




.png)


Hearing the words “bone marrow transplant” can make the room go quiet.
For many people with lymphoma, that conversation happens after a relapse, after a scan that didn't bring the news they hoped for, or after treatment has become more complicated than they expected. Patients often tell me the same thing: they hear the word transplant and immediately picture major surgery, months in a hospital bed, or a last-resort treatment. That's understandable, but it's not the full picture.
A bone marrow transplant for lymphoma is better understood as a treatment strategy. It's one important option among several. For some people, it offers a real chance at deeper remission. For others, a different path such as CAR-T cell therapy, targeted treatment, or a less intensive plan may fit better with their disease, health, and goals. The right question usually isn't just “Can I get a transplant?” It's “Is this the best next move for me?”
Your Guide to Understanding a Lymphoma Transplant
If you're reading this, you may be the patient. Or you may be the person taking notes at appointments, trying to keep track of unfamiliar terms while also holding everyone together.
Either way, it helps to slow this down.
A bone marrow transplant for lymphoma is an established treatment that became a major milestone in the 1980s and 1990s, when doctors paired high-dose chemotherapy with stem cell rescue to help the body recover after marrow damage. In selected lymphoma settings, that approach changed outcomes and remains part of standard care today. It isn't used for every patient, and it isn't always the next step. But it still matters.
What people often get wrong
Many patients assume the transplant itself is the treatment that kills lymphoma. In reality, the intensive cancer treatment usually comes first. The stem cells are then given back to restore blood production after that treatment has wiped out the marrow's ability to do its job.
That distinction matters because it explains why doctors spend so much time talking about fitness, organ function, infection risk, and recovery support. This isn't just about whether a treatment can work against lymphoma. It's also about whether your body can safely get through it.
A transplant discussion isn't only about the cancer. It's also about your reserve, your recovery, and what trade-offs you're willing to make.
What you need to understand before deciding
Most families do better with transplant decisions when they break them into a few practical questions:
- What is the goal: Are doctors aiming for durable remission, disease control, or a bridge to another therapy?
- Why now: Is this being considered after relapse, after incomplete response, or because your lymphoma type behaves aggressively?
- Which kind: Are they recommending your own stem cells or donor cells, and why?
- What will life look like: How much hospital time, caregiver support, and recovery time should you plan for?
- What are the alternatives: If transplant isn't ideal, what other treatments are reasonable?
When you understand those five things, the conversation becomes much less frightening and much more useful.
What Is a Stem Cell Transplant for Lymphoma
A stem cell transplant for lymphoma is not a surgery where doctors remove bad marrow and put new marrow in its place. That image confuses a lot of people.
The simplest way to think about it is a garden. First, doctors use very strong treatment to clear out the weeds. Then they re-seed the garden so healthy growth can return.
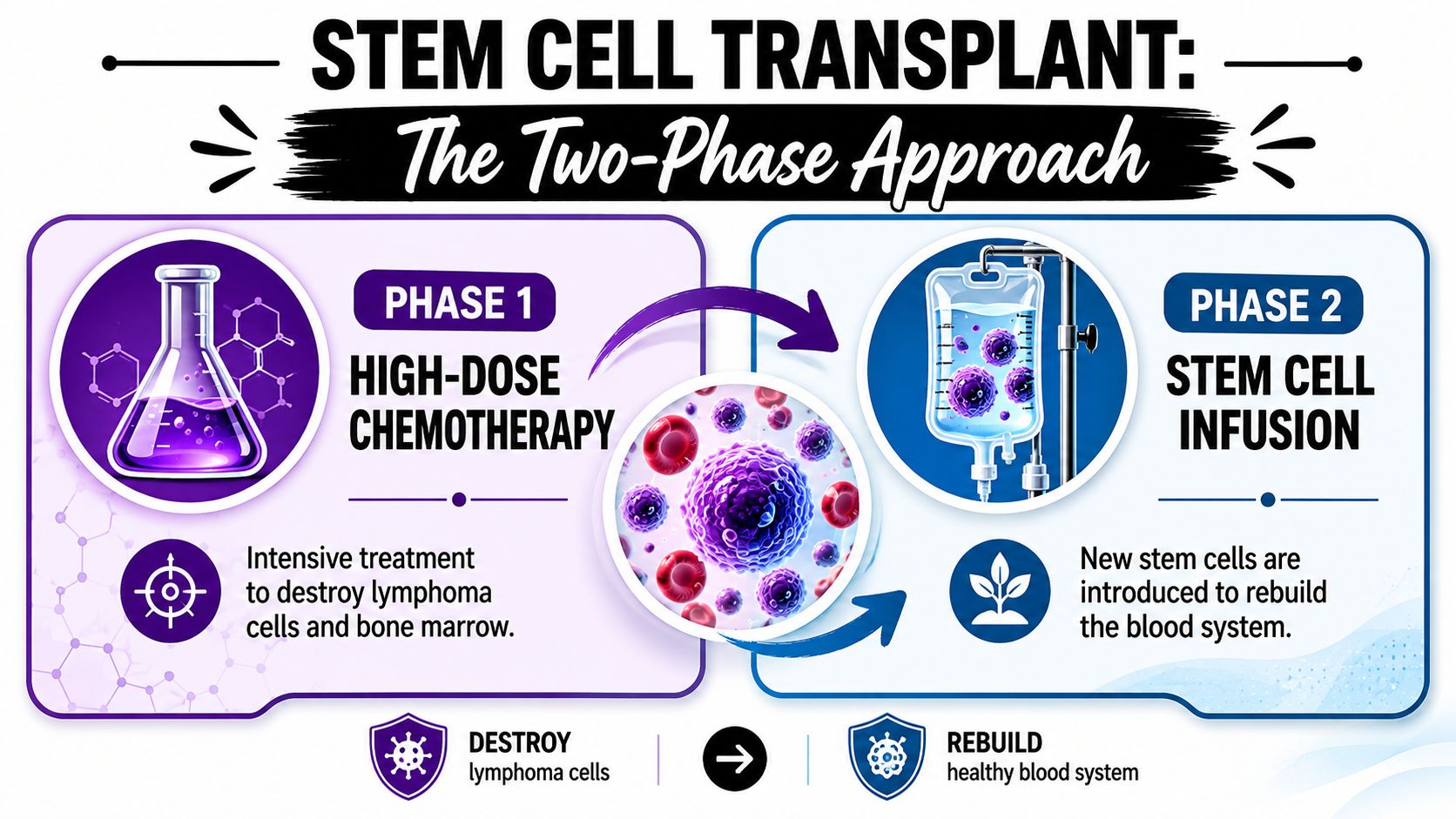
The two parts that matter most
The main treatment is the high-dose chemotherapy, and sometimes radiation, given during the conditioning phase. That treatment is designed to destroy remaining lymphoma cells. The problem is that it also severely damages the bone marrow.
After that comes the stem cell infusion. These stem cells are given through an IV. They travel back to the marrow and restart blood-cell production. A major cancer center describes this as a high-dose treatment platform followed by a rescue with reinfused stem cells to restore blood production in lymphoma care (Fox Chase explanation of stem cell transplant for lymphoma).
So when your doctor says “transplant,” they're often talking about this whole sequence:
- Collect stem cells or identify a donor
- Give intensive conditioning treatment
- Infuse stem cells
- Wait for marrow recovery
Autologous and allogeneic mean whose cells are used
These are the two terms that usually make people stop the conversation and ask for a repeat.
| Type | What it means | Why it may be used in lymphoma |
|---|---|---|
| Autologous transplant | Your own stem cells are collected and later returned to you | Common in relapsed lymphoma because it avoids donor matching and donor immune complications |
| Allogeneic transplant | Stem cells come from a donor | Used more selectively when doctors want donor cells to restore marrow function, but it brings added risks such as graft-versus-host disease |
Autologous transplant is often used in lymphoma because it lets doctors give high-dose treatment without needing to find a donor. Allogeneic transplant can be powerful in selected situations, but it adds another layer of complexity.
If you want a plain-language breakdown of the differences, this guide on allogeneic vs autologous transplant can help you sort through the terms before your next visit.
What transplant day is actually like
Many people expect an operation.
It's usually much quieter than that. The stem cells are commonly infused through an IV, more like a transfusion than a surgery. The dramatic part of transplant is not the infusion itself. It's the conditioning before it and the recovery after it.
Practical rule: When judging how hard transplant will be, focus less on “the day of transplant” and more on the weeks around it.
That shift in understanding helps families ask better questions and prepares them for the journey.
Is a Transplant the Right Path for You
Not every person with lymphoma should have a transplant. That isn't a sign that care is being withheld. It means treatment is being matched to the situation.

Doctors weigh the disease first
One of the biggest misunderstandings is the idea that transplant is automatically the strongest choice, so it must also be the best one. In lymphoma, that's not how decisions work.
Randomized evidence found no overall survival benefit for adding autologous transplant upfront in aggressive non-Hodgkin lymphoma. In that study, at 53 months, 61% of transplant patients were progression-free versus 56% with standard chemotherapy, and 68% were alive versus 77% in controls, with no significant difference (randomized evidence on upfront autologous transplant in aggressive non-Hodgkin lymphoma).
That's why transplant is usually not treated as a universal early-line upgrade. It's used more selectively, often in relapse, refractory disease, or carefully chosen high-risk situations.
Timing matters as much as eligibility
A patient can be medically fit enough for transplant and still not be at the right point in their treatment course for it.
Doctors often look at questions like these:
- Has the lymphoma relapsed: Transplant is commonly discussed after disease returns.
- Is the lymphoma responding to treatment: Chemo-sensitive disease often behaves differently from disease that resists multiple lines of therapy.
- What subtype is this: Some lymphoma subtypes are approached differently because their biology and expected benefit from transplant differ.
- What options are available now: A plan that made sense several years ago may not be the one a team recommends today.
Your health and priorities count
This part can feel personal because it is.
Transplant teams look at organ function, blood counts, prior treatment effects, infection risk, and overall physical reserve. They also think about whether you have support at home, how far you live from the treatment center, and how much disruption the process may cause.
A patient who wants the most intensive approach may still decide against transplant if the likely recovery would take too much away from daily life. Another patient may accept a harder short-term course for a chance at longer disease control.
Some of the most important transplant decisions have nothing to do with courage. They have to do with fit.
A good recommendation should reflect both the biology of the lymphoma and the life of the person living with it.
The Transplant Timeline A Step-by-Step Guide
Most families feel less anxious when the process becomes concrete. The transplant journey has a rhythm. Once you know the sequence, it's easier to prepare.
A bone marrow transplant for lymphoma became a major treatment milestone in the 1980s and 1990s. One major comparison reported 5-year overall survival of 53% with transplant versus 32% with standard treatment for certain lymphomas (historical review of transplant outcomes in lymphoma). That history is part of why transplant remains a standard option in selected cases.
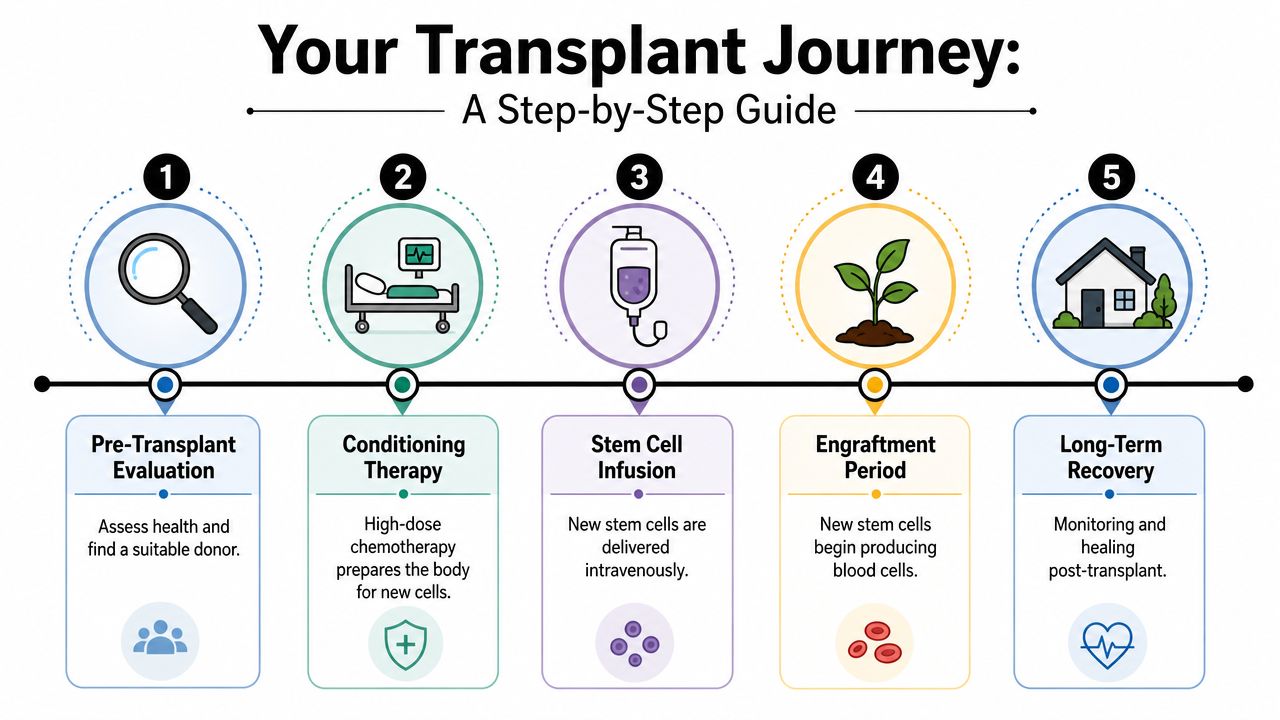
Step 1 Evaluation and testing
The first phase often feels like more appointments than treatment. You may have blood work, scans, heart testing, lung testing, and visits with transplant specialists.
This stage answers practical questions. Is your body strong enough for conditioning? Is the lymphoma under enough control to proceed? If an allogeneic transplant is being discussed, can a donor be identified?
Patients sometimes get frustrated here because it feels slow. But safety is constructed during this phase.
Step 2 Stem cell collection
If you're having an autologous transplant, your own stem cells are collected ahead of time and stored. Many people find this part less dramatic than they expected. It's a preparatory step, but it's an essential one.
If you're having an allogeneic transplant, this phase focuses on donor logistics rather than collecting your own cells.
A short video can help make the sequence less abstract.
Step 3 Conditioning treatment
This is the hardest part for many patients.
You receive high-dose chemotherapy, and in some plans radiation is added. The purpose is to kill remaining lymphoma cells and clear space for the new marrow recovery process. During this period, blood counts drop and the risk of infection rises sharply.
Common experiences can include fatigue, nausea, mouth soreness, appetite changes, and a sense that each day blends into the next. Families often expect a dramatic “transplant day,” but in reality conditioning is usually the more physically demanding stage.
Step 4 Transplant day
Transplant day is often emotionally loaded. People mark it on calendars and talk about it as if it were surgery day.
Medically, it's usually an IV infusion of stem cells. You're monitored closely, but the actual infusion may feel surprisingly uneventful. That can be reassuring. It can also feel strange, because so much preparation led to a day that seems quiet.
Step 5 Engraftment and early recovery
After the infusion, the work isn't done. This is the waiting period when the stem cells begin to settle in and restart blood production.
During this time, the care team watches closely for fever, infection, bleeding risk, dehydration, medication side effects, and signs that blood counts are beginning to recover. Families often describe this as the stretch that requires patience. Progress may come in small daily changes rather than a single turning point.
What going home usually means
Discharge doesn't mean you're “finished.” It means you're stable enough to continue recovery outside the hospital or with less intensive monitoring.
Expect:
- Frequent follow-up: Blood tests, medication adjustments, and symptom checks remain central.
- Infection precautions: Crowds, sick contacts, and food safety issues matter more than usual.
- Energy swings: Some days feel almost normal. Others don't.
- Help at home: Rides, meals, medication organization, and emotional support all matter.
The journey feels more manageable when patients know that transplant is not one event. It's a sequence with distinct phases, each with its own purpose.
Navigating Risks and Life After Transplant
A transplant conversation should include hope, but it also needs honesty.
The treatment is intensive because the period after conditioning leaves patients temporarily without normal marrow function. That creates vulnerability. Low blood counts, infection risk, bleeding risk, fatigue, and mouth or gut irritation are common concerns during early recovery. If you want a plain-language overview of one piece of that risk, this article on low white blood cell count during chemo explains why the infection window matters so much.
Short-term risks and how teams manage them
Doctors do not “watch and wait” for complications. Supportive care is built into transplant.
That can include protective infection measures, transfusion support, IV fluids, nutrition planning, symptom control, and close lab monitoring. Families often feel more grounded when they realize the transplant team expects these risks and has a plan for them.
The question is rarely whether transplant has risks. The real question is whether the likely benefits justify those risks in your specific case.
The allogeneic transplant issue families need explained clearly
If donor cells are used, there's an added concern called graft-versus-host disease, often shortened to GVHD. This happens when donor immune cells recognize the patient's tissues as foreign and attack them.
That possibility is one reason allogeneic transplant is reserved for selected cases rather than used casually. It can be an important treatment option, but it comes with a different risk profile than an autologous transplant.
Recovery is medical and emotional
One major center advises patients to expect about one month of recovery for an autologous transplant and about three months for an allogeneic transplant (NYU Langone guidance on transplant recovery time). Those time frames are useful for planning, but they aren't the whole story.
Recovery also includes:
- Rebuilding stamina: Walking across the room may feel different before it feels normal.
- Adjusting expectations: Many patients underestimate how uneven recovery can be.
- Returning to work carefully: Some people return in stages rather than all at once.
- Coping emotionally: Relief, fear of relapse, gratitude, irritability, and sadness can all show up in the same week.
Population outcomes can help doctors estimate benefit, but they don't predict exactly how one person will do. Your lymphoma subtype, prior treatment response, overall health, and transplant type all shape the road ahead.
Exploring Alternatives Transplant CAR-T and Beyond
Transplant is no longer the only major escalation option for relapsed lymphoma. That's one of the most important changes patients should understand.
Registry data show that treatment patterns are shifting. For diffuse large B-cell lymphoma, autologous stem cell transplants fell from 2,385 in 2019 to 1,548 in 2022, while CAR T-cell therapy rose from 537 to 809 over the same period (Cancer Today report on declining transplant use and rising CAR-T use in DLBCL). That doesn't mean transplant has become obsolete. It means doctors now have more than one serious option in some settings.
How the choices differ in practice
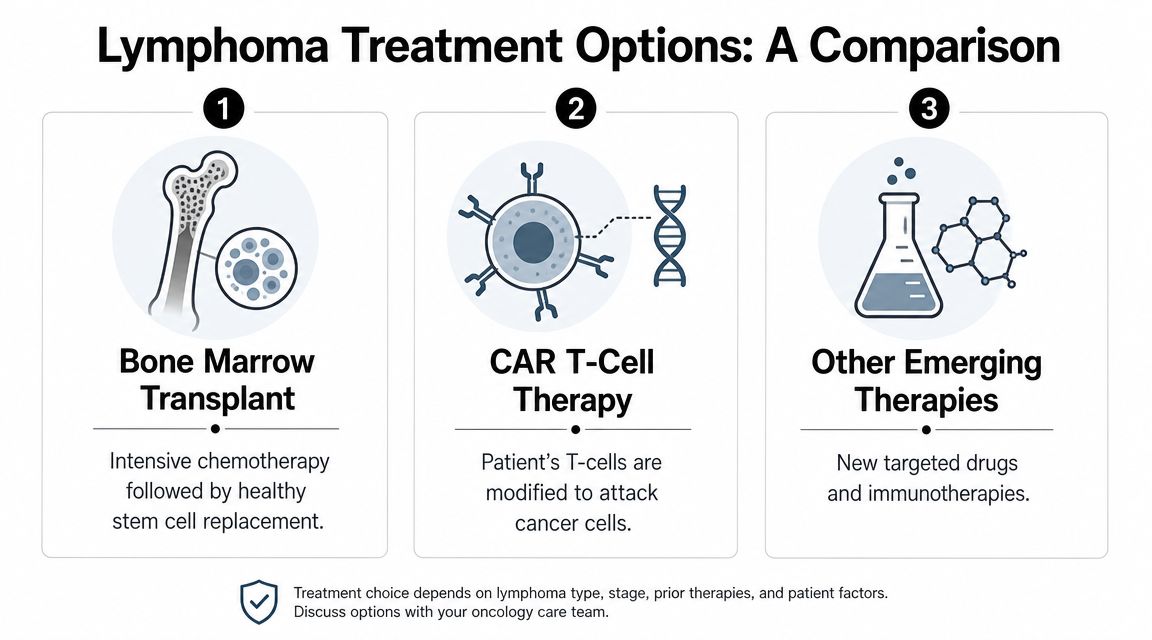
Autologous transplant and CAR-T can both be used in relapsed or refractory lymphoma, but they aren't interchangeable in every patient.
Transplant relies on high-dose chemotherapy followed by stem cell rescue. CAR-T uses a patient's T cells, which are modified to recognize and attack cancer cells. One approach leans on treatment intensity and marrow recovery. The other leans on engineered immune attack.
Transplant vs. CAR-T Therapy A Quick Comparison
| Feature | Autologous Stem Cell Transplant | CAR-T Cell Therapy |
|---|---|---|
| Core idea | High-dose chemotherapy followed by reinfusion of the patient's stem cells | Patient's T cells are modified to attack lymphoma cells |
| Typical role | Often considered in selected relapsed lymphoma | Increasingly used in some relapsed or refractory aggressive B-cell lymphomas |
| Main challenge | Infection risk and recovery after marrow suppression | Immune-related toxicities and close monitoring needs |
| Logistical burden | Intensive recovery period and strong support needs | Complex coordination, specialized centers, and monitoring after infusion |
| Best fit | Depends on disease sensitivity, fitness, and goals | Depends on subtype, prior treatment, eligibility, and access |
Other options may also matter
Some patients are not ideal candidates for either transplant or CAR-T. Others may prefer a lower-intensity strategy because of age, prior toxicities, or personal priorities.
In those situations, doctors may discuss:
- Targeted therapies: These can be useful when the lymphoma has a targetable feature or when a less intensive option is needed.
- Antibody-based treatment: Some immunotherapy approaches may fit patients who want to avoid a transplant pathway.
- Clinical trials: Trials can open access to emerging strategies when standard pathways are less appealing.
- Continued disease control treatment: In some cases, controlling lymphoma with an outpatient approach may better match a patient's goals.
If you're trying to place transplant in the bigger picture, this article on whether stem cells can cure cancer can help frame what transplant can and can't do.
The most important idea is simple: a recommendation should fit both the cancer and the person. A patient who values the most aggressive path may choose differently from a patient who prioritizes lower toxicity, outpatient care, or preserving day-to-day function.
Preparing for Your Journey and How We Can Help
The week before a transplant consult often feels like a pile of decisions all at once. One family member is asking about time off work. Another is wondering who can drive to appointments. The patient is trying to answer a harder question: which treatment path gives me the best chance of reaching my goals, and what will daily life look like if I choose it?
A good visit can turn that fog into a plan.
One of the simplest ways to do that is to bring a written list of questions. It helps you slow the conversation down, compare options clearly, and leave with fewer gaps in understanding. If transplant is being discussed alongside CAR-T or another treatment, that list also keeps the focus where it belongs: your disease, your health, and your priorities.
Questions worth bringing to your next visit
- Why are you recommending this option now: Ask why the team is suggesting transplant, CAR-T, or another treatment at this point in your care.
- What is the main goal of this treatment: You want to know whether the aim is a long remission, control of the lymphoma, symptom relief, or getting you to another therapy later.
- If transplant is part of the plan, what kind is it: Autologous and allogeneic transplants involve different risks, recovery patterns, and reasons for choosing them.
- How will this affect my day-to-day life: Ask about time in the hospital, clinic visits, fatigue, infection precautions, and when you may be able to return to work or family routines.
- What support will I need at home: Caregiver help, rides, medication organization, and meal preparation matter more than many families expect at the start.
- If transplant is not the best fit for me, what are the strongest alternatives: This question often leads to a better decision because it places transplant in context rather than treating it as the only serious option.
- What problems should lead to an urgent call: Fever, dehydration, trouble taking medicines, or sudden weakness are easier to handle when the plan is clear before treatment starts.
Practical preparation outside the clinic
Preparation is not only medical. It is also logistical and emotional.
Many families do better when they set up the basics early: a ride schedule, a clean place to rest, a simple medication system, and a short list of easy foods. During treatment, even small choices can feel tiring. Some patients find it helpful to save a few healthy meal options for cancer so meals require less thought on low-energy days.
It also helps to name your personal goals out loud. Some patients are willing to accept a harder recovery for the best chance at longer disease control. Others place more weight on staying outpatient, limiting time in the hospital, or protecting day-to-day function. Neither approach is wrong. Your oncology team can guide you best when they understand what matters most to you.
For patients in New York City who want help sorting through a complicated lymphoma decision, Hirschfeld Oncology offers consultation and infusion-based cancer care with an individualized approach to treatment planning, symptom management, and shared decision-making. For one patient, that may mean reviewing whether transplant fits the biology of the lymphoma and the realities of recovery. For another, it may mean comparing transplant with immunotherapy, targeted treatment, CAR-T, or a lower-intensity plan that better matches personal goals.
The best plan is one you understand, one you can realistically get through, and one that fits the life you are trying to protect.
If you're facing a difficult lymphoma decision and want a careful review of your options, Hirschfeld Oncology can help you weigh transplant, immunotherapy, and other treatment paths in the context of your goals, overall health, and day-to-day life.
.png)
.png)




