




.png)


When someone hears “stage 4 pancreatic cancer,” the next few minutes often blur. A scan has just changed the future. Family members start searching on their phones. Someone asks about chemotherapy, and suddenly a pair of drug names, gemcitabine and Abraxane, enters the conversation.
That combination matters because it’s one of the most established first-line treatments for metastatic pancreatic cancer. It isn’t experimental guesswork. It became a standard option after a large phase III trial showed better survival, better disease control, and higher tumor response rates than gemcitabine alone, as detailed by the National Cancer Institute summary of the MPACT trial.
In practice, though, the primary question usually isn’t only “Does it work?” It’s “Can I tolerate it well enough to stay on it?” That’s where treatment decisions become personal. The regimen on paper is only the start. What often determines whether gemcitabine and Abraxane help is how carefully the team adjusts schedule, supportive care, and monitoring to fit the patient sitting in front of them.
Navigating Your Treatment Options After Diagnosis
A common scene in clinic goes like this. A patient has abdominal pain, weight loss, or jaundice, then a CT scan shows pancreatic cancer that has already spread. The first appointment after that diagnosis is heavy. Patients want a plan quickly, but they also want to understand whether treatment will help, what daily life will look like, and whether they’ll spend their time in a chair feeling sick.
For many people with metastatic pancreatic ductal adenocarcinoma, gemcitabine and Abraxane is one of the first regimens discussed because it has been used widely in both academic and community settings. In a US retrospective study of 7603 patients with pancreatic ductal adenocarcinoma, 42.8% received the gemcitabine and Abraxane combination, underscoring how often clinicians turn to it in real-world care, according to Abraxane Pro data on metastatic pancreatic cancer.
That kind of widespread use matters for patients. It means this isn’t a niche approach used only in select centers. It’s a regimen that many oncology teams know well, including how to start it, when to hold it, and how to adjust it when fatigue, neuropathy, or blood count problems show up.
What patients are really deciding
Most patients aren’t choosing between “treatment” and “no treatment” in an abstract sense. They’re deciding among practical trade-offs:
- Cancer control: Will this regimen give a real chance of shrinking or stabilizing disease?
- Tolerability: Can the body handle repeated cycles without side effects becoming overwhelming?
- Logistics: How often will infusions happen, and how disruptive will they be?
- Goals of care: Is the focus on maximum intensity, a gentler outpatient approach, or a balance between the two?
Practical rule: The best regimen is the one that treats the cancer effectively and remains sustainable enough for the patient to continue.
That’s why the opening conversation should never sound mechanical. A fit patient with strong performance status may be able to start at full schedule. An older patient, or someone already struggling with weakness or neuropathy, may need a modified plan from the beginning. Both decisions can be reasonable.
How Gemcitabine and Abraxane Work Together
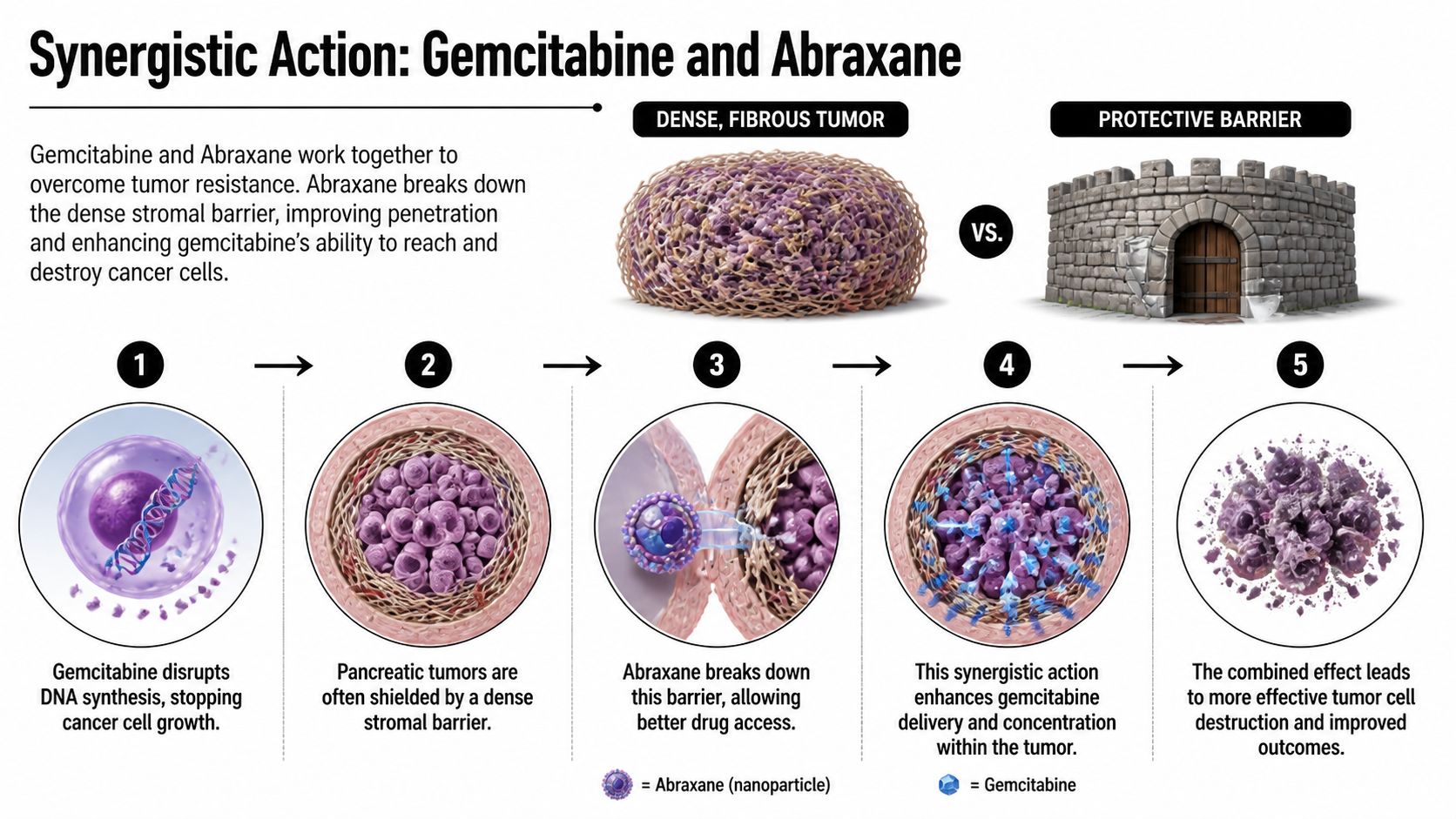
The science behind gemcitabine and Abraxane is easier to understand than most patients expect. Think of a pancreatic tumor as a target surrounded by dense, fibrous material. That outer layer acts like a barrier. One drug helps clear the path. The other does more of the direct damage once it gets in.
Gemcitabine is the drug that disrupts cancer cell DNA production. Cancer cells divide quickly, and gemcitabine interferes with that process. If you want a deeper explanation of the drug’s cell-level activity, Hirschfeld Oncology has a clear overview of the gemcitabine mechanism of action.
Abraxane, also called nab-paclitaxel, contributes in a different way. In the pancreatic setting, the combination is understood to work in part because nab-paclitaxel helps deplete the tumor stroma and improves intratumoral delivery of gemcitabine, which is described in the MPACT information on Abraxane and advanced pancreatic cancer.
The one-two treatment effect
Here’s the simplest explanation:
- Gemcitabine attacks cell replication. It interferes with DNA synthesis, which makes it harder for cancer cells to keep multiplying.
- Pancreatic tumors resist penetration. Their dense stromal environment can limit how well drugs reach the cancer.
- Abraxane helps open access. Its albumin-bound formulation supports delivery into the tumor environment and helps disrupt that protective barrier.
- More effective pairing follows. With better access, gemcitabine can reach more of the cells it needs to hit.
Why the pairing became so important
This is why oncologists don’t think of the regimen as two separate drugs happening to be given together. The point is synergy. One agent doesn’t just add to the other. It helps the other work better in a tumor type that is notoriously hard to penetrate.
When a regimen works in pancreatic cancer, it usually does so because it solves a practical problem of drug delivery, tumor biology, or both.
That’s the clinical appeal of gemcitabine and Abraxane. The pairing isn’t elegant only on a whiteboard. It addresses a real obstacle pancreatic tumors create.
Proven Efficacy for Pancreatic and Other Cancers
A common clinic conversation goes like this. A patient has just learned the cancer has spread, and the first question is not about theory. It is whether treatment can realistically slow the disease without making daily life intolerable. Gemcitabine and Abraxane became a standard first-line option because, in a large randomized trial, the combination improved survival, delayed progression, and increased tumor shrinkage compared with gemcitabine alone.
Those are three different kinds of benefit, and each matters in practice.
| Measure | What it means in real treatment decisions |
|---|---|
| Overall survival | Whether the regimen helps patients live longer after starting therapy |
| Progression-free survival | How long the cancer stays controlled before scans show growth |
| Tumor response rate | How often the tumor shrinks enough to relieve symptoms or reduce disease burden |
For pancreatic adenocarcinoma, that combination of benefits is why this regimen earned a durable place in first-line care. It can buy meaningful time. It can also improve how a patient feels if tumor control leads to less pain, better appetite, or less pressure on the bile duct or nearby organs.
The trial population also reflects an important real-world truth. Patients with better performance status usually tolerate treatment more consistently and often stay on therapy longer. In daily practice, that does not mean a less fit patient is excluded. It means the plan has to be adjusted thoughtfully. At Hirschfeld Oncology, that often starts with a frank discussion of goals, baseline strength, weight loss, neuropathy risk, and how aggressive the initial dosing should be. The same regimen can look very different in a healthy 58-year-old who is still working than in a 78-year-old who is already fatigued and losing weight.
That is one reason a specialized clinic adds value beyond following the package insert alone. Standard trial dosing proves a regimen works. It does not answer every question about how to keep a specific patient on treatment long enough to benefit. In practice, dose reductions, schedule changes, growth factor support in selected cases, and early symptom management often determine whether a patient receives one difficult cycle or several months of useful disease control. Patients exploring advanced pancreatic cancer treatment options should understand that effectiveness is tied to tolerability more often than trial tables suggest.
Outside pancreatic cancer, Abraxane also has established roles in other malignancies, including breast and lung cancer, but the strongest evidence for pairing it with gemcitabine remains in metastatic pancreatic cancer. That is the setting where the regimen has the clearest day-to-day relevance for treatment planning after diagnosis.
Supportive care around treatment also matters more than many patients expect. Fatigue, shortness of breath, and declining stamina can affect safety at home as much as they affect comfort in the infusion room. For patients who need home respiratory support during cancer care, some families also look for local options to buy oxygen equipment in St. Petersburg.
The practical takeaway is simple. Gemcitabine and Abraxane has earned its role because randomized evidence showed real benefit, and experienced oncology teams can often improve the day-to-day experience by adjusting the regimen to the patient rather than forcing the patient to fit the regimen.
Managing Side Effects and Maintaining Quality of Life
Patients rarely stop treatment because they dislike the idea of chemotherapy. They stop because side effects pile up faster than the body can recover. With gemcitabine and Abraxane, the work is to control toxicity early enough that treatment remains livable.
The side effects clinicians watch most closely are low blood counts, fatigue, nausea, hair loss, and peripheral neuropathy, which is numbness or tingling in the fingers and toes. Some patients have mild symptoms that are manageable. Others develop symptoms that force schedule changes unless the team intervenes quickly.
One useful lesson from practice is that the original weekly schedule isn’t the only reasonable way to use this regimen. A biweekly approach, given on days 1 and 15 every 28 days, has been studied as a less toxic alternative and showed acceptable toxicity with relative effectiveness in metastatic pancreatic cancer, as reported in this study of a biweekly gemcitabine and nab-paclitaxel regimen.
Common problems and what teams do about them
| Side Effect | What It Is | Common Management Strategies |
|---|---|---|
| Low white blood cells | Reduced infection-fighting cells after chemotherapy | Blood count checks, treatment delays when needed, growth factor support in selected patients, infection precautions |
| Peripheral neuropathy | Tingling, numbness, burning, or reduced dexterity in hands and feet | Early reporting, dose reduction of Abraxane, schedule modification, fall prevention, protecting hands and feet from injury |
| Fatigue | Persistent low energy that isn’t fixed by rest alone | Hydration, light activity when possible, anemia review, spacing activities, schedule changes if fatigue becomes cumulative |
| Nausea or poor appetite | Stomach upset and difficulty maintaining intake | Preventive anti-nausea medication, small frequent meals, hydration, nutrition support |
| Hair loss | Partial or substantial loss of hair during treatment | Advance preparation, head coverings if desired, scalp care, emotional support |
What patients should report early
Some side effects become harder to reverse if patients wait too long to mention them. Neuropathy is the clearest example. If numbness has started to affect buttoning clothes, writing, balance, or sleep, that’s not a detail to save for the next scan visit. It’s a treatment-management issue.
Call your team promptly if you notice:
- Fever or infection symptoms: Even mild fever matters during chemotherapy.
- New numbness or tingling: Early dose changes can prevent lasting nerve injury.
- Shortness of breath or unusual weakness: This may reflect anemia, dehydration, infection, or another treatment complication.
- Poor oral intake: Several bad days in a row can lead to a rapid drop in strength.
- Severe constipation or diarrhea: These problems can become serious quickly during chemotherapy.
Small symptoms become big problems when they cost a patient the ability to continue therapy.
Supportive care makes the regimen more usable
Supportive care isn’t an extra. It’s part of treatment. Some patients need anti-nausea medication before every cycle. Others need hydration, bowel support, or physical therapy guidance. In community practice, some patients receiving gemcitabine and Abraxane also need growth factor support for blood count issues.
When weakness or shortness of breath become part of the home picture, practical equipment can matter too. For families dealing with oxygen needs between visits, a local resource to buy oxygen equipment in St. Petersburg can be useful as part of broader symptom support planning, depending on where the patient lives and what the treating team recommends.
For a broader overview of day-to-day strategies, Hirschfeld Oncology also shares practical guidance on managing side effects of chemo.
The Hirschfeld Oncology Approach to Treatment
Standard protocols are valuable, but they don’t tell you what to do with the patient who is motivated for treatment, clearly symptomatic from cancer, and already a little frail before cycle one. That’s where oncology becomes less about memorizing a regimen and more about judging what a particular person can sustain.

An individualized approach often starts with a simple question. Is the goal to deliver the textbook schedule, or is the goal to keep the patient on effective therapy for as long as safely possible? Those aren’t always the same thing. In many real-world cases, a modified schedule preserves both quality of life and treatment continuity better than rigid adherence to the standard calendar.
A good example is the 21-day regimen, with gemcitabine and nab-paclitaxel on days 1 and 8 every 3 weeks. A real-world retrospective study found comparable efficacy with improved tolerability, including lower rates of severe neutropenia and fatigue, in patients needing a less intensive schedule, as described in this report on the modified 21-day regimen.
What personalization looks like in practice
At the clinic level, tailoring gemcitabine and Abraxane usually involves several decisions rather than one dramatic change:
- Starting dose choice: Some patients begin at standard dosing. Others start lower because waiting for toxicity to prove itself can be the wrong strategy.
- Schedule redesign: Moving from weekly treatment to a modified schedule can reduce cumulative fatigue and blood count suppression.
- Neuropathy prevention: If numbness begins early, Abraxane dose intensity may need adjustment before symptoms become functionally limiting.
- Rapid reassessment: Blood counts, weight trends, appetite, and symptom burden need frequent review, especially in the first cycles.
Why this matters for outcomes
Patients benefit from chemotherapy only if they can continue receiving it. A regimen that looks powerful on paper but repeatedly lands a patient in bed, in the emergency department, or too weak for the next cycle becomes self-defeating.
That’s why a specialized outpatient practice may lean into proactive changes rather than reactive ones. In practical terms, that can mean reducing intensity before a crisis, adding supportive medications earlier, or spacing visits differently for an older patient who is declining after each infusion.
Hirschfeld Oncology is one example of a Brooklyn infusion practice that uses individualized regimens, close monitoring, and symptom management for advanced cancers, including pancreatic cancer. The point of that model is factual and simple. Treatment is adjusted to match patient tolerability rather than forcing every patient into the same template.
The art of oncology is knowing when to push and when to modify. Both choices can serve the patient well if they’re made early and honestly.
Comparing Treatment Options and Future Directions
When discussing first-line therapy for metastatic pancreatic cancer, gemcitabine and Abraxane is usually considered alongside FOLFIRINOX. Both are established options. The choice between them depends less on ideology and more on fit.

The usual trade-offs
FOLFIRINOX is often selected for younger, fitter patients who may tolerate a more intensive regimen. Gemcitabine and Abraxane is frequently favored when clinicians want a strong first-line option that can be adapted more easily in the outpatient setting.
The comparison usually comes down to this:
| Consideration | Gemcitabine and Abraxane | FOLFIRINOX |
|---|---|---|
| Schedule flexibility | Often easier to modify with dose or timing changes | Can be harder to maintain in more fragile patients |
| Neuropathy risk | A real issue because of Abraxane | Also possible, though toxicity profile differs |
| Patient selection | Commonly used across a broad range of community patients | Often reserved for fitter patients |
No table can replace a clinical judgment call. A patient with borderline functional status may do better on a personalized gemcitabine and Abraxane schedule than on a regimen that is technically stronger but practically unsustainable.
Where the regimen may go next
The more interesting future direction is not just in metastatic disease. It’s in earlier-stage settings where treatment might improve the chance of surgery.
In a phase II trial for borderline resectable pancreatic cancer, neoadjuvant gemcitabine plus nab-paclitaxel achieved a median overall survival of 25 months, suggesting a potential role before surgery in selected patients, according to this phase II trial in borderline resectable pancreatic cancer.
That doesn’t make it the universal answer for borderline resectable disease. It does show that this regimen has value beyond palliative intent alone. For patients whose disease sits near the border between unresectable and operable, shrinking or stabilizing the tumor before surgery may create options that weren’t initially available.
Frequently Asked Questions About Treatment
How is gemcitabine and Abraxane given?
It’s given by intravenous infusion in an outpatient infusion center. The exact visit length varies by the center, the schedule being used, and how much premedication or supportive treatment is needed that day. Blood work is usually checked regularly because the regimen can lower blood counts and may need adjustment cycle to cycle.
Can I keep working during treatment?
Some patients do. Others can’t, at least not in the same way or on the same schedule. The deciding factors are usually fatigue, the physical demands of the job, neuropathy, and how your body handles treatment during the first few cycles.
A flexible employer helps. Remote work, shorter days, or lighter duties often make the difference between stopping work completely and staying partially engaged.
Do I need to follow a special diet?
There isn’t one universal “pancreatic chemo diet.” Most patients do best with food that is easy to tolerate, higher in protein when possible, and divided into smaller meals if appetite is poor. If nausea, early fullness, or weight loss becomes a problem, ask for nutrition input early rather than trying to fix it after you’ve already lost strength.
How long will I stay on this regimen?
There isn’t one fixed answer. Treatment usually continues while it is helping and remains tolerable. Doctors follow symptoms, blood counts, side effects, and scan results. If the cancer is responding but side effects are growing, many teams adjust the dose or schedule rather than stopping immediately.
What should I bring up at every visit?
Keep it simple and concrete. Tell your team about fever, numbness, falls, appetite loss, constipation, diarrhea, worsening pain, trouble sleeping, or how many hours you’re spending in bed. Those details often matter more than a general statement like “I’m doing okay.”
“Doing okay” can hide a lot. Specific symptoms help your team protect you and keep treatment on track.
If you or a family member is weighing treatment options for pancreatic cancer or another advanced gastrointestinal cancer, Hirschfeld Oncology offers consultations focused on individualized regimens, outpatient infusion care, and practical treatment planning built around both disease control and day-to-day tolerability.
.png)
.png)




