




.png)


You may be reading this after a cystoscopy report, a pathology call, or a portal message that introduced a term you had never heard before: bladder carcinoma in situ, often shortened to bladder CIS.
That moment is unsettling because the words pull in different directions. Carcinoma sounds serious. In situ sounds small or limited. Then someone mentions BCG, biopsies, close follow-up, and possibly even bladder removal if treatment doesn't work. It's a lot to absorb.
The most helpful way to approach this diagnosis is step by step. Bladder CIS is a serious form of bladder cancer, but it is also one where careful diagnosis, risk-aware treatment, and good follow-up can make a major difference. The hardest part for many patients is not just understanding what CIS is. It's understanding the decisions that come next, especially if first-line treatment doesn't do what everyone hoped.
What Is Bladder Carcinoma in Situ
A common and confusing moment happens after a cystoscopy or biopsy call. You hear that the cancer is "high-grade," but also "non-muscle-invasive." Those terms can seem to pull in opposite directions. Bladder carcinoma in situ, or bladder CIS, sits exactly in that uncomfortable space. It is serious because of how the cells behave, even though the disease is still limited to the inner lining.
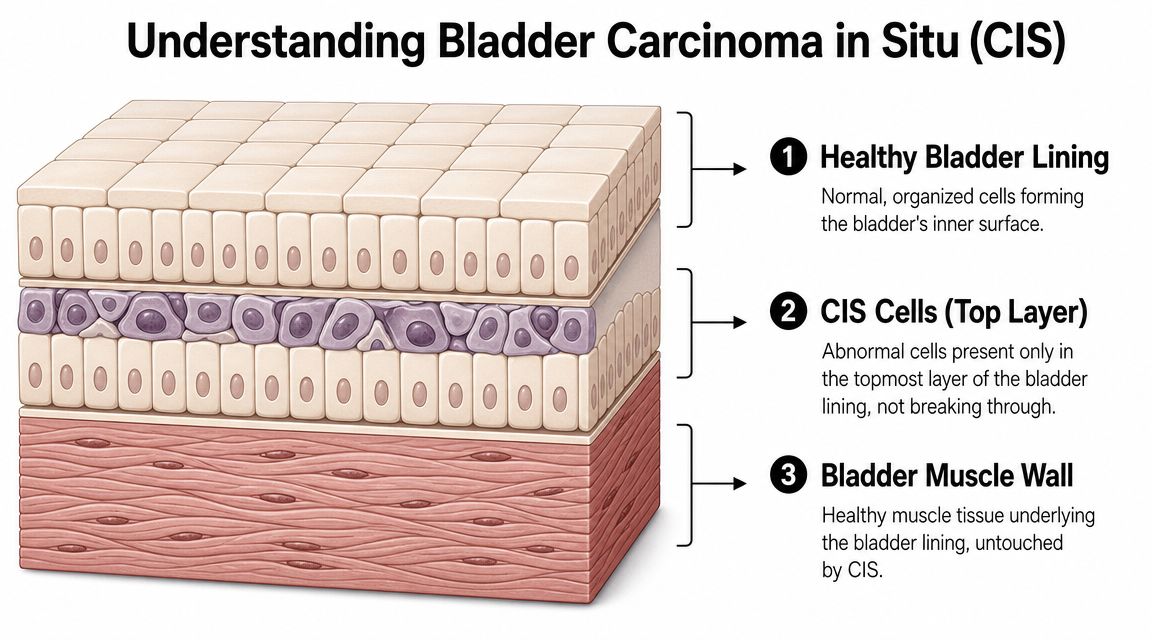
Bladder carcinoma in situ is a flat, high-grade, non-muscle-invasive cancer of the bladder lining. In plain language, the abnormal cells are spread across the surface layer instead of growing as a rounded tumor that projects into the bladder.
What each part of the name means
- Carcinoma means cancer that begins in lining tissue.
- In situ means the abnormal cells are still confined to the place where they started, the surface lining.
- High-grade means the cells look very abnormal under the microscope and are more likely to act aggressively.
- Non-muscle-invasive means the cancer has not grown into the deeper bladder muscle.
That last distinction determines treatment choices. A cancer confined to the lining is handled very differently from one that has reached the muscle wall, even when both require prompt attention.
Why CIS can be hard to recognize
CIS often does not form a clear bump, stalk, or mass. It can look like a reddened patch, a velvety area, or sometimes very little at all. For that reason, it may be missed on routine inspection unless the doctor is already suspicious from urine testing, symptoms, or biopsy results.
It can also be multifocal or diffuse. In other words, it may involve several areas of the bladder lining at once. That matters because treatment planning is not just about removing one spot. It is about deciding how to control a surface disease that can affect the bladder more broadly.
If you are reading your pathology before your appointment, this helpful guide to reading a pathology report can make the wording easier to follow. Some patients also start asking questions after abnormal urine findings, and this guide for urine test results can help you understand how those reports are commonly described.
Practical rule: In bladder CIS, "non-invasive" means "limited to the lining." It does not mean "low risk."
Why doctors treat it seriously
The concern with CIS is its biology. Pathologists see cells that already look aggressive, even before the cancer has grown into the bladder muscle. That is why your care team may recommend prompt treatment, close follow-up, and careful discussions about next steps if the first treatment does not clear it.
This becomes one of the key decision points after diagnosis. If CIS responds to bladder-sparing treatment such as BCG, the goal is to keep the disease controlled while protecting bladder function. If it does not respond, the conversation changes. At that point, your doctor is no longer asking only, "What is this?" The more important question becomes, "What is the safest next move before the cancer gains ground?"
For patients and families, that is the central idea to hold onto. CIS is contained, but it is not minor. Understanding that early helps the later treatment choices make more sense.
How Doctors Diagnose Bladder CIS
A common scene goes like this. Someone has blood in the urine, or weeks of urgency and burning that keep getting brushed off as infection. The first tests may be unclear. Then a bladder exam looks only mildly abnormal, yet the doctor still recommends biopsy because the story does not fully add up. That extra step often matters in CIS.
Bladder CIS can hide in plain sight. It often behaves more like a thin patch of damaged lining than a lump you can easily see and remove. That is why diagnosis usually depends on several pieces of evidence that are interpreted together, not on one test alone.
A typical diagnostic sequence
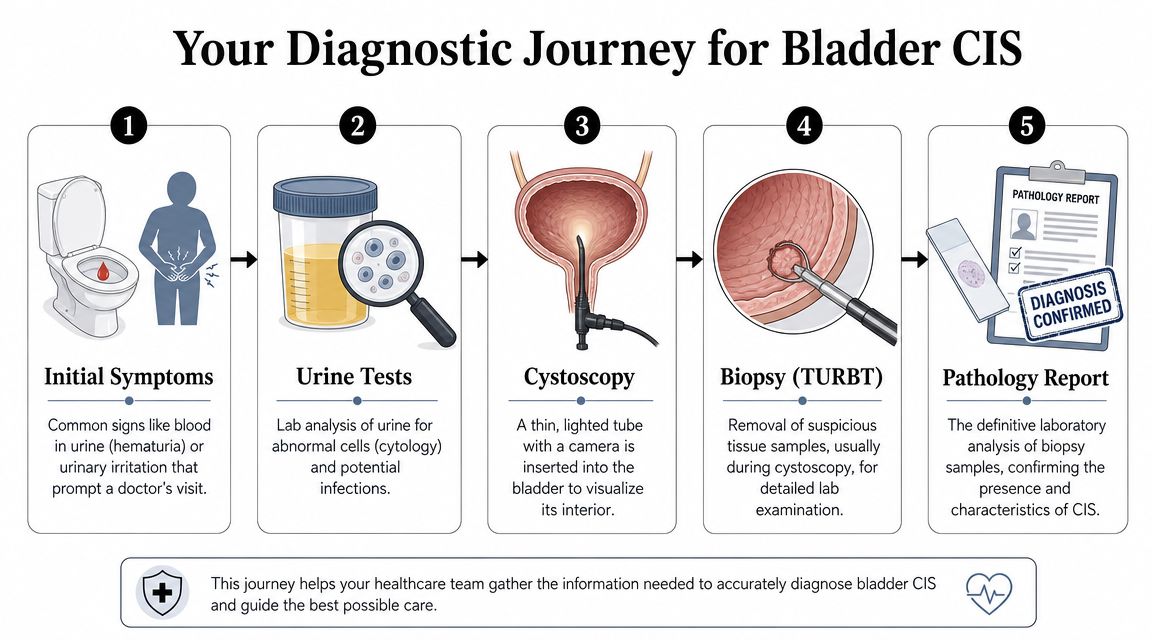
Urine testing often starts the workup
Doctors usually begin with urine studies to check for blood, infection, and abnormal cells. Urine cytology can be especially helpful in CIS because cancer cells may shed into the urine even when there is no obvious mass. If you are trying to sort through unfamiliar lab terms before your visit, this guide for urine test results can help you understand how urine findings are commonly described.Cystoscopy gives a direct look inside the bladder
During cystoscopy, a thin camera passes through the urethra into the bladder so the urologist can inspect the lining. This test is very good at finding many bladder tumors. CIS is harder because it is flat. It may appear as a red, irritated, velvety, or only slightly abnormal area, and sometimes it is not obvious at all under standard white light.Biopsy settles the question
If the lining looks suspicious, or if urine findings suggest cancer despite a subtle exam, the urologist may take tissue samples from the bladder. This is often done during TURBT or a directed biopsy procedure. Under the microscope, the pathologist can tell whether the cells are cancerous, whether they are high grade, and whether they remain limited to the inner lining.
Why diagnosis can take more than one test
Families often ask, "If the camera looked almost normal, why do we still need biopsy?" The reason is simple. CIS can be present as a thin sheet of abnormal cells spread across the surface, like a stain on wallpaper rather than a bump in the wall. A camera can miss that pattern. Cytology may raise suspicion first, and biopsy confirms whether that suspicion is correct.
This is also why some urologists use more than one sampling approach. Depending on the situation, they may take targeted biopsies from areas that look suspicious, sample other parts of the bladder lining, or use enhanced imaging techniques to make subtle areas easier to spot. These decisions matter because the diagnosis shapes the next major treatment choice, especially if later discussions involve whether BCG is working well enough or whether a different plan should be considered.
In bladder CIS, a reassuring appearance on cystoscopy does not always close the case. Urine cytology, biopsy, and pathology often carry equal weight.
The pathology report is the final checkpoint
The pathology report is the document that turns suspicion into a firm diagnosis. It tells your team what type of abnormal cells were found and whether they are still confined to the lining. That distinction guides the whole treatment strategy.
Many patients find this report intimidating because it is written for clinicians. If you want help translating the wording, this explanation of how to read a pathology report can make the terms easier to follow.
For patients and families, the key idea is this. Diagnosing bladder CIS is often a process of putting clues together carefully. That can feel slow, but it is how doctors make sure the next decision is based on the clearest possible picture.
Standard Treatment with BCG Intravesical Therapy
A CIS diagnosis often leads to a very practical question: if the abnormal cells are spread along the bladder lining, what treatment can reach that whole surface?
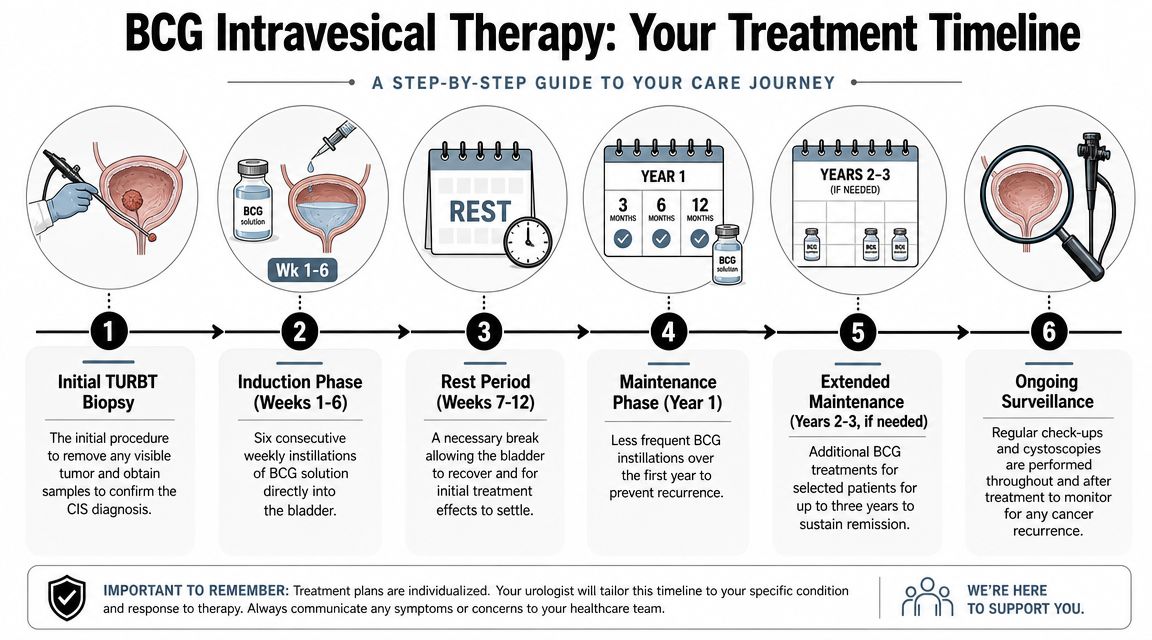
For many patients, the first step is still to make sure any visible lesion has been removed or sampled with TURBT. That matters because CIS can exist alongside other bladder tumors. But TURBT alone usually does not solve CIS, since the disease often behaves more like paint spread across a wall than a single spot that can be cut out.
That is why the standard treatment is usually BCG intravesical therapy.
What BCG is
BCG stands for Bacillus Calmette-Guérin. It is a weakened bacterium. In bladder cancer care, doctors place it directly into the bladder through a catheter so it can act on the bladder lining itself.
BCG works like a local fire alarm for the immune system. Its job is to stir up an immune response inside the bladder so immune cells are more likely to recognize and attack abnormal cells on that lining. That local approach is one reason it has remained a standard treatment for high-risk non-muscle-invasive disease, including CIS, as described in the American Urological Association guideline for non-muscle-invasive bladder cancer.
If you want a broader overview of immune-based cancer treatment, this overview of cancer immunotherapy can help place BCG in context.
What treatment usually feels like
BCG is usually given during a short outpatient visit. A catheter is placed into the bladder, the medication is instilled, and you hold it for a period of time before urinating it out.
The schedule sounds simple on paper. Living through it can feel less simple.
Many patients find the visits themselves manageable, while the bladder irritation builds over time. Burning with urination, urgency, frequency, fatigue, and flu-like symptoms are common reasons people call the clinic with questions. Some weeks feel harder than others. A milder treatment day does not automatically mean the treatment failed.
Keeping a clear record can make these visits more useful. Some patients track the date of each instillation, symptoms afterward, fever, urinary changes, and questions for the next appointment. Even a general planning tool such as these Simbie AI treatment plan templates can be a practical way to organize what happened after each instillation and what to ask at the next visit.
Later in treatment, it may help to hear the process explained visually and verbally:
Why maintenance matters
One of the most common points of confusion is the difference between induction and maintenance. Patients often hear both terms early, but the reason for using both is not always explained clearly.
| Phase | What it means in practice | Why it matters |
|---|---|---|
| Induction | The initial course, often given weekly over several treatments | This starts the immune response in the bladder lining |
| Maintenance | Additional treatments spaced out over time | This helps keep that response active and lowers the chance that CIS returns |
The easiest way to understand it is to compare BCG with training rather than a one-time repair. Induction gets the immune system's attention. Maintenance helps it stay alert. For CIS, that distinction can shape the next major decision, because a patient who completes only induction may have a different discussion with their doctor than someone who has already had an adequate course of BCG and still has persistent disease.
What I tell patients: BCG is not just a series of appointments. It is an organized attempt to control a high-risk lining cancer while keeping the bladder. Knowing whether you have had induction alone or induction plus maintenance becomes very important if the cancer does not fully respond.
When BCG Fails Advanced Treatment Options
You finish treatment expecting the next cystoscopy to bring relief. Instead, your doctor says the CIS is still there, or it returned soon after BCG. For many families, this is the moment when the conversation changes. The question is no longer just, "What is CIS?" It becomes, "What should we do now, and how do we choose well?"
At that point, you may hear the term BCG-unresponsive. In plain language, it means the cancer has shown that standard BCG is not controlling it well enough. That label matters because it changes the strategy. Repeating the same plan usually makes less sense once the tumor has shown you how it behaves.
The three main paths doctors discuss
After BCG failure, the decision is rarely about finding one perfect answer. It is about choosing the next best move based on three things: how aggressive the CIS appears, how fit you are for treatment, and what trade-offs you can realistically live with.
Another bladder-directed treatment
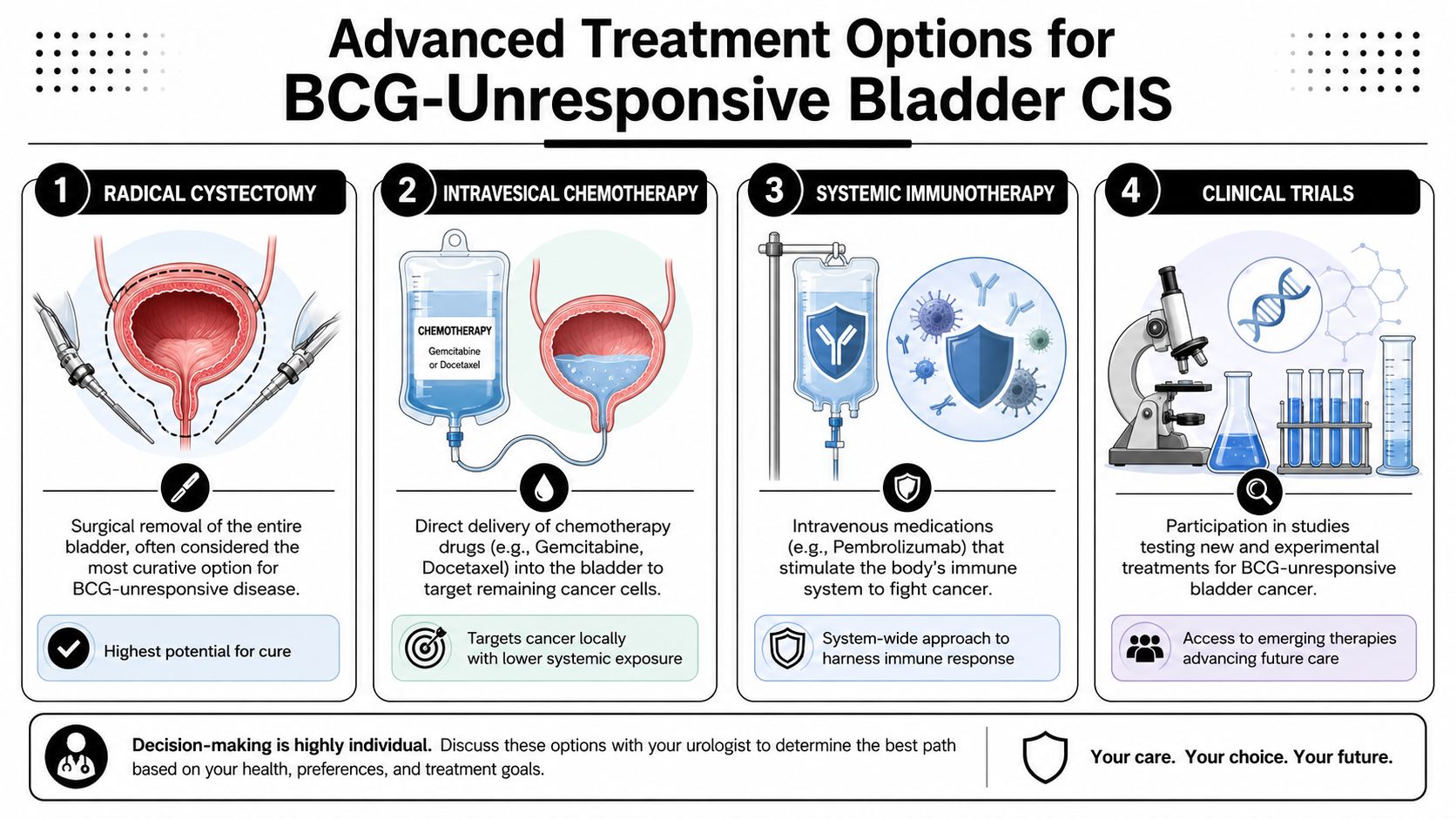
Some patients pursue another intravesical treatment, which means medicine placed directly into the bladder. This approach tries to preserve the bladder while treating the lining where CIS lives.
A useful comparison is this: if radical cystectomy removes the whole room because a fire keeps restarting, intravesical therapy is another attempt to put out the fire without tearing down the house. That can be reasonable for selected patients, especially if surgery is high risk or bladder preservation is a top priority. But it requires a clear-eyed discussion about the chance that the cancer may persist or return.
Systemic immunotherapy
Another option is systemic immunotherapy, such as pembrolizumab. It is given by IV and works throughout the body, not only inside the bladder.
This often confuses patients because BCG is also an immune treatment. The difference is location. BCG tries to stir up an immune response in the bladder lining itself. Systemic immunotherapy changes immune signaling more broadly, which can offer a bladder-preserving path for some patients after BCG has failed. The trade-off is a different set of side effects, including immune-related problems that can affect organs outside the urinary tract.
Radical cystectomy
Radical cystectomy, or bladder removal, remains the most definitive option for BCG-unresponsive CIS. It offers the strongest cancer control because it removes the organ where the cancer continues to persist or recur.
It is also major life-changing surgery. Patients deserve time to understand urinary diversion, recovery, sexual side effects, and day-to-day function after surgery. In my experience, fear often comes from vagueness. The more concrete the discussion becomes, the more manageable this choice feels.
How to frame the decision
A practical way to organize this discussion is to focus on three questions.
- How much cancer control is this option likely to give me? Surgery usually offers the clearest control. Bladder-sparing options may preserve the organ, but they ask you to accept more uncertainty.
- What burdens come with this treatment? Some burdens are short term, such as recovery from surgery. Others are ongoing, such as repeated bladder treatments, IV visits, or immune side effects.
- What matters most to me right now? One patient may prioritize keeping the bladder if there is a reasonable path to do so. Another may decide that removing the bladder is worth it for the strongest chance of control.
This is the real crossroads after BCG failure. Radical cystectomy has long been the standard option for many patients with BCG-unresponsive CIS because of the risk that high-grade lining disease can progress. At the same time, bladder-preserving approaches may still be appropriate for selected patients who understand the trade-offs and have a careful follow-up plan with their team.
For patients who have limited standard options or want to ask about newer approaches, it is reasonable to discuss immunotherapy clinical trials with your doctor. A trial does not promise a better result, but it may give access to treatments that are not otherwise available.
If you're in New York and want a medical oncology perspective alongside urologic care, Hirschfeld Oncology offers bladder cancer consultations and treatment planning as one option among the specialist resources patients may consider.
Surveillance Prognosis and Life After Treatment
For many patients, the emotional low point doesn't come at diagnosis. It comes after treatment, when they expect to feel “done” and instead learn they'll need ongoing surveillance.
That follow-up is not a sign that treatment failed. In bladder CIS, surveillance is part of treatment. The disease can be subtle, and early recurrence is easier to address than delayed recurrence.
Why follow-up stays close
Doctors usually continue watching the bladder with repeated cystoscopy, urine testing, and sometimes additional biopsies when findings are unclear. The schedule is often more frequent early on, then adjusted over time depending on what your bladder shows.
This can feel tiring, but there is a strong logic behind it. CIS is a lining disease that may recur in ways that aren't obvious from symptoms alone. A patient can feel fairly well and still need a careful look inside.
Follow-up visits are not a vote of no confidence. They are how your team keeps small problems from becoming big ones.
What prognosis really means here
Patients often ask, “So what's my prognosis?” What they usually mean is, “Can this be managed, and how worried should I be every day?”
The answer depends on whether the CIS responds to treatment, whether it stays confined to the lining, and whether surveillance catches any return early. A good outlook in CIS is usually built, not granted. It comes from a combination of effective treatment, reliable follow-up, and timely action when something changes.
A helpful way to view prognosis is this:
| Situation | What it generally means |
|---|---|
| CIS responds and surveillance stays clear | The path is more reassuring, but follow-up remains important |
| CIS recurs but is caught promptly | You and your team still have decision points and treatment options |
| CIS persists after standard therapy | The discussion becomes more specialized and often more urgent |
Living with the uncertainty
The surveillance cycle can trigger anxiety before every urine test or cystoscopy. That's normal. Many families find it useful to treat follow-up as a routine health practice rather than a looming verdict.
A few habits can help:
- Keep a simple record of procedures, pathology, and symptoms.
- Bring the same core questions to each visit so you can compare answers over time.
- Report changes early, especially bleeding, worsening irritation, or anything new that persists.
- Ask what result would change the plan, because that tells you what your doctors are watching for.
Life after treatment for bladder CIS often involves learning how to live well while staying medically attentive. Those two goals can coexist.
When to Seek a Second Opinion or Specialist
A second opinion isn't a sign of distrust. In cancer care, it's often a sign that you're taking the diagnosis seriously enough to confirm the strategy.
This matters most when the next decision is large, irreversible, or unusually complex. Bladder CIS can reach that point quickly, especially after BCG.
Situations where a second opinion is wise
BCG hasn't worked as hoped
If the cancer persists or returns after appropriate BCG, you're at a genuine crossroads. Another specialist may help clarify whether more bladder-directed therapy is reasonable or whether the window for cystectomy should be discussed more urgently.You're being advised to consider bladder removal
Radical cystectomy is an important and sometimes necessary option. It's also a life-changing surgery. Confirming the recommendation with a specialist is sensible.Your test results and your symptoms don't seem to match
CIS can be visually subtle. If urine tests suggest disease but the bladder doesn't look convincing, a center or clinician with deep experience in high-risk non-muscle-invasive disease may add useful perspective.You want to explore treatments not offered locally
Some practices focus mostly on standard pathways. Others may discuss additional intravesical approaches, systemic immunotherapy, or trial enrollment.
What a good second opinion should do
A useful second opinion should answer three things clearly:
- Do they agree with the diagnosis and staging?
- Do they agree with the current plan?
- If not, what exactly would they do differently, and why?
“Bring your pathology report, procedure notes, imaging reports, and a timeline of prior treatments. The best second opinions are built on details, not memory alone.”
The best specialists don't compete with your existing team. They add perspective. Sometimes the outcome of a second opinion is reassurance that your current plan is exactly right. That is valuable too.
Navigating Your Path Forward with Confidence
Bladder carcinoma in situ asks patients to do something difficult. It asks you to hold two truths at once. This is a serious, high-risk bladder cancer diagnosis. It is also one that can often be managed thoughtfully when the plan is precise and the follow-up is disciplined.
Across the United States, bladder cancer remains a major health issue. The American Cancer Society estimates 84,530 new U.S. cases in 2026, which is one reason understanding subtypes such as CIS matters so much when treatment planning begins (ACS estimate cited through SEER bladder cancer overview).
The practical challenge is rarely just learning the label. It's learning how to make decisions at each fork in the road. What did the biopsy really show? Is BCG working? If it isn't, are you trying to preserve the bladder, maximize cancer control, or balance both as carefully as possible?
What helps patients most
Clarity over speed
A fast decision isn't always the best decision. A clear decision usually is.Records you can understand
Ask for copies of pathology, procedure notes, and treatment summaries. If English isn't your first language, accurate interpretation matters. Problems in communication can affect safety, and this discussion of patient safety and medical translation explains why clear medical language is not a luxury.A team that clearly explains trade-offs
Good oncology care doesn't just present options. It helps you understand what each option protects, what it risks, and what life may look like afterward.
You do not need to master every detail of bladder pathology to advocate for yourself. You do need a working map. Know what your diagnosis means, know what treatment is trying to achieve, and know what result would change the next step. That is how patients regain a sense of control.
If you're facing a new bladder CIS diagnosis, deciding what to do after BCG, or weighing whether bladder preservation is still realistic, Hirschfeld Oncology offers consultations for patients who want a careful review of their case and a clear discussion of next-step treatment options.
.png)
.png)




