




.png)


The phone call ends. You have a scan result, a pathology report, and a handful of new words that sound technical and urgent. Your family wants answers right away. You want one clear sentence that tells you what happens next.
Patients don't typically get that sentence on day one.
Instead, they hear about stages, chemotherapy combinations, surgery, mutation testing, radiation, ports, pumps, side effects, and follow-up plans. That can make pancreatic cancer treatment guidelines feel cold or impersonal. In practice, they're meant to do the opposite. They give your doctors a structured starting point so your care doesn't depend on guesswork.
Navigating Your Pancreatic Cancer Diagnosis
A pancreatic cancer diagnosis often lands in the middle of ordinary life. One week you're chasing down the cause of weight loss, abdominal pain, jaundice, or fatigue. The next, you're trying to understand a disease known for being aggressive and hard to catch early.
The numbers explain why the first conversations feel so serious. Pancreatic cancer has the highest mortality rate among all major cancers, with a 5-year relative survival rate of only 13% for all stages combined. The same source projects that 67,530 Americans will be diagnosed in 2026, and notes that nearly 80% of patients have advanced, inoperable disease by the time symptoms appear according to PanCAN's pancreatic cancer facts.
That's frightening information. It's also why guidelines matter so much.
What guidelines actually do
Guidelines are not a rigid script. They're a map built from clinical evidence and expert review. They help answer practical questions:
- Which tests come first: imaging, biopsy, staging, and molecular testing
- Who should get intensive chemotherapy: usually based on performance status, organ function, and overall health
- When local treatment helps: surgery or radiation for selected situations
- What to do next if treatment changes: second-line therapy, symptom support, and targeted options
Practical rule: When you hear “guidelines,” think “starting framework,” not “one-size-fits-all order.”
What families usually need most
Patients and caregivers often want the same three things right away:
- A plain-language explanation of the stage and what it means.
- A treatment plan with a reason behind it.
- A sense of what comes after the first step.
That's how experienced oncology teams use pancreatic cancer treatment guidelines. They translate them into choices that fit the person in front of them, not just the disease on paper.
Understanding Pancreatic Cancer Staging and Diagnosis
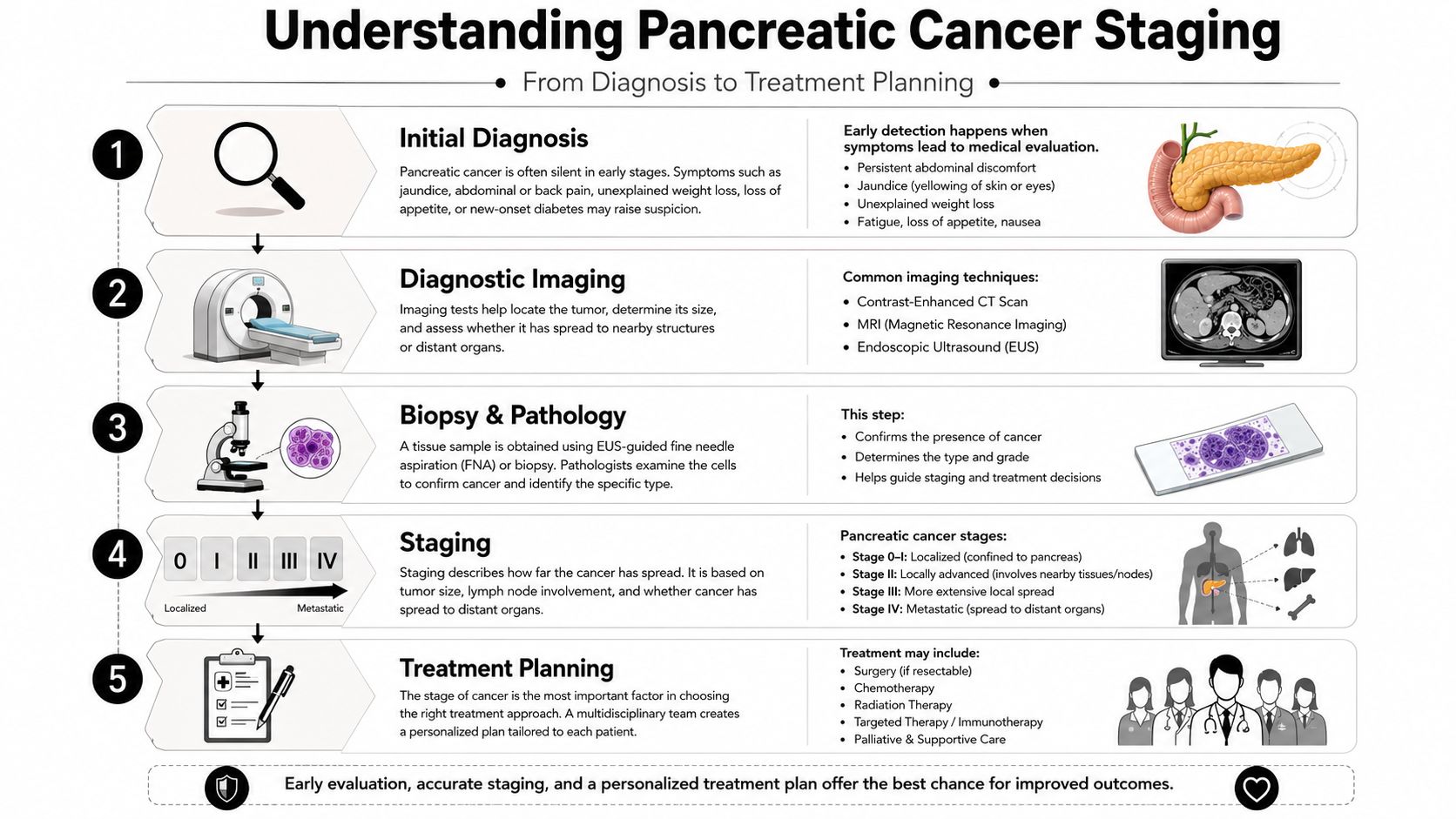
Before any treatment starts, your team has to answer two questions. Where is the cancer, and how far has it spread? That's what staging does.
A simple way to think about it is travel distance. A tumor confined to the pancreas is a local problem. A tumor involving nearby major structures is a regional problem. Cancer that has spread to distant organs is a body-wide problem. The label changes the treatment path.
The key stages in plain language
Doctors often describe pancreatic cancer in categories that matter more for treatment than for memorizing stage numbers.
- Resectable: the tumor appears removable with surgery.
- Borderline resectable: surgery may be possible, but the tumor is close to important blood vessels.
- Locally advanced: the cancer hasn't spread to distant organs, but it involves nearby structures enough that surgery usually isn't the first move.
- Metastatic: the cancer has spread to distant sites, so treatment usually focuses on whole-body therapy rather than an operation.
That distinction matters because a pancreatic surgeon, a medical oncologist, and a radiation oncologist each play a different role depending on stage.
The tests that build the plan
No single test answers everything. Your doctors combine several pieces of information.
Imaging
A CT scan usually gives the first detailed look at the pancreas and nearby blood vessels. An MRI can help clarify liver findings or bile duct issues. An endoscopic ultrasound, often called EUS, can help doctors look closely at the tumor and guide biopsy.
Biopsy and pathology
A biopsy confirms that the mass is cancer and identifies the tumor type. This is important because treatment should be based on tissue confirmation whenever possible, especially before starting systemic therapy.
Performance status and baseline health
Staging tells doctors where the cancer is. It does not tell them how strong your body is for treatment. That's why they also assess performance status, nutrition, weight change, pain, liver function, kidney function, and other medical conditions.
A scan can show the cancer. It can't show how much treatment your body can reasonably tolerate. That judgment comes from the full clinical picture.
Why this early phase can feel slow
Families sometimes worry that too much time is being spent on testing. In reality, a rushed plan can lead to the wrong starting treatment. The best first regimen depends on whether the disease is resectable, locally advanced, or metastatic, and whether the patient is healthy, frail, or somewhere in between.
That last group is where many people feel overlooked. They're not well enough for the most aggressive approach, but they still want treatment that has a real chance of helping. That gap becomes especially important when chemotherapy decisions begin.
First-Line Chemotherapy The Guideline Cornerstones
A common clinic moment goes like this. A patient hears that chemotherapy should start soon, then hears two very different messages in the same visit. One regimen may control the cancer more strongly, but it can also hit the body much harder. Another may be easier to tolerate, but families worry it may not be enough. For older adults and people with borderline strength, that tension often defines the whole decision.
That is why first-line treatment is not merely a ranking of drugs from strongest to weakest. It is a matching process. The goal is to choose a regimen that has a realistic chance of helping and that the patient can adhere to.
Why guideline regimens matter, and where they can fall short
Standard recommendations usually center on a few well-known starting options. For fit patients with metastatic pancreatic cancer, doctors often consider FOLFIRINOX. For patients who are frailer or who have more medical issues, gemcitabine-based treatment is commonly used.
Those categories are useful, but real patients do not always fit neatly into them. Many people are not strong enough for the most intensive plan, yet they are also not so frail that single-agent treatment feels like the only reasonable choice. This is the gap many families notice right away, especially in adults who are older, have weight loss, or have an ECOG performance status that sits in the gray zone.
What FOLFIRINOX means in practical terms
FOLFIRINOX combines four drugs. It is often chosen for patients with strong baseline function because it can be more active against the cancer than gentler regimens. The tradeoff is a heavier side-effect burden, including fatigue, diarrhea, neuropathy, and blood count suppression that can raise infection risk.
A helpful way to think about it is this. FOLFIRINOX is built for a body with reserve. If someone is already spending much of the day resting, losing weight quickly, or struggling with other illnesses, the treatment itself can become part of the problem.
That does not mean it should be ruled out automatically. Some patients receive modified versions with dose adjustments, schedule changes, or closer supportive care. Guidelines provide the framework. Experienced clinicians still have to judge how much treatment a specific person can absorb safely.
The gentler end of the spectrum
For patients who are more fragile, gemcitabine alone may be the safer starting point. It is generally easier to tolerate than FOLFIRINOX, though it still requires monitoring and can still cause low blood counts, fatigue, and other side effects.
The concern many families raise is understandable. If FOLFIRINOX feels too harsh and gemcitabine alone feels too limited, is there a middle path?
Often, yes.
Where gemcitabine plus nab-paclitaxel fits
One commonly used middle-ground option is gemcitabine plus nab-paclitaxel. This combination is often considered for patients who need active treatment but may not be ideal candidates for full-intensity FOLFIRINOX. In practice, this is one of the most important ways doctors tailor first-line therapy for older adults and patients with marginal performance status.
If you want a plain-language overview before discussing it with your oncologist, this guide to gemcitabine and Abraxane in pancreatic cancer care explains how the regimen is used and what side effects to expect.
This is also where personalization begins to matter more than the guideline table alone suggests. Some patients start with this doublet at full dose. Others do better with reduced starting doses, longer intervals between treatments, or early supportive measures for nausea, diarrhea, neuropathy, and appetite loss. Those adjustments are not a sign that treatment is failing. They are often what make treatment possible.
First-Line Chemotherapy Regimens at a Glance
| Regimen | Typical fit | Main advantage | Main concern |
|---|---|---|---|
| FOLFIRINOX | Patients with strong performance status and enough organ function to tolerate intensive therapy | Higher anticancer activity in appropriately selected patients | More toxicity, including blood count suppression, neuropathy, and gastrointestinal side effects |
| Gemcitabine plus nab-paclitaxel | Patients who need meaningful disease control but may not be ideal for FOLFIRINOX | Active regimen with a balance of effectiveness and tolerability for many patients | Fatigue, neuropathy, myelosuppression, and the need for dose adjustment in some patients |
| Gemcitabine monotherapy | Frail patients, many with ECOG 2 or substantial comorbidity | Simpler and often easier to tolerate | May offer less tumor control than combination treatment |
The best first regimen is the one that matches both the cancer and the patient in front of you.
Questions worth asking before treatment starts
Families often feel pressure to choose quickly. A better approach is to ask targeted questions that clarify fit.
Ask whether the recommendation is based on tumor biology, performance status, age, nutrition, liver function, symptom burden, or all of the above. Ask what side effects are most likely to interfere with daily life. Ask whether the team expects to start at full dose or with modifications. Ask what signs would trigger a change in plan.
Those questions matter most for the group that standard guidelines describe only broadly. Older adults. Patients with borderline stamina. Patients who want treatment with real intent, but not at the cost of spending every day recovering from the last infusion.
A note on coordination
Chemotherapy decisions often overlap with discussions about future radiation, symptom control, and logistics across multiple clinics. If your care plan later includes radiation, families sometimes find it helpful to review OMOPHub's CPT code guidance so the scheduling and billing language is less confusing.
The larger point is simple. Guidelines are the starting map. Personalized first-line treatment is what helps many patients, especially those in the middle ground, turn that map into a plan they can live with.
When Surgery and Radiation Are Part of the Plan
Many people assume cancer treatment starts with surgery. In pancreatic cancer, that's only true for a smaller group of patients.
The reason is straightforward. Surgery treats disease in one place. If cancer has already spread, removing the primary tumor doesn't address the full problem. That's why local treatment is usually reserved for resectable and some borderline resectable cancers, and sometimes reconsidered after initial therapy for selected locally advanced cases.
When surgery has a role
Surgery is usually discussed when imaging suggests the tumor can be removed safely, or might become removable after treatment. In that setting, doctors may talk about treatment with curative intent, meaning the goal is long-term disease control rather than symptom management alone.
For many patients, chemotherapy comes first. That approach can help test how the cancer behaves and, in some cases, improve the chances of getting to surgery.
Where radiation fits
Radiation may be used to help control local disease, especially when the tumor is causing pain or sits close to structures that make surgery difficult. Sometimes it's paired with chemotherapy. Sometimes it's used later to manage symptoms.
Families often get confused by the logistics of radiation because the treatment plan includes not only medical decisions but also planning visits, simulation, and coding details that affect coordination across clinics. If you're trying to understand the administrative side, OMOPHub's CPT code guidance for radiation oncology gives a useful overview of how these services are categorized.
Questions worth asking the team
- Is the tumor resectable now, or only potentially resectable later?
- Are you recommending chemotherapy before surgery? If so, why?
- Would radiation be used to improve local control, symptom relief, or surgical planning?
If surgery isn't being offered, that doesn't mean nothing can be done. It means your team is choosing the treatment that matches where the disease is behaving.
Unlocking Personalized Treatments with Biomarkers
A common moment of confusion happens after the first treatment plan is explained. A family hears about chemotherapy, then suddenly the oncologist starts talking about gene changes, tumor testing, and drugs that only help a small group of patients. It can sound like a separate conversation. It is part of the same treatment decision.
Biomarker testing adds another layer to the plan. Staging tells your team where the cancer is behaving. Biomarker results help show how the tumor is built and whether it has features that open the door to a more individualized treatment, sometimes with a different side effect profile than standard chemotherapy. That matters especially for older adults and people with borderline performance status, where the usual guideline regimens may be hard to tolerate at full intensity.
Which biomarker tests matter
A biomarker is a measurable tumor feature that can guide treatment choice. In pancreatic cancer, the main guideline-supported tests look for changes such as BRCA1/2 mutations, NTRK gene fusions, and MSI-H or dMMR status. The NCCN patient guidelines for pancreatic cancer describe molecular testing as part of treatment planning for patients who may be candidates for targeted therapy or immunotherapy.
That point is easy to miss. These tests are not extra paperwork added at the end. They help answer a practical question early. Is there a treatment option that matches this tumor more precisely than standard chemotherapy alone?

How results change treatment choices
Some biomarker results can lead to a targeted drug or immunotherapy.
For patients with a germline BRCA mutation whose cancer has remained controlled on first-line platinum chemotherapy, maintenance olaparib became an option based on the POLO trial published in The New England Journal of Medicine. For NTRK fusion-positive tumors, drugs such as larotrectinib or entrectinib may be considered. For tumors that are MSI-H or dMMR, pembrolizumab may be an option because these cancers can be more responsive to immunotherapy.
The gap in standard guidelines creates a very real challenge for patients. Guideline cornerstone regimens are still the starting point for many people. But if a patient is 78, frail after weight loss, or functioning at the edge of what full-dose combination chemotherapy would allow, biomarker-driven treatment can sometimes provide a better-matched path. It does not replace standard care for everyone. It helps identify the subset of patients for whom a more individualized regimen may offer meaningful benefit with less collateral toxicity.
How to understand biomarkers without the jargon
Biomarkers work like fingerprints left by the tumor. A CT scan shows the outline of the problem. Biomarker testing shows some of the tumor's internal wiring.
Chemotherapy treats broadly, which is often necessary in pancreatic cancer. Targeted therapy is narrower. It only works when the cancer carries the matching feature. That is why two patients with the same stage of disease can receive different recommendations.
Not every tumor will have an actionable finding. Still, asking whether testing has been done is reasonable, especially if the standard regimen feels too intense, if side effects are building, or if your team is trying to balance effectiveness with day-to-day function. If you want a clearer picture of what broader tumor testing includes, this explanation of genomic profiling to guide pancreatic cancer therapy can help frame that discussion. For a plain-language refresher on biomarker basics, Goodlabs for biomarker tracking is also a useful reference.
In pancreatic cancer, the scans tell part of the story. The biomarker results may explain which treatments fit the tumor, and which ones may fit the patient better.
Next Steps When Your First Treatment Changes
One of the hardest moments in care is hearing that the first regimen is no longer the right one. Sometimes the cancer grows. Sometimes side effects accumulate. Sometimes a treatment helps for a while but stops helping enough.
That change does not mean the roadmap is over.
What second-line treatment means
Second-line therapy is the next systemic treatment used after the initial regimen. The choice depends on several practical questions:
- What was used first
- How much toxicity is still present
- Whether the liver, kidneys, and bone marrow can support more therapy
- Whether the patient still has the performance status to benefit
In such cases, oncology becomes very individualized. The best next step after one regimen is not automatically the best next step after another.
A guideline-supported second-line option
For patients with metastatic pancreatic cancer who started with gemcitabine plus nab-paclitaxel and still maintain ECOG 0 to 1, the preferred second-line cytotoxic regimen is fluorouracil plus nanoliposomal irinotecan, with fluorouracil plus regular irinotecan as an acceptable alternative when nanoliposomal irinotecan is not accessible, according to the ASCO guideline update on metastatic pancreatic cancer.
The same guidance states that second-line cytotoxic therapy can improve overall survival when doctors choose the regimen carefully and account for residual toxicities, organ function, and comorbidities.
What else should happen at this decision point
This is also the time to ask about:
- Symptom management if pain, appetite loss, or fatigue have changed
- Molecular results if biomarker testing wasn't completed earlier
- Clinical trials that may fit the current stage of treatment
If you're exploring research options alongside standard care, this page on clinical trial opportunities for pancreatic cancer patients can help you prepare better questions for your oncology team.
Second-line treatment is not just “more chemo.” It's a reassessment of goals, tolerance, and available tools.
Beyond the Guidelines Personalizing Your Treatment Path
A common and painful moment in pancreatic cancer care happens after the first treatment discussion. An older adult sits in clinic with a spouse or adult child. The standard regimens have been explained. One sounds too harsh for their current strength. Another sounds gentler, but may also sound too limited. Families often ask the same question: is there anything in between?
For many patients, that is the actual gap in standard guidelines.
The National Cancer Institute's pancreatic cancer treatment resource notes that recommendations often sort patients into broad groups, such as those who can tolerate intensive combination treatment and those better suited for less intensive single-drug therapy, with less direction for people in the middle, as described in the NCI pancreatic treatment PDQ.

That middle group includes patients who are older, losing weight, recovering from jaundice, or living with fatigue, neuropathy, diabetes, or other medical problems that narrow their margin for side effects. They may still want active treatment. They may still benefit from it. They just may not benefit from treatment delivered at full intensity.
Personalization often helps bridge that gap.
A personalized plan does not mean abandoning guidelines or inventing therapy from scratch. It works more like tailoring a suit. The fabric is still the same evidence-based treatment. The fit changes so the person can wear it. In practice, that may mean adjusting dose, changing the schedule, choosing a better starting regimen for a frailer patient, building in more nutritional support, or monitoring more closely so side effects are addressed before they spiral into a hospitalization.
Sometimes the best plan is a modified combination regimen rather than the strongest standard schedule. Sometimes it is a single agent used thoughtfully, with room to add or change treatment if strength improves. Sometimes biomarker findings create another option entirely. The goal is simple: preserve enough function and comfort that treatment remains both tolerable and worthwhile.
Quality of life is integral to cancer treatment success, not merely a side issue.
Patients often worry that asking for a lower-toxicity approach means they are settling. Families worry that reducing intensity means losing time. In reality, a regimen that causes severe exhaustion, infections, repeated delays, or emergency visits can stop helping very quickly. A better-matched plan may allow treatment to continue longer, control symptoms more steadily, and protect independence at home.
Nutrition is part of that same conversation. Pancreatic cancer and its treatment often make eating harder through nausea, pain, early fullness, taste changes, and poor digestion. Families frequently need practical structure, not vague advice. Resources such as personalized cancer meal plans can help organize meals around appetite, symptoms, and treatment days.
A short discussion of this balance between active treatment and tolerability can be helpful for families who are weighing options:
The better question is often not “What is the strongest treatment?” It is “What treatment gives this person the best chance to benefit without losing too much of daily life?”
At a practice level, centers that offer individualized regimens, molecular profiling, infusion support, and symptom management can be useful for these more complicated decisions. Hirschfeld Oncology is one example of a Brooklyn oncology practice that provides customized treatment planning for complex and advanced-stage cancers, including lower-toxicity strategies when standard pathways do not fit.
If you or a loved one is sorting through pancreatic cancer treatment options after hearing that standard regimens may be too toxic or no longer enough, Hirschfeld Oncology offers educational resources and consultation information that can help you prepare for a more informed discussion about personalized treatment paths.
.png)
.png)




