




.png)


Many people start chemotherapy with one fear sitting louder than the rest: “What if I'm sick all the time?”
That fear is understandable. You may be staring at a bag of new prescriptions, hearing names like ondansetron, dexamethasone, or aprepitant, and wondering why one treatment seems to come with so many anti nausea medications for chemo. You may also be worried about whether you'll be able to eat, sleep, work, or feel like yourself.
The good news is that modern nausea care is built around prevention, not just rescue. The goal is no longer to wait for vomiting or severe queasiness and then react. Your oncology team usually builds a plan in advance, based on how likely your treatment is to trigger nausea and when that nausea is most likely to happen. If you're preparing for treatment, this guide on how to prepare for chemotherapy can also help you feel more grounded before your first infusion.
Navigating Your Concerns About Chemotherapy Nausea
A first chemotherapy visit often has a predictable moment. The conversation covers the cancer, the treatment schedule, and the logistics. Then the question that has been sitting underneath everything comes out: “Am I going to throw up from chemo?”
That question is about more than nausea. It is about control. It is about whether you will be able to eat dinner, sleep that night, ride home without getting sick, or walk into the next appointment without dread.
For some patients, the body starts reacting before the medicine is even infused. The National Cancer Institute's PDQ summary on nausea and vomiting related to cancer treatment describes anticipatory nausea and vomiting as a learned response that can happen before chemotherapy begins, especially after a difficult earlier experience. In plain language, the brain can start pairing the sights, smells, and routines of treatment with feeling sick.
That is why anti nausea medication for chemo is best understood as a strategy, not a pile of prescriptions. Your doctors are building layers of protection. One medicine may block an early signal. Another may last longer and cover the next phase after you get home. A third may be kept in reserve in case nausea breaks through anyway.
The plan is also personal. Two people can receive chemotherapy for the same cancer and still need different nausea prevention plans because their drug combinations, past motion sickness, pregnancy-related nausea history, anxiety level, and prior treatment experiences all matter. At Hirschfeld Oncology, that kind of tailoring becomes especially important in complex cases, where small adjustments in timing, drug choice, or home rescue medication can make the next cycle much easier.
A useful way to read your medication list is to ask, “What role does each one play, and when should I use it?” That question turns the plan from something being handed to you into something you can use with confidence. It also makes it easier to report back clearly if the plan needs work. If you are getting ready for your first infusion, this guide on how to prepare for chemotherapy before treatment day can help you feel more steady going in.
Practical rule: If your doctor prescribes several anti-nausea medicines, they are usually covering different triggers or different time windows, not reacting to a problem your body has already “failed” to handle.
Good nausea control starts with prevention, but it also depends on communication. If you felt fine in the infusion center but got sick that evening, say that. If the medicine helped the nausea but caused constipation or made you too sleepy, say that too. Those details give your oncology team the information they need to adjust the plan before the next cycle, which is often how nausea care improves from one treatment to the next.
Why Chemotherapy Can Cause Nausea
Nausea from chemotherapy can feel mysterious, but the basic pattern is easier to understand than it sounds. Think of your body as having an alarm system with more than one sensor. Chemotherapy can set off signals in the gut and in the brain, and those signals don't always happen at the same time.
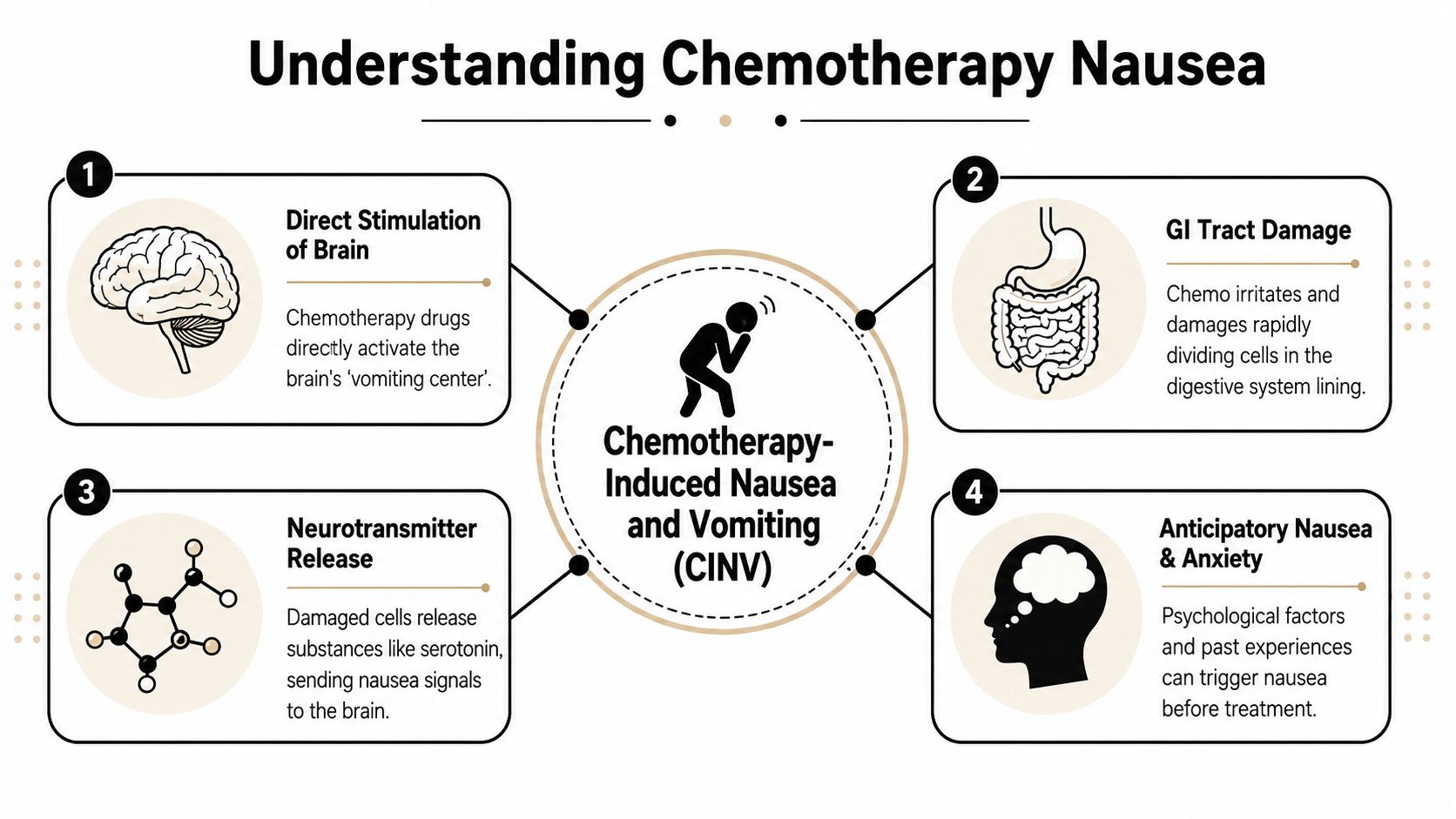
The first signal comes from the gut
Some chemotherapy drugs irritate cells in the digestive tract. Those cells can release serotonin, which then sends a fast “something is wrong” message toward the brain. This early pattern is one reason a 5-HT3 receptor antagonist such as ondansetron, granisetron, or palonosetron is often used as the backbone of prevention before treatment, as explained in this patient guide to anti-nausea drugs.
That early gut-to-brain message often shows up as acute nausea, meaning symptoms that happen soon after treatment. If you've ever wondered why your infusion nurse gives anti-nausea medicine before the chemotherapy starts, this is why. The team is trying to block the alarm before it rings.
A visual explanation can make this easier to grasp:
A later signal can come from a different pathway
Chemotherapy can also trigger a later nausea pathway involving Substance P. This can result in a person feeling fairly well on treatment day, then developing more trouble after getting home. That delayed pattern is why a single anti-nausea pill often isn't enough.
Here is the simple version:
- Early nausea pathway: Often linked to serotonin signaling from the gut.
- Delayed nausea pathway: Often linked to Substance P and brain-based signaling.
- Anticipatory nausea: Sometimes linked to prior bad experiences, anxiety, or learned associations with the treatment setting.
One medicine can block one doorway. Combination treatment tries to lock several doors at once.
Once you understand that, the logic behind combination therapy becomes much easier to accept. Your doctor is not piling on medicine without a reason. Your doctor is matching the plan to the biology.
Your Medication Toolkit for Preventing Nausea
The easiest way to think about anti nausea medication for chemo is as a toolkit. Each tool handles a different part of the problem. Some prevent the first wave. Some reduce delayed symptoms. Some are reserved for backup.
The American Cancer Society notes that 5-HT3 antagonists like ondansetron are typically given before chemo, while NK1 antagonists like aprepitant are especially useful for preventing delayed nausea. Dexamethasone is the most common steroid, and regimens for highly emetogenic chemo often combine these classes, with dosing continuing for 3 to 4 days post-infusion to manage delayed symptoms in its guide to medicines used for nausea and vomiting.
The main drug classes
5-HT3 receptor antagonists
These are often the front-line drugs for acute nausea prevention. They block serotonin-related signaling. Common examples include ondansetron, granisetron, and palonosetron.
NK1 receptor antagonists
These are especially important for delayed nausea. They block the Substance P pathway. Examples include aprepitant, fosaprepitant, rolapitant, and netupitant.
Corticosteroids
The steroid used most often for nausea prevention is dexamethasone. Patients are sometimes surprised that a steroid is part of an anti-nausea plan, but it often strengthens the effect of the rest of the regimen.
Olanzapine
Olanzapine is not just a psychiatric medication. In oncology, it is also used in some anti-nausea regimens, especially in more difficult cases or higher-risk settings.
Dopamine antagonists and phenothiazines
These are often rescue medications rather than the main preventive backbone. Prochlorperazine and promethazine are common examples.
Benzodiazepines
Lorazepam can help when nausea has a strong anticipatory or anxiety-related component.
Common anti-nausea medication classes for chemo
| Medication Class | Primary Target | Common Examples |
|---|---|---|
| 5-HT3 antagonists | Serotonin-related acute nausea signaling | Ondansetron, granisetron, palonosetron |
| NK1 antagonists | Substance P and delayed nausea signaling | Aprepitant, fosaprepitant, rolapitant, netupitant |
| Corticosteroids | Broad anti-nausea support in combination regimens | Dexamethasone |
| Atypical antipsychotic | Multi-receptor nausea control | Olanzapine |
| Dopamine antagonists and phenothiazines | Breakthrough or rescue nausea pathways | Prochlorperazine, promethazine |
| Benzodiazepines | Anticipatory or anxiety-associated nausea | Lorazepam |
Why patients get confused
Many people expect one medicine to do everything. That's rarely how this works.
A helpful analogy is a home security system. You might have one sensor on the front door, another on the window, and another motion detector inside the house. If you protect only one entry point, the alarm may still go off another way. Combination anti-nausea treatment works the same way.
Some patients also receive medicines in different forms and at different times:
- Before chemo in clinic: Often IV prevention
- At home after chemo: Often pills taken on a schedule
- As needed: Rescue medication if symptoms break through
That schedule can look complicated on paper. In practice, it's usually a very deliberate way to protect you through the full risk window, not just the first few hours.
How Doctors Create Your Anti-Nausea Plan
The plan usually starts before your first infusion. A patient sits down expecting to hear the name of one anti-nausea drug, then learns there may be a before-chemo medicine, home pills for the next few days, and a backup option if symptoms break through. That can sound like a lot. In reality, it reflects a strategy.
Doctors build the plan by asking two questions. First, how likely is this chemotherapy regimen to trigger nausea and vomiting? Second, what does this specific patient need on top of the standard starting point to stay ahead of symptoms?
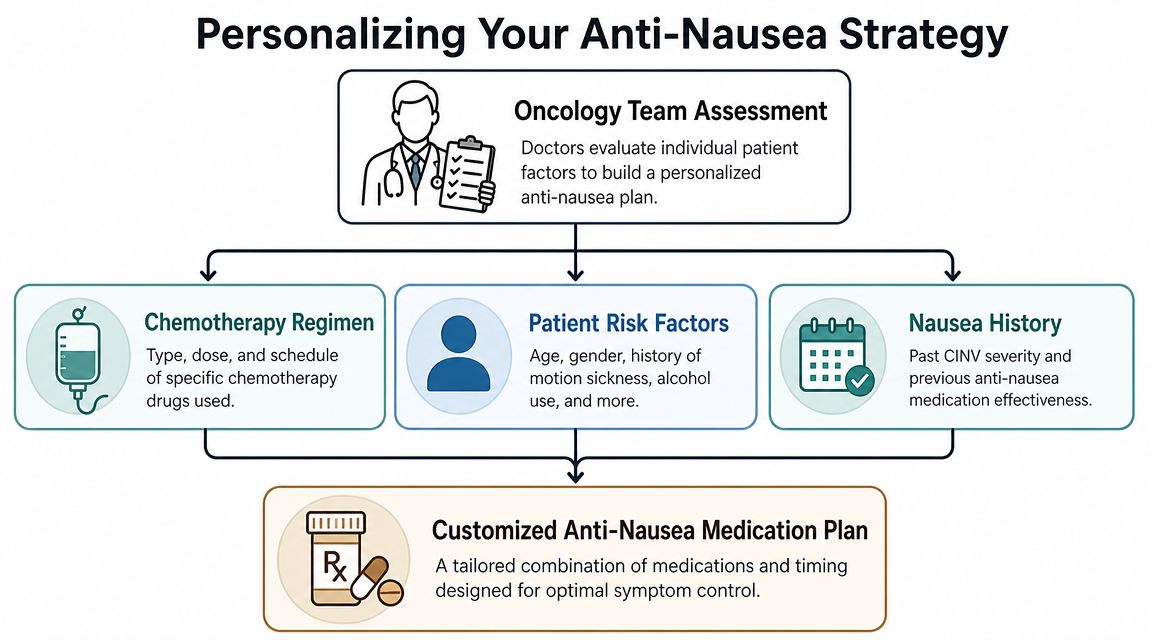
Risk level shapes the starting plan
The medical term for chemo-related nausea risk is emetogenic risk. It means how aggressive a regimen tends to be in provoking nausea and vomiting. That risk level gives doctors the first draft of your prevention plan.
According to the NCCN patient guidance on nausea and vomiting with cancer treatment, moderate-risk chemotherapy often starts with a 5-HT3 blocker plus dexamethasone, while higher-risk regimens often call for a three- or four-drug prevention plan that may include an NK1 blocker and olanzapine. The point is not to pile on medicine for its own sake. The point is to block more than one nausea signal before it has a chance to build.
A good comparison is weather preparation. A light rain forecast calls for a jacket. A hurricane warning calls for shutters, supplies, and an evacuation plan. The response changes because the threat changes.
Timing matters as much as drug choice
Many patients ask why some medicines are given in the infusion chair while others are scheduled at home later. The answer is that chemo nausea often comes in waves.
Some regimens are more likely to cause symptoms the same day. Others can trigger delayed nausea over the next several days. That is why the schedule may include medication before treatment and then continued protection afterward. Hirschfeld Oncology uses this same prevention-first approach when minimizing side effects during cancer treatment, especially when the risk window extends beyond infusion day.
If your calendar says to keep taking anti-nausea pills after you feel okay, there is usually a reason. Those doses are often there to prevent the second wave, not to react after you are already miserable.
Your history changes the final plan
Two people can receive the same chemotherapy and still need different prevention plans. Prior motion sickness, nausea during pregnancy, anxiety before treatment, trouble swallowing pills, constipation risk, diabetes, sedation concerns, and what happened in earlier cycles can all affect the final choice.
Patients can provide significant assistance. Tell your team what happened last time in plain language. Did nausea start at night? Did you vomit or just feel queasy? Did one medicine make you too sleepy to function? Those details help your oncologist adjust the next cycle more intelligently than a simple "yes" or "no" ever could.
At Hirschfeld Oncology, that individualized approach matters most in complex cases, including patients receiving combinations of therapies or patients whose symptoms do not follow the expected pattern. Sometimes the standard guideline plan is the right fit. Sometimes it needs careful adjustment and close follow-up.
The strategy is more important than memorizing the drug list
A clear anti-nausea plan usually follows this logic:
- Start with the chemo regimen. The treatment itself sets the baseline nausea risk.
- Match the prevention strength to that risk. Higher-risk regimens usually need more than one drug class working together.
- Cover the full timeline. Protection may need to continue after you leave the clinic.
- Adjust after each cycle. Your real-world experience helps refine the next plan.
That last step matters. If cycle one teaches your team that your nausea shows up late, or that a certain medicine causes constipation or heavy sedation, cycle two should reflect that.
Some patients also benefit from broader support if nausea overlaps with reflux, bowel changes, or appetite issues. In those situations, an integrative health approach to gut issues may be part of the conversation alongside standard oncology care.
If your medication list looks more detailed than expected, that often means your team is planning ahead. The goal is not limited to handing you drugs. The goal is to give you a prevention strategy you understand well enough to follow, monitor, and discuss with confidence.
Managing Breakthrough Nausea and Medication Side Effects
Even a good preventive plan can leave gaps. If nausea shows up despite your scheduled medicines, doctors call that breakthrough nausea. It doesn't mean you did anything wrong, and it doesn't mean your treatment has failed. It means the plan may need a backup layer.
Rescue medication works differently on purpose
Breakthrough nausea is often managed with a different pharmacologic class than the drugs used for prevention. As-needed rescue options commonly include dopamine antagonists like prochlorperazine, while lorazepam can help with anticipatory nausea, according to this childhood cancer support guide discussing anti-nausea drugs used during treatment.
That class-switching matters. If one receptor pathway has already been blocked and you still feel sick, your doctor may target a different pathway instead of repeating the same medicine.
What to do if you still feel sick
Patients often freeze in the moment because they're unsure whether to wait or take the rescue medication. Your own written instructions should guide you, but these habits help:
- Use the rescue drug early: If your team told you to take prochlorperazine as needed, waiting until you're miserable can make it harder to recover.
- Track the pattern: Note whether symptoms started after eating, overnight, or on a specific day after treatment.
- Report repeated breakthrough symptoms: If the same problem happens cycle after cycle, your team may change the prevention plan next time.
Don't judge the plan by one rough hour. Judge it by the pattern, then tell your team exactly what happened.
The anti-nausea drugs can have side effects too
This part often surprises people. The medicines that protect you from nausea can create their own annoyances.
Common examples patients notice include:
- Ondansetron: Constipation can become an issue.
- Dexamethasone: Some people feel wired, restless, or have trouble sleeping.
- Olanzapine: Drowsiness can be useful for some patients and frustrating for others.
- Prochlorperazine or promethazine: Sedation may occur.
If constipation starts becoming part of the problem, it can worsen overall abdominal discomfort and make nausea feel worse. Some patients appreciate a broader discussion of digestive side effects and medication burden, including this integrative health approach to gut issues, as a complementary way to think about symptom patterns.
Practical ways to stay ahead
- For constipation: Ask early whether you should start a bowel plan rather than waiting.
- For steroid-related insomnia: Ask whether morning dosing is appropriate for your schedule.
- For drowsiness: Don't drive or make important plans until you know how a rescue medicine affects you.
- For confusion about timing: Bring your pill bottles or medication list to every visit.
The main goal is simple. Your anti-nausea plan should reduce suffering, not leave you stuck choosing between nausea and chaos.
Beyond Pills Complementary Strategies for Nausea Control
Medicine is the foundation. Daily habits can make that foundation work better.
Some patients feel more in control when they have a short list of things they can do between visits. That matters. A good nausea plan includes both prescriptions and practical measures that lower triggers.
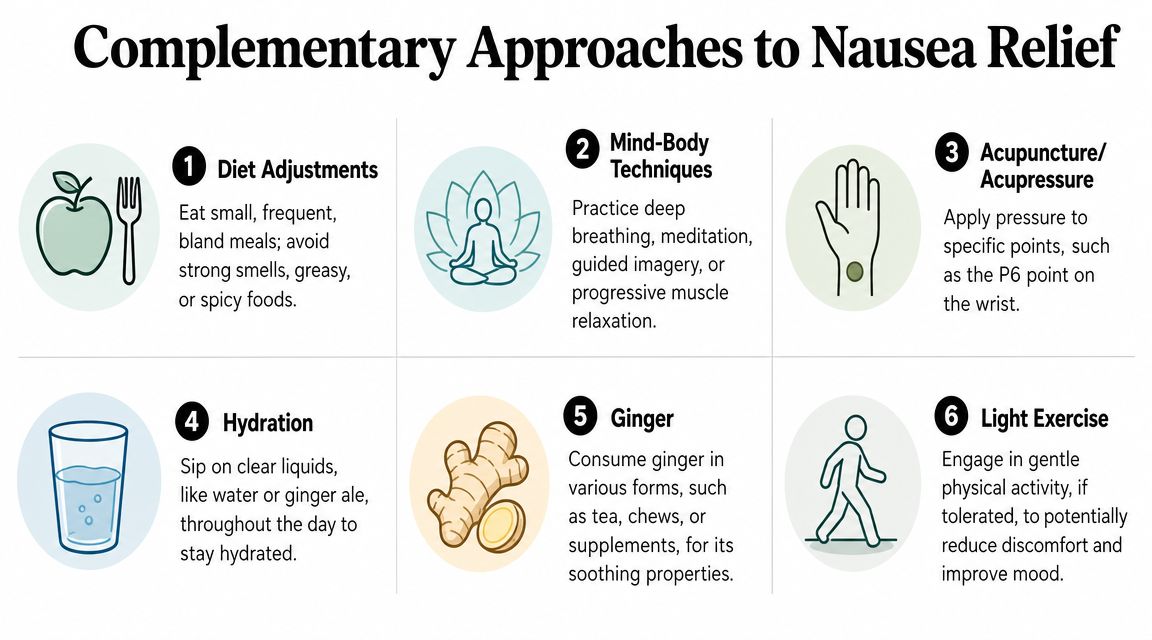
Daily habits that often help
- Small meals instead of large ones: An overly full stomach can be as uncomfortable as an empty one.
- Bland foods first: Crackers, toast, rice, bananas, or simple soups are often easier than greasy or spicy foods.
- Cool or room-temperature foods: Strong food smells can trigger nausea. Cooler foods often have less odor.
- Steady hydration: Sip through the day rather than forcing a large glass at once.
For practical nutrition ideas during treatment, this guide on what to eat during chemotherapy can help you identify foods that are easier to tolerate.
Sensory and mind-body support
The nervous system plays a role in nausea, especially when anxiety or past treatment experiences get mixed in. Some patients benefit from:
- Deep breathing or guided relaxation
- Acupressure wristbands aimed at the P6 point
- Light movement such as short walks, if tolerated
- A quiet eating environment without strong smells
Ginger and other soothing options
Ginger is one of the most commonly discussed natural supports for nausea. Some people prefer ginger tea, ginger chews, or ginger in food. If you're curious about topical or aromatic uses as part of a comfort routine, you may also want to discover ginger essential oil benefits.
These strategies are not replacements for prescribed anti nausea medication for chemo. They are add-ons. Think of them as ways to lower the volume on nausea triggers while your medical plan does the heavier work.
Partnering with Your Hirschfeld Oncology Team
The strongest nausea plan is not the one written on paper. It's the one that gets updated based on what happens to you.
That matters even more when treatment is complex. A major gap in patient information is how anti-nausea therapy is personalized when chemotherapy is combined with newer immunotherapy or targeted therapies. Public guidance often doesn't explain how those regimens can change nausea patterns, as discussed in this report on newer antiemetic guidance and personalization challenges.
What your team needs to hear from you
Be specific. “I was nauseated” is helpful, but “I felt fine on infusion day, then got queasy the next morning after breakfast and needed my rescue pill by noon” is much more useful.
Try to track:
- Timing: Did symptoms start in clinic, that night, or days later?
- Pattern: Was it constant nausea, sudden vomiting, or smell-triggered queasiness?
- Medication response: Which pill helped, and which one didn't seem to do much?
- Side effects: Did the anti-nausea medicine cause constipation, drowsiness, or insomnia?
When to call instead of waiting
Call sooner if you can't keep fluids down, your vomiting is recurring, or your rescue plan isn't working the way it was supposed to. Waiting until the next appointment can leave you dehydrated and miserable, and it also delays the chance to improve the next cycle.
Your oncology team can only personalize the plan if they know what your body actually did between visits.
For patients receiving combination regimens, novel protocols, or treatment after standard options have been exhausted, this feedback becomes even more important. In those settings, nausea may not follow the classic script, and the best care often comes from close monitoring and step-by-step adjustment.
If you're looking for a more individualized plan for nausea control during cancer treatment, explore the patient education resources and consultation options at Hirschfeld Oncology. Their blog offers practical guidance on symptom management, treatment side effects, and personalized oncology care for patients and families navigating complex cancer treatment.
.png)
.png)




