




.png)


Your phone rings. A nurse says your bloodwork showed abnormal liver enzymes. You may not feel sick at all, yet the phrase lands hard. Many patients immediately wonder whether this means liver failure, cancer spread, or that treatment has stopped working.
Most of the time, that first call is not a diagnosis. It’s a signal. The liver releases certain enzymes into the blood when liver cells are irritated, when bile flow is slowed, or when something outside the liver is affecting it. In cancer care, those patterns matter because they can reflect the cancer itself, a blockage in the bile ducts, a medication effect, or a separate liver condition that needs attention.
The hardest part is that one lab report can feel both urgent and vague. Families often hear one number is “a little high” and assume it’s harmless. Others see several flagged results and fear the worst before anyone has explained what they mean. Both reactions are understandable.
What helps is learning how doctors read the pattern, not just the word abnormal.
That Call About Your Bloodwork Understanding Abnormal Liver Enzymes
A common scene in clinic goes like this. A patient checks a portal message, sees AST or ALT marked in red, and spends the next hour searching online. By the time we talk, they’re often carrying two opposite fears at once. “Maybe it’s nothing,” and “Maybe this changes everything.”
Both deserve a careful answer.
Think of liver enzymes as workers inside a factory. When the factory is under stress, some workers spill out into the bloodstream. A blood test picks that up. The result tells us the liver may be irritated or that bile may not be draining normally, but it does not tell us the cause by itself.
That distinction matters because abnormal liver enzymes can happen for many reasons. A fatty liver, alcohol, medications, supplements, viral infections, blocked bile ducts, tumors in or near the liver, and cancer treatments can all affect the same lab panel. The next step is to sort out which story fits your situation.
Research has shown this isn’t something to brush off casually. About 10% of Americans have abnormal liver enzymes, and even mild abnormalities have been linked to higher long-term mortality risk, with a standardized mortality ratio ranging from 1.21 to 1.78 in the cited research on asymptomatic abnormalities from EurekAlert's summary of Mayo Clinic liver enzyme findings.
Abnormal doesn’t always mean dangerous right now. It does mean the result deserves context.
If you’re in active cancer care, that context gets even more important. Some infections can affect the liver directly, and some viruses are also tied to cancer risk. If that’s part of your concern, this overview on how viruses can cause cancer can help frame the bigger picture.
The main message after that first phone call is simple. Stay calm, but don’t ignore it. Ask which enzymes are high, how high they are, whether the pattern fits liver-cell injury or bile-flow blockage, and what your team wants to do next.
Decoding the Patterns Hepatocellular vs Cholestatic
Doctors usually start by asking a basic question. Does the lab pattern look like liver cell irritation, or does it look more like bile drainage trouble?
That’s the difference between a hepatocellular pattern and a cholestatic pattern.
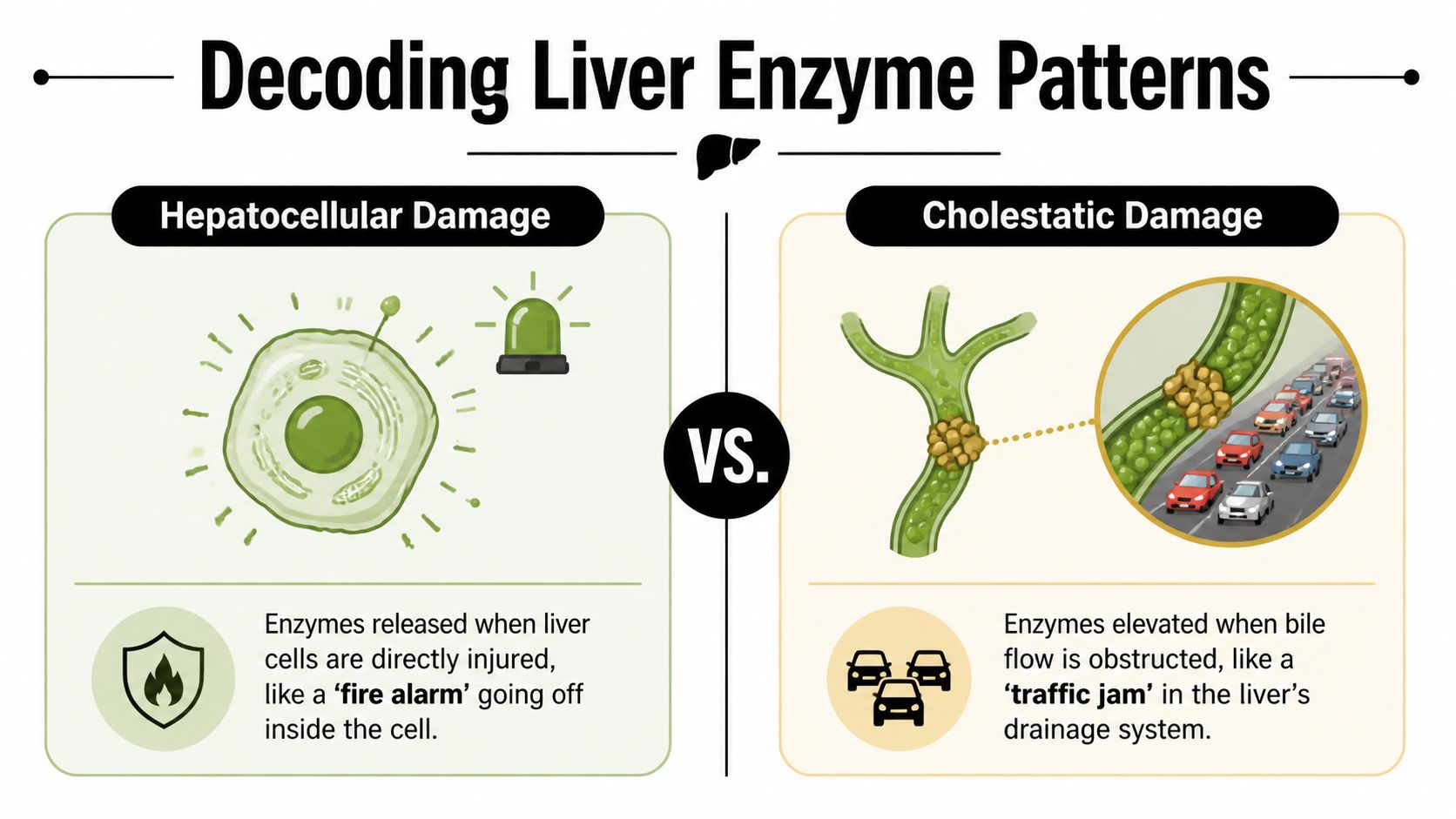
Hepatocellular pattern
In a hepatocellular pattern, the main enzymes that rise are ALT and AST. These are the markers doctors watch when liver cells themselves are inflamed or injured.
Using the factory analogy, this is the inside-the-building problem. The workers are sounding the alarm from within the production floor. That can happen with fatty liver disease, viral hepatitis, medication injury, immune-related inflammation, or cancer treatment side effects.
A few things often confuse patients here:
- AST is not liver-only. It can also rise from muscle injury and other non-liver causes.
- ALT is often more liver-specific. When ALT is increased, liver irritation becomes a stronger possibility.
- A mild increase still matters. A small rise can be temporary, but it shouldn’t be dismissed without context.
Cholestatic pattern
In a cholestatic pattern, the bigger clues are ALP and GGT, sometimes along with bilirubin. This pattern suggests that bile isn’t flowing the way it should.
That makes it the shipping department problem. The factory may be making bile, but the drainage route is backed up. A gallstone, inflammation, scar tissue, a tumor pressing on a duct, or cancer in the bile ducts can all create that traffic jam.
This pattern is especially important in oncology. A cholestatic pattern with increased ALP and GGT can point to obstruction from cancer involvement. In patients with colorectal cancer metastases, tumor-induced bile duct dilatation occurred in 16.5% of cases in the cited review, a finding discussed in this oncology-focused analysis of cholestatic liver test patterns.
Clinical clue: A single high number is less informative than the overall pattern. Doctors read ALT, AST, ALP, GGT, bilirubin, symptoms, and imaging together.
A simple comparison
| Pattern | Main labs doctors focus on | What it often suggests |
|---|---|---|
| Hepatocellular | ALT, AST | Irritation or injury of liver cells |
| Cholestatic | ALP, GGT, often bilirubin | Impaired bile flow or obstruction |
For patients and families, this is the first big turning point in understanding abnormal liver enzymes. The report isn’t just saying “something is off.” It’s often telling your doctor which direction to investigate first.
Common Culprits Beyond Cancer
Not every abnormal liver test in a cancer patient is caused by cancer. That’s important to say clearly, because people often jump straight to the most frightening explanation.
The most common non-cancer cause is nonalcoholic fatty liver disease, or NAFLD. It’s the leading cause of abnormal liver enzymes in the U.S. and a common reason for mild increases that show up on routine bloodwork. In the reviewed data, up to 7.9% of the U.S. population had increased AST, and more than 30% of initial abnormal results returned to normal when rechecked about 18 days later, as described in this review on elevated liver enzymes and NAFLD.

That repeat-testing point matters. Sometimes a result reflects a temporary strain, recent illness, dehydration, a lab variation, or a medication taken around the time of the blood draw. A repeat panel helps separate noise from a real ongoing problem.
The usual non-cancer categories
Fatty liver and metabolic strain
NAFLD often develops alongside weight gain, insulin resistance, diabetes, or high cholesterol. Many people have no symptoms at all. For a patient-friendly overview, Maryland Primary Care on fatty liver explains why it can stay silent for years.Alcohol use
Alcohol can inflame liver cells and worsen other liver conditions already present. In some patients, it also magnifies the stress of cancer treatment.Medications and supplements
Prescription drugs, over-the-counter pain relievers, herbal products, and “natural” supplements can all affect liver tests. Families are often surprised by this. If your list includes anything beyond prescribed cancer medicines, bring the bottles or photos to your visit.Viral hepatitis and infections
Hepatitis viruses remain part of the standard evaluation because they can directly inflame the liver.
Many “mild” abnormalities become clearer once your doctor reviews alcohol intake, supplements, recent antibiotics, pain medicines, and prior liver history.
Why history matters so much
A careful conversation often explains the lab pattern before any scan does. Doctors usually want to know:
- When the abnormal liver enzymes first appeared
- Whether they’re rising, stable, or improving
- Which medicines changed recently
- Whether there are symptoms like itching, dark urine, pale stools, nausea, or jaundice
If bile duct blockage is part of the concern, especially in someone with jaundice or duct-related pain, patients sometimes benefit from learning how biliary stent placement can relieve obstruction and improve liver drainage.
The Critical Link to Cancer and Treatment Toxicity
In oncology, abnormal liver enzymes usually raise two broad questions. Is the cancer affecting the liver or bile ducts? Or is the treatment affecting the liver?
Both are common enough that neither should be assumed without a full review.

When the cancer causes the abnormality
Some cancers spread to the liver. Others press on or grow into the bile ducts. In both situations, liver tests can change before symptoms become dramatic.
Colorectal cancer commonly metastasizes to the liver, and those tumors can alter enzyme levels. Pancreatic cancer is another major example. In the cited imaging review, over 50% of pancreatic cancer cases involved liver metastases at diagnosis, often with bile duct blockage and characteristic enzyme elevations, according to the AJR review on liver metastases and biliary findings.
For patients, this creates understandable confusion. A high enzyme level may reflect:
- tumor in the liver
- pressure on a bile duct
- inflammation around the pancreas or biliary tree
- reduced bile flow causing jaundice
Bile duct cancer, or cholangiocarcinoma, deserves special attention because it’s often overlooked outside specialist care. A persistent cholestatic pattern can be one of the earliest clues, especially when other explanations don’t fit.
When treatment causes the abnormality
Modern cancer therapy has changed what doctors watch for. Chemotherapy can inflame the liver. Targeted therapy can alter bile handling or trigger liver irritation. Immunotherapy can activate the immune system against healthy liver tissue in some patients.
That doesn’t mean treatment has failed or must stop permanently.
It means the team has to answer a practical question. Is this a manageable side effect, a sign of obstruction, or progression of disease? The treatment plan depends on that distinction.
Why oncology monitoring looks different
In general medicine, a mildly abnormal result may lead to a repeat test in a few weeks. In active cancer care, the timeline is often tighter because the liver may affect whether treatment can continue safely.
Doctors often track trends rather than reacting to a single value alone. They look at:
| Clinical question | Why it matters |
|---|---|
| Did the change start after a new drug? | Suggests treatment toxicity may be contributing |
| Is bilirubin rising with ALP and GGT? | Raises concern for biliary obstruction |
| Are scans showing liver lesions or duct changes? | Helps separate treatment effect from cancer effect |
| Are symptoms changing with the labs? | Adds urgency and guides next steps |
In cancer care, abnormal liver enzymes are often a decision-making tool. They influence imaging, treatment timing, dose adjustments, and whether a patient needs urgent biliary evaluation.
For families, one of the hardest moments is hearing that treatment may be paused while liver tests are investigated. That can feel like losing ground. In practice, short pauses and dose adjustments are often what make it possible to continue therapy safely instead of pushing through a preventable liver injury.
Your Roadmap for Evaluation and Red Flags
When patients hear “your liver enzymes are high,” they often want one immediate answer. What caused it? However, good evaluation follows a sequence.
Step one is to confirm the pattern
Doctors first look closely at which tests are abnormal. Is the rise mainly AST and ALT? Is it ALP and GGT? Is bilirubin high too? Then they compare the result with prior labs.
A trend tells a more useful story than one isolated test. A stable mild elevation is different from a sudden jump. A result that improves on repeat testing is different from one that keeps climbing.
Step two is to review the whole clinical picture
This is where details matter. Your team may ask about alcohol, supplements, acetaminophen, antibiotics, recent infusions, new targeted drugs, itching, fever, abdominal pain, appetite, urine color, and stool color.
That questioning can feel repetitive, but it’s not random. Many causes of abnormal liver enzymes look alike on paper and only separate once symptoms and timing are added.
Step three is to use imaging when needed
If the pattern suggests obstruction, tumor involvement, or a structural problem, imaging often follows. Depending on the situation, that may include ultrasound, CT, or MRI.
Here’s a patient-friendly video that helps explain how liver-related test abnormalities fit into a broader diagnostic process.
Red flags that need prompt attention
Some situations deserve faster action, especially in cancer care.
Yellowing of the eyes or skin
Jaundice can signal worsening bile blockage or reduced liver processing.Dark urine or pale stools
These changes often point toward a bile-flow problem rather than a minor incidental lab finding.New itching with high ALP and GGT
That combination raises concern for cholestasis.Persistent cholestatic labs without a clear benign cause
Persistently abnormal liver enzymes, especially a cholestatic pattern with high ALP and GGT, can be a red flag for cholangiocarcinoma. In the cited data, 25% to 30% of these cases first presented with abnormal liver function tests, with delays in diagnosis being common, as noted in this PubMed-indexed discussion of cholangiocarcinoma and liver test presentation.
Don’t focus only on whether a number is “high.” Focus on whether it’s persistent, worsening, and matched by symptoms or a cholestatic pattern.
Questions worth asking at your appointment
| Ask this | Why it helps |
|---|---|
| Which enzymes are elevated? | Clarifies the pattern |
| Do my labs suggest liver cell injury or bile duct blockage? | Guides the workup |
| Could this be from treatment, the cancer, or something separate? | Keeps the differential broad |
| Do I need repeat labs, imaging, or urgent evaluation? | Turns concern into a plan |
Patients and caregivers usually feel less overwhelmed once there’s a sequence. Confirm the result. Define the pattern. Review exposures and symptoms. Image the liver and bile ducts when the pattern points there. Escalate quickly if jaundice, obstruction, or persistent cholestatic abnormalities are present.
Managing Liver Health During Cancer Care
During treatment, the goal isn’t just to “watch the numbers.” The goal is to protect the liver so cancer therapy remains as safe and effective as possible.
That often means active management. A team may repeat labs before the next infusion, hold one drug while keeping another, reduce a dose, add supportive medicines, or arrange a procedure to relieve biliary obstruction. For immunotherapy, the question may be whether the immune system is inflaming the liver. For chemotherapy, it may be whether the liver needs time to recover before the next cycle.
What proactive management looks like
Some patients worry that any abnormal liver enzymes mean treatment has to stop. Usually, the main issue is how to continue thoughtfully.
- Trend-based decisions help separate a brief bump from a dangerous rise.
- Medication review can uncover a non-cancer drug or supplement that’s adding avoidable strain.
- Coordination across specialists matters when imaging, gastroenterology, interventional procedures, and oncology all intersect.
If treatment conversations are happening partly by telehealth or with family joining remotely, practical communication habits can make a real difference. These effective virtual meeting strategies are not cancer-specific, but they’re useful for organizing medication lists, questions, and caregiver participation before a complex visit.
Why careful monitoring supports treatment
Close monitoring is part of good cancer care, not a sign that things are falling apart. It’s often what allows a patient to stay on therapy longer and with fewer serious complications.
Patients also benefit from understanding the broader effects of chemotherapy, since liver enzyme changes may be one piece of a larger treatment picture that includes fatigue, appetite changes, blood count shifts, and medication timing.
Good liver management during cancer care is not passive. It’s how teams protect options.
For families, the most reassuring truth is this. A careful response to abnormal liver enzymes is often a sign that your team is paying close attention to the details that keep treatment possible.
Frequently Asked Questions About Liver Enzymes
Families usually ask practical questions first. That’s often where the most reassurance comes from.
| Question | Short answer | Why it matters | What to do next |
|---|---|---|---|
| Do abnormal liver enzymes always mean cancer is growing? | No. | Treatment effects, fatty liver, medications, infection, and bile duct problems can all change liver tests. | Ask your doctor what pattern your labs show and whether imaging is needed. |
| Can mildly abnormal liver enzymes still matter? | Yes. | “Mild” doesn’t always mean harmless, especially if results persist or fit a cholestatic pattern. | Follow through with repeat testing and recommended evaluation. |
| Should I stop my cancer treatment on my own if labs are abnormal? | No. | Stopping suddenly can create new problems and may not address the real cause. | Call your oncology team before changing anything. |
| Can diet help? | Sometimes. | Diet can support overall liver health, especially when fatty liver or poor intake is part of the picture. | Ask for individualized advice rather than trying supplements on your own. |
| Are supplements safe for the liver? | Not always. | “Natural” products can still irritate the liver or interact with treatment. | Show your care team every supplement you take. |
| When should we seek urgent help? | If jaundice, dark urine, pale stools, worsening abdominal pain, confusion, or rapid decline appear. | Symptoms can signal obstruction or significant liver stress. | Contact your doctor promptly or seek urgent evaluation. |
A final point matters more than any single answer. Abnormal liver enzymes are a clue, not the full story. The right response is careful interpretation, not panic and not delay.
If you or a loved one is trying to make sense of abnormal liver enzymes during cancer care, Hirschfeld Oncology offers educational resources and guidance focused on complex diagnoses, treatment tolerance, and thoughtful next steps. Their blog is a helpful place to learn more about advanced cancer care, liver-related complications, and supportive strategies for patients and families.
.png)
.png)




