




.png)


The waiting room is often the hardest part.
You check your phone, glance at the IV chair, and wonder what your body will feel like in a few hours, tomorrow morning, or next week. Many people come to their first infusion expecting one simple answer to a complicated question: “What side effects will I get?” The honest answer is that cancer infusion side effects depend on the treatment, the timing, and how your own body responds.
That uncertainty is stressful, but it doesn't have to leave you powerless. Side effects aren't random chaos. They usually follow patterns. Some happen while the drug is entering your vein. Others show up days later. Some are uncomfortable but manageable at home. Others are warning signs that need immediate attention.
If you're preparing for treatment at an outpatient center, it helps to know what the process looks like in a real clinic setting, including how a local cancer infusion center supports patients through treatment. The more familiar the process feels, the less every sensation has to become a mystery.
Your Infusion Journey and What to Expect
A first infusion visit usually begins with questions, not medication. Nurses ask how you've been feeling, review your medications, check vital signs, and confirm the treatment plan. That can feel repetitive when you're tired or anxious, but each step is there to catch problems early.
Think of infusion treatment as a guided trip, not a single event. The medicine is one part. The other part is monitoring. Your team watches for signs that your body is tolerating the treatment well, and they make adjustments when it isn't.
What patients often worry about first
Most new patients worry about the dramatic things they've heard from friends, family, or social media. They wonder if they'll have an allergic reaction in the chair, whether they'll be sick for days, or if treatment will make normal life impossible.
Those fears are understandable. But most side effects become less frightening once you know three things:
- Which treatment you're receiving: Chemotherapy, immunotherapy, and targeted therapy cause different patterns of side effects.
- When symptoms tend to appear: Some reactions happen fast. Others are delayed.
- What deserves a same-day call: Not every symptom is dangerous, but some require immediate action.
Cancer treatment feels less overwhelming when you stop treating every symptom as a surprise and start seeing it as information.
What your care team is really doing
During infusion, nurses aren't just “checking in.” They're watching for changes in breathing, blood pressure, skin, pain, and behavior. After infusion, your oncologist and nursing team rely on your reports to complete the picture.
That partnership matters. If you know what to watch for, you can report changes early, before a manageable issue becomes a crisis. That's the heart of good side effect management.
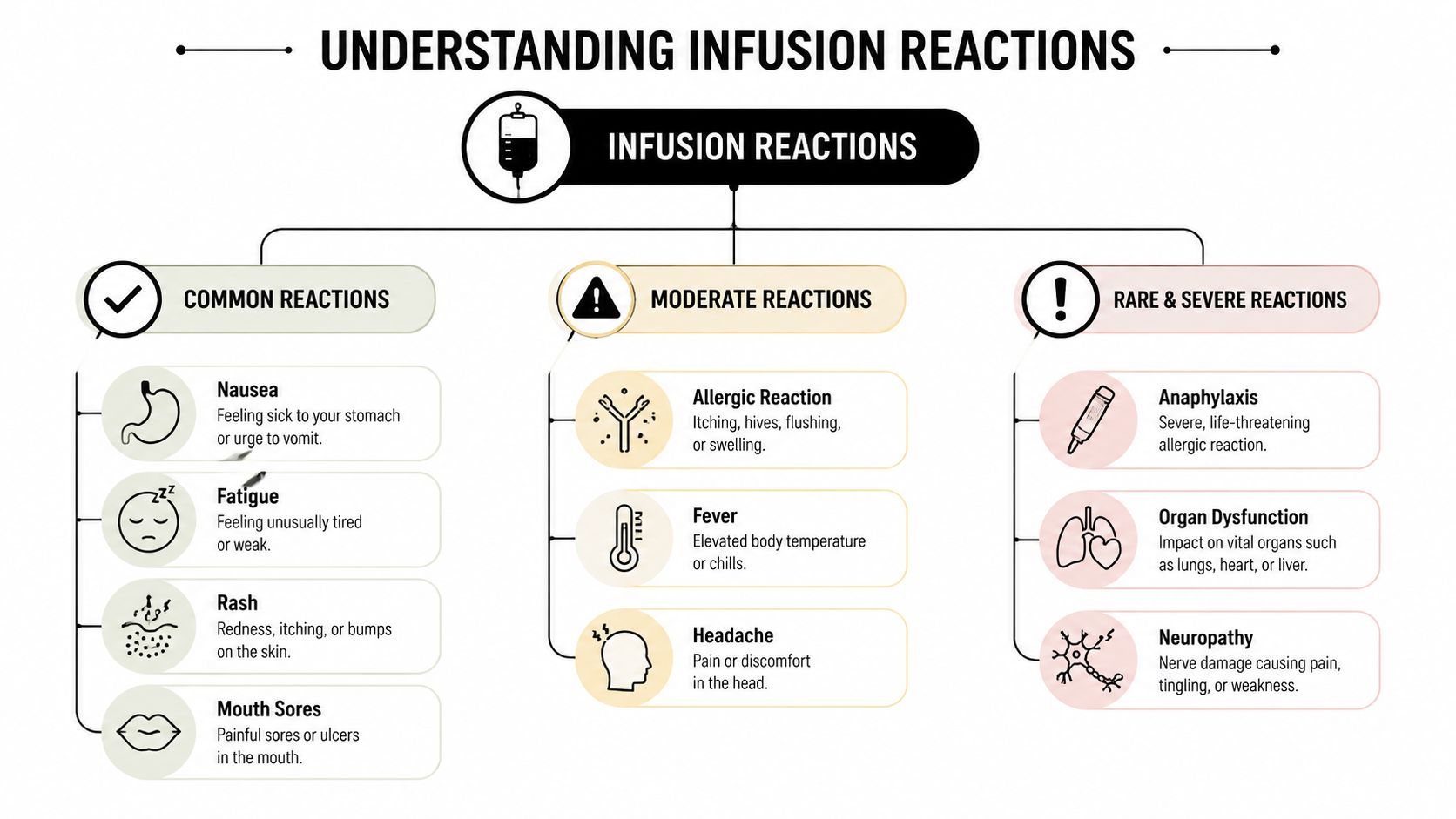
Understanding Infusion Reactions from Common to Rare
Not all side effects are the same kind of event. Patients often use one phrase, “I had a reaction,” to describe very different experiences. In practice, it helps to separate immediate infusion reactions from systemic side effects that unfold after the medicine starts working through the body.
A useful analogy is a building alarm system. Some problems are like the fire alarm going off the moment smoke is detected. They happen quickly and get everyone's attention. Other effects are more like what happens after the firefighters move through the building. There's disruption, cleanup, and lingering consequences that take time to notice.
Immediate reactions in the infusion chair
These are the reactions people usually imagine first. They may involve flushing, itching, chills, shortness of breath, dizziness, swelling, or a sudden change in how you feel during the infusion itself.
When this happens, the nurse may slow the infusion, stop it temporarily, give medications, or monitor you more closely. An immediate reaction doesn't always mean you can never receive that treatment again. Sometimes it means the team needs a different infusion rate, premedication plan, or monitoring approach.
Side effects that show up later
Other cancer infusion side effects don't look like an “allergic” event at all. They may include fatigue, nausea, mouth soreness, rash, bowel changes, brain fog, or low blood counts. These symptoms can begin after you've already gone home.
That delayed pattern confuses many patients. They think, “I felt fine at the clinic, so why do I feel awful now?” The answer is that many drugs don't cause problems at the moment they enter the vein. They cause changes later, as they affect cancer cells, the immune system, or healthy fast-growing cells.
A practical way to sort symptoms
Use three buckets when you think about symptoms:
| Category | What it usually means | Examples |
|---|---|---|
| Common | Expected, often manageable, still worth reporting | Nausea, fatigue, mild rash, mouth sores |
| Moderate | Needs prompt guidance from your team | Fever, worsening headache, stronger rash, persistent vomiting |
| Rare or severe | Needs urgent medical attention | Trouble breathing, chest symptoms, severe allergic reaction, signs of organ inflammation |
Practical rule: A symptom may be common and still deserve treatment. You do not need to “wait until it gets bad” to mention it.
That matters because many side effects start small. Early action is often what keeps them from becoming severe.
The Timeline of Side Effects Acute vs Delayed
One of the most important questions in oncology is simple: When did the symptom start? Timing helps your team decide whether a symptom is likely related to the infusion, the cancer itself, an infection, another medication, or something unrelated.
Many patients expect side effects to happen right away. Some do. Many don't.
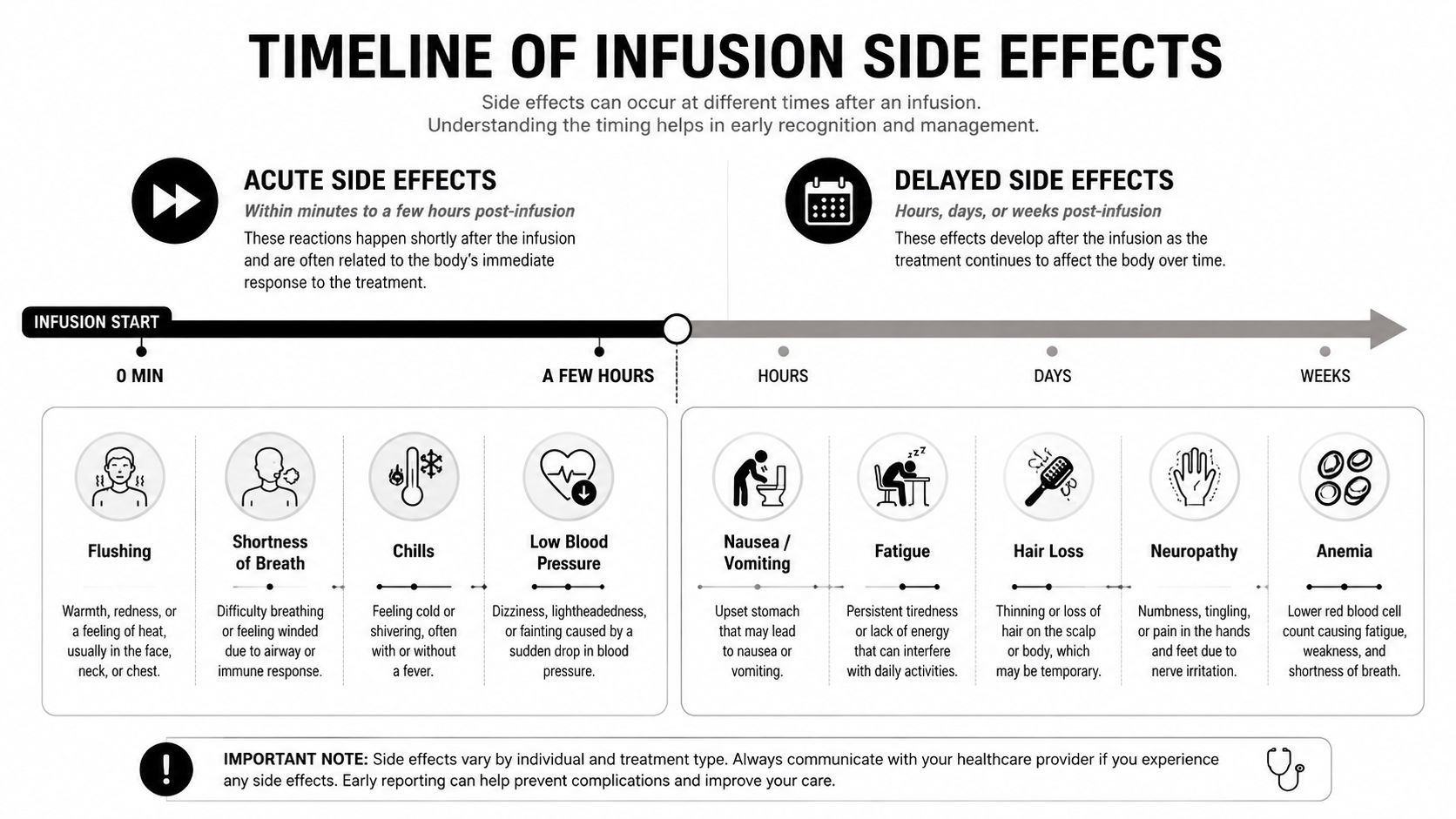
Acute side effects
Acute side effects happen during the infusion or soon after. These are the symptoms that can begin within minutes or hours. They may include flushing, chills, lightheadedness, shortness of breath, or blood pressure changes.
These symptoms tend to come from the body reacting to the medication as it enters the bloodstream. That's why the infusion unit monitors you closely while treatment is running. The goal is speed. If a reaction starts, the team can respond immediately.
Delayed side effects
Delayed side effects often appear later the same day, the next day, or several days afterward. Some take even longer. Fatigue may creep in gradually. Mouth sores may show up after the tissues lining the mouth become irritated. Numbness or tingling can build with repeated treatment over time.
This delay has a biological reason. Different tissues in the body react on different schedules. Some cells turn over quickly. Others show stress only after repeated exposure. Your symptoms often reflect that internal clock.
Why delayed symptoms feel so unpredictable
Patients often say delayed side effects feel “sneaky.” That's a good description. You may leave treatment feeling normal and then wake up feeling different.
A simple way to think about it:
- Fast reactions usually come from the body sensing the drug immediately.
- Short-delay effects often come from irritation of sensitive tissues such as the stomach, bowel, or mouth.
- Longer-delay effects may reflect changes in blood counts, nerve irritation, immune activation, or cumulative stress on the body.
What to track at home
If you keep a simple symptom log, note these details:
- When it began: During infusion, that evening, two days later, or longer.
- How it changed: Better, worse, or coming in waves.
- What else was happening: New medicines, poor sleep, reduced eating, or dehydration.
- How it affects function: Can you eat, walk safely, think clearly, or do your normal tasks?
The timing of a symptom is often as important as the symptom itself.
That's why your team asks so many timeline questions. They're not being repetitive. They're building the pattern that guides treatment decisions.
How Side Effects Differ by Treatment Type
A lot of confusion comes from articles that group all cancer infusion side effects together. That blurs the biggest point. Different treatments cause different side effects because they work in different ways.
Chemotherapy attacks rapidly dividing cells. Immunotherapy activates the immune system. Targeted therapy interferes with specific signals or proteins that cancer cells depend on. If the mechanism is different, the side effect pattern will be different too.
For a deeper patient-friendly overview of those treatment differences, Hirschfeld Oncology has a helpful explainer on the difference between immunotherapy and chemotherapy.
Chemotherapy and fast-growing healthy cells
Chemotherapy is often the easiest to explain with an analogy. It acts like a weed killer that targets fast growth, but it can't perfectly distinguish between weeds and every healthy fast-growing plant nearby.
That's why chemotherapy commonly affects bone marrow, hair follicles, the digestive tract, and the lining of the mouth. One major effect is myelosuppression, meaning the bone marrow makes fewer blood cells. According to the NCBI review of chemotherapy-related myelosuppression, blood counts often reach their lowest point 7–14 days post-infusion, and up to 30% of patients receiving standard-dose anthracycline or taxane regimens experience Grade 3–4 neutropenia. The same review defines febrile neutropenia as a temperature of ≥100.5°F (38°C) with a neutrophil count <1,500/mm³, a combination that requires immediate hospitalization and broad-spectrum antibiotics.
Immunotherapy and the overactive immune system
Immunotherapy can feel less intuitive because it does not poison fast-growing cells. Checkpoint inhibitors remove some of the immune system's brakes. That can help T cells attack cancer more effectively, but it can also break normal self-tolerance.
The result can be immune-mediated adverse events, often shortened to irAEs. These are inflammatory side effects caused by the immune system attacking healthy organs. The Hirschfeld Oncology review of side effect management in cancer care notes that clinically significant irAEs include colitis, pneumonitis, and myocarditis. It also reports that severe Grade 3–4 irAEs range from 10% to 20%, while myocarditis is less than 1% but can be highly fatal if not recognized within 48 hours of infusion onset, which is why rapid evaluation and close cardiac monitoring matter.
Targeted therapy and pathway-specific effects
Targeted therapy sits between these worlds. It aims at specific molecular pathways rather than broadly attacking all rapidly dividing cells or globally activating immunity.
That selectivity can reduce some classic chemotherapy problems, but it creates its own pattern. Patients often see treatment-specific effects such as rash, bowel changes, or blood pressure issues, depending on the pathway being blocked. In plain terms, the side effects often mirror the normal jobs of the pathway the drug is interfering with.
Common side effect profiles by treatment type
| Treatment Type | Mechanism of Action | Common Side Effect Examples |
|---|---|---|
| Chemotherapy | Damages rapidly dividing cells, including some healthy ones | Low blood counts, nausea, mouth sores, fatigue |
| Immunotherapy | Releases immune brakes so T cells attack cancer more strongly | Inflammatory side effects involving bowel, lungs, skin, or heart |
| Targeted therapy | Blocks specific signals or proteins tied to cancer growth | Rash, diarrhea, treatment-specific organ or skin effects |
What matters most is this. If you know which treatment family you're receiving, many side effects stop feeling random. They start making medical sense.
Proactive Management Before During and After Your Infusion
Good side effect management starts before the IV ever begins. The safest infusion experience usually comes from preparation, close observation, and clear follow-up, not from reacting at the last minute.

Before infusion
Before treatment, ask your team what medications you'll receive before the infusion and why. Premedications may include drugs to reduce nausea or lower the chance of a reaction. If you know what each medicine is for, the day feels less confusing and you're more likely to recognize when something feels different than expected.
Medication review matters more than many patients realize. A complete and up-to-date list helps clinicians catch duplicate drugs, interactions, and changes made by outside specialists. For practices trying to tighten that process, structured tools for medication reconciliation for practices can support safer handoffs and clearer records, which is especially important when patients see multiple doctors.
Bring a written list that includes prescriptions, supplements, over-the-counter medicines, and anything you take “only sometimes.” That list can affect what supportive medications are safe to use.
During infusion
During treatment, speak up early. Don't wait to see whether a new symptom passes on its own if you're having chest discomfort, itching, flushing, dizziness, throat tightness, or sudden shortness of breath.
Nurses can do a lot in real time. They can pause the infusion, slow the rate, check vital signs, notify the oncologist, and give rescue medications if needed. Most infusion units are built around that rapid-response workflow.
A helpful patient habit is to describe symptoms plainly rather than trying to diagnose them. “My chest feels tight” is more useful than “I think I'm anxious,” if what you feel is a change in breathing or pressure.
After infusion
After you go home, the goal shifts from observation to pattern recognition. Keep fluids nearby. Eat small, tolerable meals if your stomach is unsettled. If your mouth becomes sore, choose softer foods and avoid sharp, acidic, or highly seasoned items that scrape irritated tissue.
Fatigue usually responds best to pacing, not to forcing yourself through a full normal schedule. Many people do better when they break tasks into smaller pieces, rest before they're depleted, and accept help earlier.
If you're on chemotherapy, be especially alert for fever during the period when blood counts may drop. The NCBI review cited earlier explains that the low point in blood counts often occurs 7–14 days after infusion, and that low neutrophils can lead to febrile neutropenia. Some patients receive G-CSF to reduce that risk, especially when the regimen is known to suppress the bone marrow significantly.
A simple after-care checklist
- Track symptoms daily: Write down start time, severity, and what made it better or worse.
- Watch for infection clues: Fever, shaking chills, or feeling suddenly unwell deserve urgent attention.
- Protect your energy: Spread errands and chores out instead of stacking them on one “good day.”
- Keep rescue medications ready: Anti-nausea drugs don't help if they're still at the pharmacy when symptoms start.
Small symptoms reported early are easier to manage than severe symptoms explained later.
If you want a broader practical framework for home monitoring and supportive care, Hirschfeld Oncology also offers guidelines for managing side effects during cancer treatment.
The Hirschfeld Oncology Approach to Minimizing Toxicity
Some clinics treat side effects as an unavoidable cost of cancer treatment. A better approach is to treat them as a major part of the treatment plan itself.
That's the philosophy many patients look for when they're dealing with advanced cancer, prior treatment toxicity, or fear that they won't tolerate standard regimens well. A patient-centered practice asks two questions at once: What gives the cancer the best chance of control, and what gives the patient the best chance of living through treatment with function and dignity intact?
What a lower-toxicity model looks like
Hirschfeld Oncology describes a care model built around low-dose chemotherapy, personalized immunotherapy, targeted therapy, close monitoring, and individualized symptom management. That matters because toxicity isn't only about dramatic complications. It's also about whether a patient can keep eating, walking, thinking clearly, sleeping, and staying out of the hospital whenever possible.
Why support changes outcomes patients can feel
A high-support model doesn't promise zero side effects. No honest oncologist would promise that. What it can do is reduce avoidable suffering by matching treatment intensity, supportive care, and follow-up to the individual patient rather than using a one-size-fits-all script.
For patients with treatment-resistant or metastatic disease, that kind of personalization can be the difference between “I had therapy” and “I was supported through therapy.”
FAQ on Cancer Infusion Side Effects
Which symptoms mean I should call right away or seek urgent care
Call your team immediately or seek urgent care for trouble breathing, chest pain, severe diarrhea, major weakness, confusion, a high fever, shaking chills, or any symptom that feels suddenly intense or unsafe.
If you're receiving chemotherapy, fever deserves special respect because of the risk of neutropenia discussed earlier. If you're receiving immunotherapy, new bowel, lung, or heart symptoms can reflect immune-related inflammation and shouldn't be brushed off as “probably nothing.”
When in doubt, call. Oncology teams would rather hear about a false alarm than learn later that you waited through a serious complication.
Is chemo brain real, or am I just overwhelmed
It's real. And for many patients, it's one of the most frustrating cancer infusion side effects because other people often can't see it.
A review discussing this gap in patient guidance reports that 87% of patients experience fatigue and significant cognitive trouble and notes that resources often mention the symptom without explaining how to live with it day to day, especially for working adults and caregivers, as described in this review on cognitive impairment and fatigue in cancer care.
What helps in real life is practical compensation, not self-criticism:
- Use external memory tools: Keep one notebook, one phone note, or one calendar instead of several systems.
- Reduce safety risks: Don't multitask while cooking, managing medications, or driving if you feel mentally foggy.
- Chunk decisions: Make one decision at a time when possible. Fatigue and cognitive overload often travel together.
- Ask for repetition: It's appropriate to ask your team to repeat instructions, write them down, or include a caregiver on the call.
“I can think, but I can't think as quickly or hold as much at once.” That's how many patients describe chemo brain, and it's a useful way to explain it to family.
How do I tell my care team about side effects without sounding like I'm complaining
Try to report symptoms like a clinician would. Be specific and concrete.
You can say:
- “This started the night after infusion.”
- “It's happening every day, not just once.”
- “I can still eat, but only soft foods.”
- “I'm forgetting steps when I manage my medications.”
- “I'm not asking to stop treatment. I need help managing this safely.”
That last sentence is powerful. Many patients stay quiet because they worry reporting symptoms will make the team stop effective therapy. In reality, good reporting helps your team protect you and keep treatment on track whenever possible.
If you or a loved one is dealing with difficult cancer infusion side effects and wants a more individualized, lower-toxicity treatment strategy, Hirschfeld Oncology offers compassionate, research-informed care focused on symptom control, close monitoring, and treatment plans built around both effectiveness and quality of life.
.png)
.png)




