




.png)


You may be hearing about antibody-drug conjugates after standard treatments have already taken a lot out of you. Maybe surgery was followed by chemotherapy. Maybe one treatment helped for a while, then stopped. Maybe you or someone you love has reached the point where every new option sounds hopeful, but also hard to trust.
That mix of hope and caution makes sense.
When patients ask me what is an antibody drug conjugate, they usually aren't asking for a chemistry lesson. They want to know something simpler and more urgent. Is this a smarter treatment? Will it help if other treatments haven't? And what's the catch?
Antibody-drug conjugates, often shortened to ADCs, are one of the most important newer approaches in cancer treatment. They're designed to deliver a powerful anti-cancer drug more directly to cancer cells than standard chemotherapy can. That targeted design is the reason people sometimes describe them in glowing terms.
But there's another side patients deserve to hear clearly. ADCs are promising, but they are not side-effect-free, and they are not perfect “magic bullets.” They can still cause serious systemic side effects. Knowing both sides helps you ask better questions and make decisions with your eyes open.
A New Chapter in Cancer Treatment
You sit in an exam room after hearing that the last treatment is no longer working. Your family wants to know what comes next. Then a new term enters the conversation. Antibody-drug conjugate. It sounds highly technical, but the question underneath it is very human. Is this a treatment that can aim more carefully at the cancer without putting the whole body through the same kind of damage?
That hope is part of the story. So is caution.
Cancer treatment has expanded beyond the older model of surgery, radiation, and standard chemotherapy alone. In some cancers, doctors can now choose medicines based on features found on the tumor itself. ADCs belong to that newer group. They pair a lab-made antibody, which is designed to recognize a marker on certain cancer cells, with a very strong anti-cancer drug. If you want background on the targeting part, this explanation of how monoclonal antibodies work can help.
The basic idea sounds encouraging. Carry a potent drug closer to the cancer cell before releasing it. Many patients hear that and picture a treatment that attacks only the tumor. I always slow down at that point, because ADCs are more complicated than that. They are targeted treatments, but they are not perfectly selective treatments. Some normal tissues can still be affected, and side effects can still be serious.
That tension is what makes ADCs important to understand clearly. They represent years of work to improve on older approaches, not by removing toxicity, but by trying to direct more of a powerful drug toward cancer cells. In practice, patients and families need to prepare for both sides at once. There may be a more precise aim than standard chemotherapy alone, yet there can still be body-wide effects from the payload, the target itself, or the way the drug is processed after it enters the body.
The history of ADCs helps explain why this balance matters. The concept has been around for decades, and early versions often fell short because the treatment either did not work well enough or caused too much harm. Over time, researchers improved the antibodies, linkers, and payloads, and ADCs began to earn approval in more cancers. That long path is a reminder that this field was built through trial, setback, and refinement, not through a single breakthrough that solved every problem.
For many patients, ADC therapy opens a real option at a difficult moment. It can offer another way to treat cancer that has stopped responding to other therapies. It also requires honest preparation. The best conversations about ADCs include both the potential benefit and the dual-toxicity reality, meaning the treatment may be more directed than traditional chemotherapy while still causing meaningful systemic side effects. That balanced view helps families ask better questions and weigh treatment choices with clearer expectations.
The Three Parts of a Cancer-Targeting Smart Bomb
When people ask what is antibody drug conjugate in plain English, I often use a military analogy carefully. An ADC works like a smart bomb. It has a guidance system, an explosive payload, and a trigger that's supposed to activate in the right place.
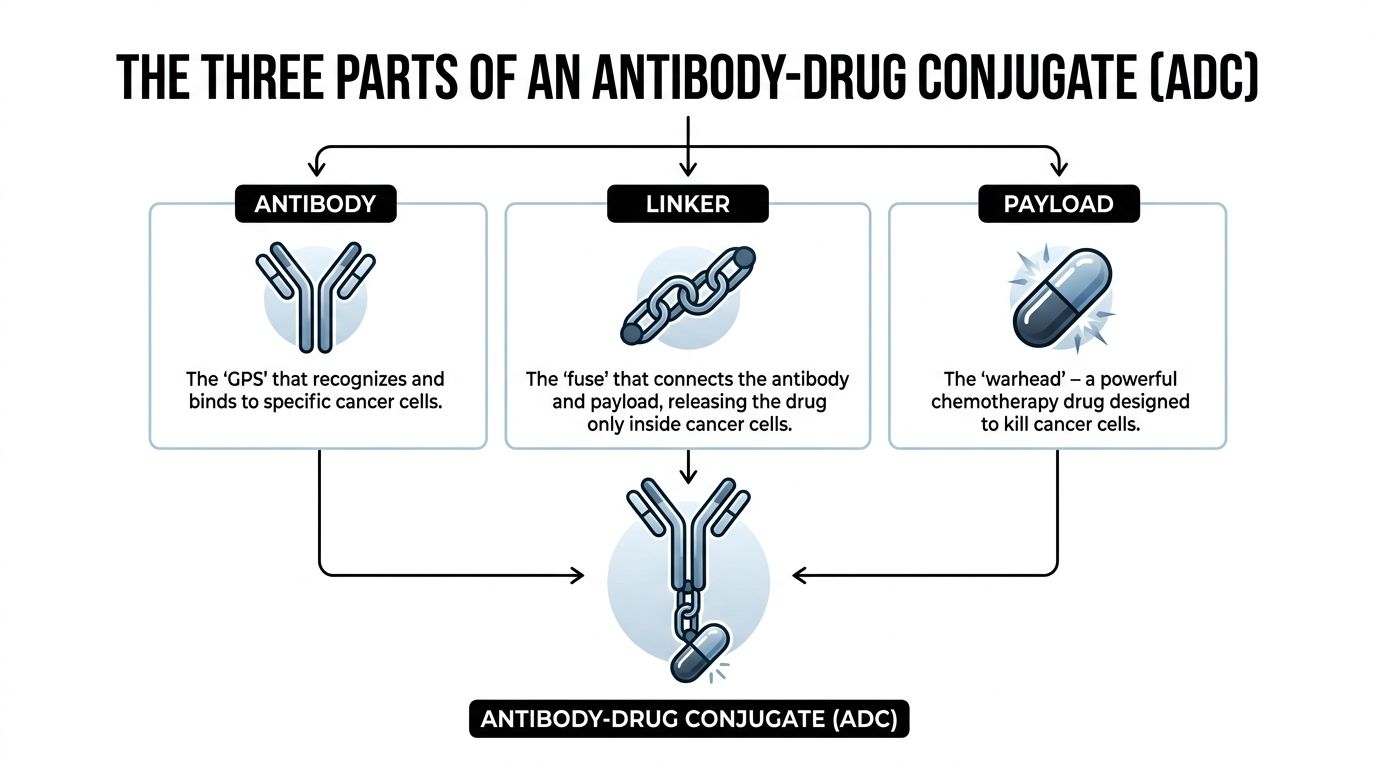
The antibody finds the target
The antibody is the homing device. It's built to recognize a specific marker, also called an antigen, on the surface of certain cancer cells. If you've ever wanted a simpler explanation of antibodies themselves, this guide on how monoclonal antibodies work is a helpful companion.
The key idea is selectivity. The antibody doesn't wander aimlessly. It's looking for a particular flag on the cancer cell.
The payload does the killing
The payload is the toxic drug attached to the antibody. This is not a mild medicine. ADC payloads are usually extremely potent because they're meant to kill cells after being delivered to a specific target.
That's where some confusion starts for patients. People hear “targeted therapy” and assume the drug itself must be gentle. It isn't. The payload is often stronger than what is typically imagined when thinking of standard chemotherapy.
The linker holds everything together
The linker is the chemical bridge between the antibody and the payload. It has one job that sounds simple but proves hard to engineer. It must stay stable while the ADC circulates in the bloodstream, then release the drug only after the ADC gets inside or near the intended cancer cell.
A review in Signal Transduction and Targeted Therapy describes ADCs as precision “biological missiles” made from a monoclonal antibody, a highly cytotoxic payload, and a chemically engineered linker designed to keep the toxic drug stable in circulation and release it intracellularly near the target cell, which helps minimize off-target toxicity in the right setting, as explained in this overview of ADC structure and function.
If the linker releases the payload too early, the treatment becomes less precise and more dangerous.
Why all three parts matter
An ADC only works well if all three parts work together:
- Right antibody: It must recognize a useful target on the cancer.
- Right payload: It must be strong enough to kill the cell once delivered.
- Right linker: It must stay intact long enough to avoid unwanted release.
If even one piece is poorly matched, the ADC may be less effective or more toxic than expected.
How Antibody Drug Conjugates Work in Your Body
The easiest way to understand an ADC is to follow its path through the body.
From infusion to contact
An ADC is usually given by infusion. After it enters the bloodstream, it circulates through the body and searches for cells carrying the antigen its antibody recognizes. That's the targeted part.
This is why ADCs are often grouped with targeted therapy options in cancer care. They aren't just floating chemotherapy. They're designed around a specific molecular target.
Once the antibody finds that target on a cancer cell, it binds to it. You can think of that moment as the lock finding its matching key.
What happens after binding
After binding, the cancer cell can pull the ADC inside. Doctors often call this internalization or endocytosis. Patients don't need to memorize those terms. The practical point is that the whole package gets taken into the cell.
Inside the cell, conditions allow the linker to break down or release the payload. The toxic drug is then freed where it can do the most damage to the cancer cell itself.
The payload may disrupt DNA or interfere with structures the cell needs to divide. Either way, the goal is the same. The cell is injured from the inside and dies.
This inside-the-cell delivery is what makes ADCs different from ordinary chemotherapy, which spreads its effects more broadly through the body.
Why the idea took so long to work
The logic behind ADCs has been around for a very long time, but making them work safely took decades. Early versions often had too much toxicity or too little benefit. Better antibodies, better linkers, and better payload design helped move the field forward.
If you want to see the process visually, this short video gives a useful overview of how the treatment reaches and affects cancer cells.
Where patients often get confused
A common misunderstanding is that the ADC acts only on cancer and nowhere else. That's not quite true. The design is more selective than traditional chemotherapy, but not perfectly selective.
Cancer biology is messy. Targets may not be expressed identically on every tumor cell, and healthy tissues can sometimes be affected too. That's why ADC treatment can be both impressively targeted and still difficult to tolerate for some patients.
Approved ADCs and the Cancers They Treat
A patient may hear an oncologist say, “You may be eligible for an antibody drug conjugate,” and assume that means a gentler, highly precise treatment. Sometimes it is more precise. It is not automatically gentle. That is why it helps to know which ADCs are already approved, what cancers they are used for, and why the match has to be so specific.
ADCs have moved from research into routine cancer care for selected patients. The number of approved drugs continues to grow, and the FDA list of approved oncology drugs shows how active this area has become. In practice, these medicines are used in cancers such as breast cancer, urothelial cancer, leukemia, and some gastrointestinal cancers, but only in the settings where testing, prior treatment history, and overall health support their use.
Examples you may hear by name
Patients often hear the brand name first. The details behind that name matter because each ADC is built to look for a different marker on cancer cells.
| Drug Name (Brand) | Target Cancer(s) | Antigen Target |
|---|---|---|
| Trastuzumab deruxtecan (Enhertu) | Breast cancer, gastric cancer, other HER2-expressing cancers in appropriate settings | HER2 |
| Ado-trastuzumab emtansine (Kadcyla) | Breast cancer | HER2 |
| Enfortumab vedotin (Padcev) | Urothelial cancer | Nectin-4 |
| Sacituzumab govitecan (Trodelvy) | Breast cancer, urothelial cancer in appropriate settings | Trop-2 |
| Gemtuzumab ozogamicin (Mylotarg) | Acute myeloid leukemia | CD33 |
| Inotuzumab ozogamicin (Besponsa) | Acute lymphoblastic leukemia | CD22 |
This table is a starting point. It does not answer the harder question a family usually asks, which is, “Is this the right drug for this person right now?” That decision depends on the exact diagnosis, stage, earlier treatments, biomarker results, organ function, and the side effect profile a patient is most likely to face.
Why the target changes everything
An ADC only makes sense if the tumor carries the marker the antibody is designed to find. A HER2-directed ADC needs HER2 expression. A CD33-directed ADC is used in a very different disease context than a Trop-2 directed ADC. The treatment and the target have to line up.
Tumor testing helps your care team make that call. You can picture it like a key and lock, but with an added complication. Some cancer cells may carry a lot of the target, some may carry very little, and some normal tissues may carry enough of it to contribute to side effects. That is part of the dual-toxicity reality. The drug may be more selective than standard chemotherapy, while still causing whole-body problems that need close monitoring.
A practical way to read the list
It helps to read an ADC table as a list of conditional options, not a menu. Approval means a drug has shown benefit in a particular cancer setting. It does not mean the drug fits every patient with that cancer, and it does not mean side effects will be mild.
For some families, seeing several approved ADCs on paper creates hope. Hope is appropriate. So is caution. The same features that make these drugs powerful can also lead to nerve problems, lung inflammation, low blood counts, liver test abnormalities, eye problems, or other toxicities depending on the specific ADC.
The importance of that balance is clear. Approved ADCs have opened important treatment options, especially for cancers that have become harder to treat. They also require a careful discussion about fit, timing, and risk before anyone can call them the right choice.
Understanding the Benefits and Risks of ADC Therapy
A common moment in clinic goes like this. A family hears that an antibody drug conjugate is a targeted therapy, and the room gets a little lighter. Then the next question comes quickly. If it is targeted, does that mean it will be easier on the body?
Sometimes it is. Sometimes it is not.
A primary benefit of an ADC is selectivity, not gentleness. The antibody helps carry treatment toward cells that display the right target, which can improve the chance of hitting the cancer while limiting some exposure to healthy tissue. That is why these drugs can help people whose cancer has stopped responding to other treatments.
But selectivity has limits. The payload attached to the antibody is still a very potent anti-cancer drug. Some normal tissues can still be affected, and some ADCs can release part of their payload in ways that lead to whole-body side effects. That is the dual-toxicity reality patients deserve to hear clearly before treatment starts.
The benefit patients hope for
When an ADC works, it combines precision with strength. The antibody helps with delivery. The payload does the cell-killing work after the drug reaches its target.
For a patient, that can mean another meaningful option after standard chemotherapy, hormone therapy, or earlier targeted treatments have lost effect. In some settings, ADCs can shrink tumors, delay cancer growth, or help control symptoms. Those are important gains, especially when choices are becoming fewer.
Hope belongs in this conversation. So does realism.
Why side effects still happen
Many articles describe ADCs in glowing terms and stop there. Patients need the fuller picture.
Researchers and drug developers continue to examine a central problem with ADC treatment: a drug can be targeted and still cause substantial systemic toxicity, including side effects serious enough to require dose delays, dose reductions, or stopping treatment, as discussed in this review of ADC challenges from Crown Bioscience. In plain language, the treatment may be more selective than standard chemotherapy, but it is still powerful medicine that can affect the whole body.
A useful comparison is asthma treatment. An inhaler is designed to deliver medication to the lungs, yet patients still need to learn about managing albuterol side effects because a targeted route does not eliminate body-wide effects. ADCs follow a similar principle, though with much higher stakes and very different risks.
Bottom line: Targeted does not mean harmless.
What risks patients should ask about
The side effects depend on the specific ADC, the payload it carries, your overall health, and the treatments you have already received. The pattern is not the same for every drug.
Common concerns include:
- Low blood counts. Neutropenia, thrombocytopenia, and anemia can raise the risk of infection, bleeding, or severe fatigue.
- Infusion-related reactions. Some people develop fever, chills, rash, shortness of breath, or a general feeling of being unwell during treatment.
- Organ-specific toxicities. Certain ADCs are associated with lung inflammation, liver injury, nerve damage, or eye problems.
- Everyday treatment burden. Nausea, poor appetite, weakness, and fatigue can still interfere with daily life even when the drug is working against the cancer.
Some ADCs also carry side effect patterns that are serious enough to shape who should receive the drug and how closely they need to be followed. That is one reason your oncologist may spend as much time discussing risk monitoring as benefit.
What a balanced decision looks like
A good ADC discussion is personal. It asks whether this exact drug matches your cancer biology, whether the likely benefit is meaningful in your situation, and whether the potential harms are acceptable to you.
For one patient, an ADC may offer a well-justified chance to control a hard-to-treat cancer. For another, the risk of severe toxicity may be too high, or a different treatment sequence may make more sense. Careful cancer care lives in that balance, with open eyes about both the promise and the price of treatment.
How Your Care Team Manages Side Effects
Good ADC care doesn't stop at choosing the drug. It depends on how carefully the team watches for problems and how quickly they respond.
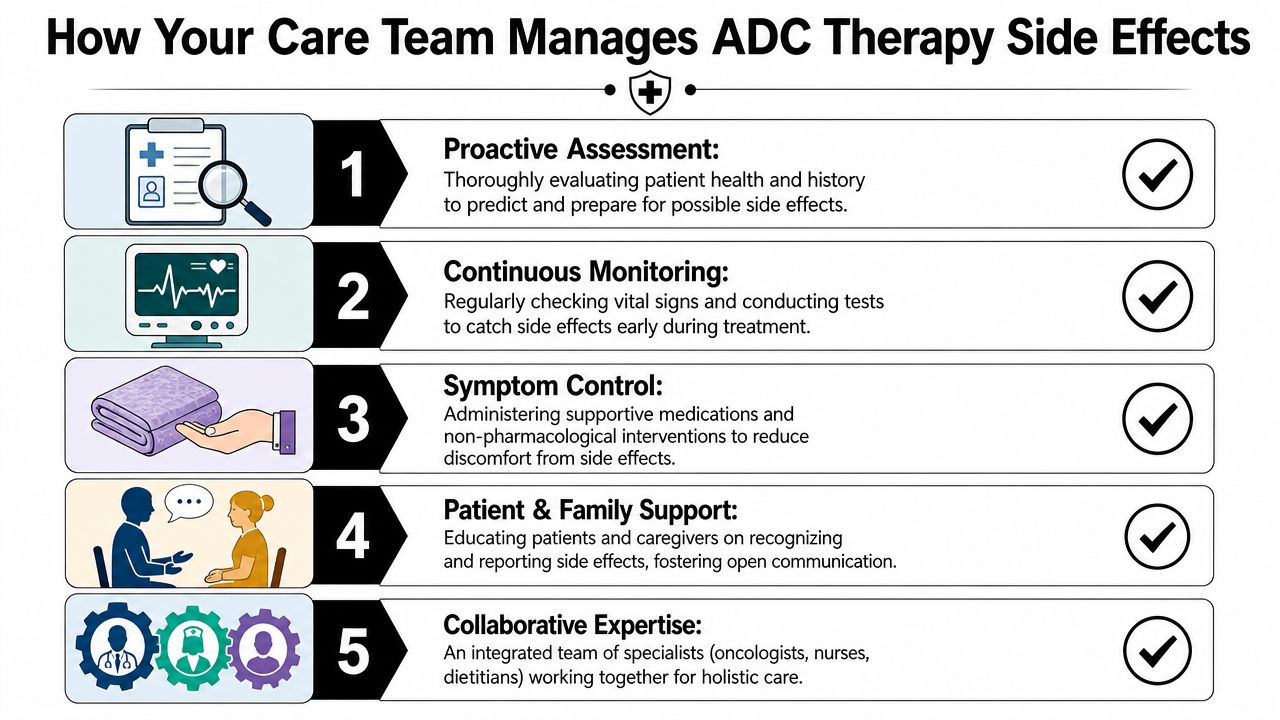
Monitoring starts before the first dose
An experienced oncology team looks at the whole picture before treatment begins. That includes the cancer type, prior therapies, blood counts, organ function, and any symptoms already affecting daily life.
The complexity of ADCs also matters on the manufacturing and quality side. They require close assessment of critical quality attributes such as drug-to-antibody ratio (DAR) and the presence of free cytotoxic payload, and regulators require rigorous validation to support batch consistency and safety, as outlined in this review of ADC analytical and regulatory oversight. Patients don't manage those technical details themselves, but they benefit when care teams respect how specialized these treatments are.
What side effect management usually looks like
In practice, side effect management is often a rhythm of prevention, monitoring, and adjustment.
- Regular blood work: Teams check blood counts to catch falling neutrophils or platelets before they become dangerous.
- Symptom review at each visit: New cough, shortness of breath, blurred vision, fever, numbness, or severe fatigue should be reported early.
- Premedications when needed: Some patients receive medications before infusion to reduce the chance of reactions.
- Dose changes: Oncologists may delay treatment, reduce the dose, or space infusions differently when side effects build up.
- Supportive care: Anti-nausea treatment, hydration, nutrition support, and infection precautions can make a real difference.
The safest patients are often the ones who report symptoms early, even if they seem minor.
Families play a bigger role than they realize
Caregivers often notice changes before the patient says anything. A loved one may spot worsening fatigue, confusion, poor appetite, eye irritation, or shortness of breath sooner than the person receiving treatment does.
That's why practical symptom education matters. Even outside oncology, patients benefit when side effects are explained in clear language. A plain-English resource on managing albuterol side effects shows how symptom-focused guidance can help people recognize problems sooner. The same principle applies during cancer treatment. Clear instructions reduce delay.
Questions worth asking at the start
Before starting an ADC, ask your care team:
- Which side effects are most concerning with this specific drug?
- What symptoms should trigger a same-day call?
- How often will blood work or other monitoring be needed?
- If side effects appear, will the plan be to pause, reduce, or switch treatment?
Those questions don't make you difficult. They make you prepared.
Exploring ADC Therapy in New York City
For patients in New York City, access matters almost as much as eligibility. It's one thing to read about newer cancer treatments. It's another to sit with an oncologist who can judge whether an ADC fits your disease, your treatment history, and your day-to-day priorities.

When ADCs enter the conversation
ADCs may come up after other treatments stop working, but that's not the only setting. They can also become relevant when a tumor carries a target that makes an ADC especially appealing, or when a physician is trying to balance anti-cancer activity with the hope of avoiding some of the broader damage of standard chemotherapy.
The right choice depends on details. A patient with metastatic breast cancer may face a different ADC discussion than someone with urothelial cancer, acute leukemia, or another advanced solid tumor. That's why personalized review matters more than headlines.
What to look for in a treatment center
When you're considering ADC therapy, look for a team that does more than prescribe. You want clinicians who can:
- Review prior treatment carefully: Sequence matters in advanced cancer care.
- Interpret biomarker testing: A target has to be present for an ADC to make sense.
- Monitor closely: These drugs require follow-up, not just infusion.
- Adjust quickly: Side effects should lead to action, not delay.
- Discuss alternatives openly: Sometimes another targeted treatment or immunotherapy path is more appropriate.
If you're also comparing newer options beyond ADCs, it can help to review how immunotherapy for cancer near me differs from other personalized treatment approaches.
The best next step is not the newest drug. It's the treatment that best matches the biology of the cancer and the needs of the person living with it.
A realistic but hopeful view
ADCs won't replace every other cancer treatment, and they won't help every patient. But they do represent a meaningful advance for many people facing resistant or advanced disease. They bring together precision and potency in a way older treatments often couldn't.
If you've been asking what is an antibody drug conjugate, the honest answer is this: it's a targeted cancer therapy that can be remarkably useful, but it demands respect. It offers hope, and it requires caution. Both are true at the same time.
If you or a loved one in Brooklyn, Williamsburg, Bushwick, or elsewhere in New York City is exploring advanced treatment options, Hirschfeld Oncology offers consultation and individualized cancer care built around careful decision-making, close monitoring, and realistic discussions of benefits and risks. For patients with complex or treatment-resistant cancers, including pancreatic, bile duct, breast, ovarian, colorectal, gastric, and esophageal cancers, Dr. Azriel Hirschfeld and his team can help you understand whether an ADC, immunotherapy, targeted therapy, or another individualized approach may fit your goals.
.png)
.png)




