in both males and females and across every age group.
That means when a pathologist identifies lung adenocarcinoma, they are naming the dominant histologic pattern in a very common cancer setting. That label has practical consequences for testing and management.
Where readers usually get tripped up
People often compare the words as if they were two competing diagnoses. They aren't. One term is broad, and the other is a subset within it.
A good way to test your understanding is to swap in everyday categories:
- Fruit is the broad category.
- Apple is the subtype.
You wouldn't ask whether an apple is different from fruit in the same way you would compare an apple to an orange. The same logic applies here.
When doctors refine “carcinoma” to “adenocarcinoma,” they're not changing the family. They're identifying the subtype more precisely.
How Doctors Pinpoint Your Diagnosis
Most patients know they had a biopsy. Fewer know what happens after the sample reaches the lab, or why the final diagnosis sometimes takes longer than expected.
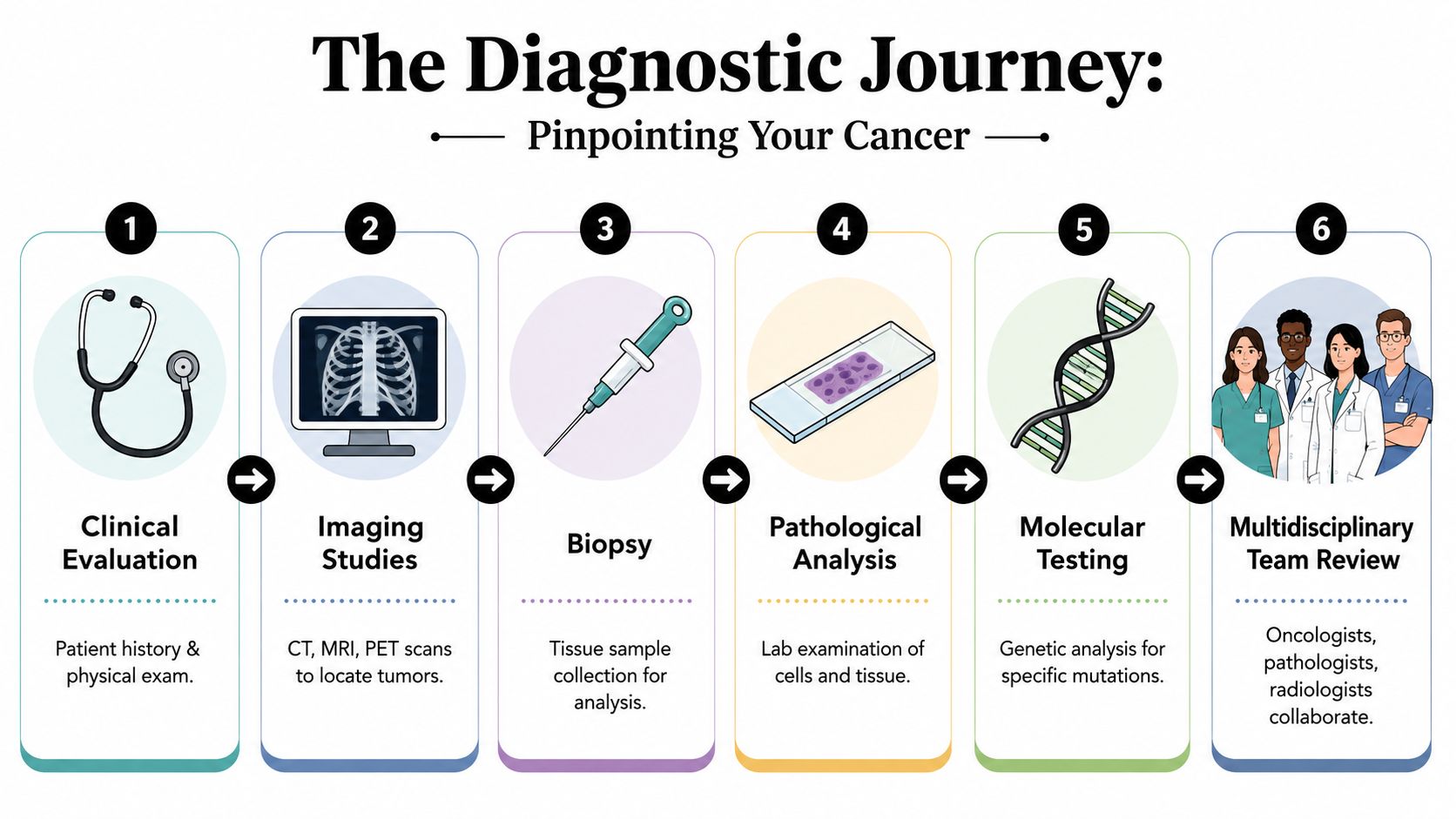
The biopsy starts the process
A biopsy gives the team actual tumor tissue to study. Imaging can show where a mass is and how large it may be, but imaging alone usually can't tell doctors whether a cancer is carcinoma, adenocarcinoma, or another type.
The pathologist then examines the sample under a microscope. This is histology. They look at how the cells are arranged, whether they resemble gland-forming tissue, and how abnormal they appear.
Immunohistochemistry adds another layer
If the answer isn't obvious on routine microscopy, pathologists often use immunohistochemistry, usually shortened to IHC. In simple terms, IHC uses stains that bind to proteins on or in tumor cells. Those staining patterns can support whether the tumor is glandular and may also offer clues about the organ of origin.
This matters most when the biopsy is tiny, the tumor is poorly differentiated, or the cancer has already spread. In those situations, the pathology team is often answering two questions at once: what subtype is this, and where did it begin?
For readers who want a patient-friendly overview of this next layer of testing, this explanation of molecular testing for cancer is a useful companion.
Precision often requires several steps
Diagnosis usually unfolds in stages rather than all at once. A report may begin broadly and become more specific as more information comes in.
That sequence often looks like this:
- Initial biopsy result: Cancer is present.
- Microscopic classification: The tumor looks epithelial, suggesting carcinoma.
- Special stains: The pattern supports adenocarcinoma.
- Molecular workup: Additional findings may help identify actionable features or strengthen the suspected site of origin.
- Team review: Pathology, radiology, and oncology findings are compared to make sure they fit together.
Why this process matters in advanced disease
In straightforward early-stage cases, diagnosis can be relatively clear. In advanced or unusual cases, details become harder and more important at the same time.
A small liver biopsy, for example, may show metastatic adenocarcinoma. That tells doctors the liver lesion likely spread from somewhere else. The next step isn't just naming it. It's working out whether the source is more likely gastrointestinal, pancreatic, lung, breast, or another gland-forming organ. That answer can change treatment direction substantially.
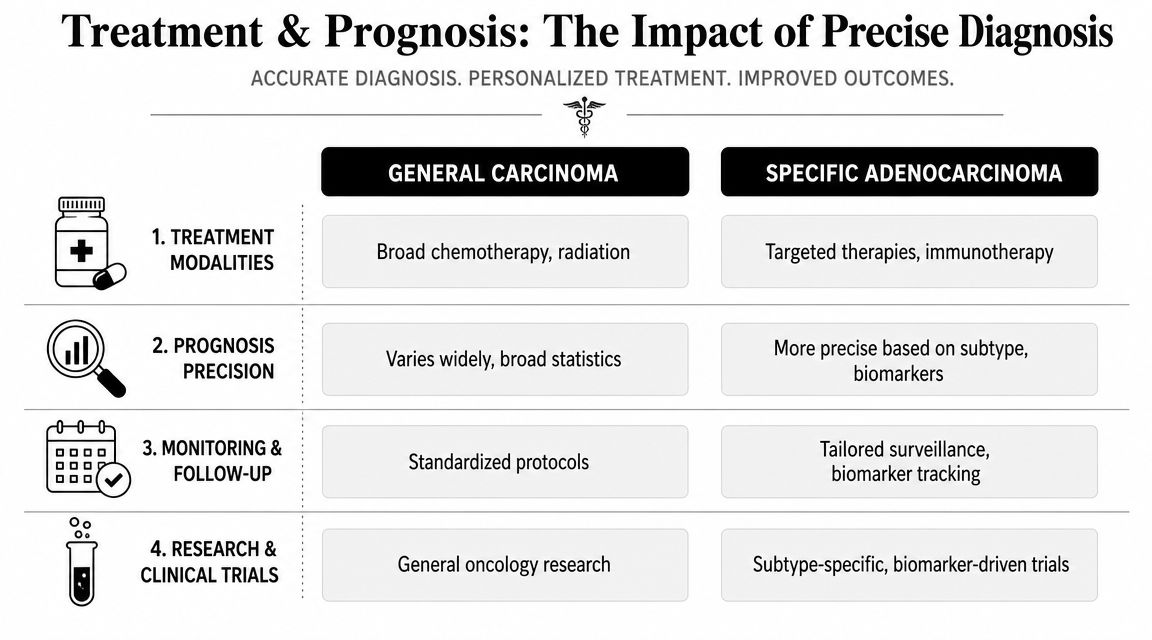
Why This Distinction Shapes Your Treatment and Prognosis
The reason patients search for carcinoma vs adenocarcinoma is usually not pure curiosity. They want to know whether the wording changes what happens next. In many cases, it does.
Prognosis depends more on site than on the word alone
One of the biggest misconceptions is that adenocarcinoma has a single prognosis. It doesn't. The outlook depends heavily on where the adenocarcinoma started, along with stage, spread pattern, overall health, and tumor biology.
The clearest example comes from Cleveland Clinic's adenocarcinoma survival overview, which reports U.S.-based 5-year relative survival estimates of 99% for prostate adenocarcinoma, 90% for breast and colorectal, 56% for lung, 47% for esophageal, 32% for gastric, and 10% for pancreatic adenocarcinoma. That wide range shows why the primary site matters far more than the broad label alone.
If your report says adenocarcinoma, the next key question is not “Is this good or bad?” The better question is: Where did it start, what stage is it, and what molecular features does it have?
Histology can influence treatment choices
Once doctors know a cancer is adenocarcinoma, they often pursue more specialized testing. In many advanced cancers, treatment planning depends not just on histology but also on whether the tumor carries a feature that may respond to targeted therapy or immunotherapy.
That's why precision oncology has become so important in modern cancer care. If you'd like a broader explanation of that approach, this guide to precision oncology offers a patient-focused overview.
What to ask your oncologist
A more specific diagnosis gives you better questions to ask. These are often the most useful:
- Has the primary site been confirmed? If not, what are the leading possibilities?
- Was the diagnosis based only on routine pathology, or were special stains used?
- Do I need molecular testing? This can matter greatly in advanced disease.
- Does my subtype affect which drugs are more appropriate?
- Is prognosis being estimated based on my exact cancer type and stage, or only on a broad category?
A precise pathology label doesn't guarantee an easy treatment path. It does give your team a more reliable map.
Why this matters most in complex cases
In early disease, surgery may settle many decisions quickly. In metastatic or treatment-resistant disease, every layer of specificity becomes more valuable. A broad label may be enough to start the conversation. It usually isn't enough to finish it.
That is especially true when doctors are weighing standard chemotherapy, targeted options, immunotherapy, clinical trial eligibility, and how to balance treatment benefit against side effects and quality of life.
Your Next Steps Consulting an Oncology Specialist
Once you know the diagnosis is more specific than “carcinoma,” the next step is to make sure the treatment plan is equally specific. That doesn't mean rushing into more fear. It means slowing down enough to ask whether the pathology, imaging, staging, and molecular workup all tell the same story.
When a specialist review helps most
A specialist consultation is especially useful when:
- The cancer is advanced: Treatment planning often depends on subtype and molecular findings.
- The biopsy is limited or ambiguous: A second pathology review may clarify the diagnosis.
- The primary site is uncertain: This is common in metastatic presentations.
- Standard treatment has stopped working: A fresh review may uncover additional options.
You should expect a good oncology visit to include a careful review of the pathology report, prior scans, the stage of disease, your current symptoms, and the goals that matter most to you. For some people, the priority is aggressive disease control. For others, it's balancing disease control with lower toxicity and daily function. Both are legitimate priorities.
Questions worth bringing to the appointment
Bring your report and ask plainly:
- Do you agree with the pathology diagnosis as written?
- Is there enough tissue for further testing?
- Are there treatment options tied to this exact subtype?
- What are the realistic goals of treatment in my case?
Those questions can turn a vague diagnosis into a workable plan.
Frequently Asked Questions
Is adenocarcinoma worse than carcinoma
Not by definition. Adenocarcinoma is a subtype of carcinoma, not a universally more severe form. What matters most is the organ of origin, the stage, and the tumor's biology. A lung adenocarcinoma, pancreatic adenocarcinoma, and prostate adenocarcinoma do not carry the same outlook or treatment path.
Can a carcinoma turn into an adenocarcinoma
In routine diagnosis, doctors don't think of this as one becoming the other. Carcinoma is the broad family, and adenocarcinoma is a subtype within that family from the start. Usually, the question is whether the pathology team has narrowed the diagnosis enough yet.
What if my report says adenocarcinoma but the primary site is unknown
That can happen, especially in metastatic disease or when the biopsy sample is small. In cancers of unknown primary, adenocarcinoma is one of the core diagnostic categories, and Memorial Sloan Kettering Cancer Center explains that modern classification uses immunohistochemistry and next-generation sequencing to identify actionable alterations even when the original site is uncertain. In practice, that means doctors may still be able to guide treatment even before every question about origin is fully resolved.
Does the pathology wording affect treatment right away
Often, yes. A more specific subtype can change which additional tests are ordered, how the likely site of origin is judged, and whether targeted or biomarker-driven options should be explored.
If you or a loved one is trying to make sense of a pathology report that mentions carcinoma or adenocarcinoma, a specialist review can bring needed clarity. Hirschfeld Oncology provides patient-centered care for complex and advanced cancers, with careful attention to pathology, molecular testing, treatment tolerability, and individualized planning. For patients and families in Brooklyn and across New York City, it's a place to ask hard questions, explore thoughtful options, and move forward with a team that understands how much precision matters.
.png)
.png)




