




.png)


You may be here because a blood test showed anemia, or because someone you love has been exhausted for weeks and no amount of rest seems to help. Maybe they look paler than usual. Maybe climbing stairs suddenly feels harder. These symptoms are common, and that's part of what makes them easy to brush off.
As an oncologist, I try to help families hold two ideas at the same time. First, anemia is common and often treatable. Second, anemia can be a clue. Sometimes it points to iron deficiency, vitamin deficiency, chronic illness, treatment side effects, or bleeding. Sometimes it is one of the early signs that pushes us to look for a hidden cancer.
That doesn't mean anemia equals cancer. It means anemia deserves an explanation.
Understanding Anemia as a Warning Sign
A familiar story goes like this. Someone has been tired for months, but life is busy. They blame work, stress, poor sleep, or getting older. Then they start feeling winded walking from the parking lot. Their primary doctor orders blood work and says, “You're anemic.”
That word can sound technical, but the basic idea is simple. Your red blood cells are the delivery trucks that carry oxygen. If you don't have enough of them, your muscles and organs get less oxygen than they need. That's why anemia can make you feel weak, foggy, lightheaded, short of breath, or unusually cold.

When anemia is more than “just low iron”
One of the biggest points of confusion is this: people hear “iron deficiency” and assume the answer must be diet alone. Sometimes that's true. Sometimes it isn't.
If you follow a plant-based diet and are sorting through symptoms that can overlap with nutrient issues, a practical overview of vegan vitamin deficiency symptoms can help you think through possibilities. But when anemia appears without a clear reason, especially in adults, doctors have to think more broadly.
A major reason we take unexplained iron-deficiency anemia seriously comes from a retrospective cohort study in which patients with iron-deficiency anemia had an overall cancer risk more than doubled compared with the general population, with a standardized incidence ratio of 2.15. The excess risk was especially notable in the first five years, and even after excluding cancers found early, the risk remained higher for pancreatic, kidney, liver, and bladder cancers, as described in this population-based analysis of iron-deficiency anemia and cancer risk.
Practical rule: If an adult develops unexplained iron-deficiency anemia, the right question isn't only “How do we raise the iron?” It's also “Why did the iron drop in the first place?”
The signal, not the diagnosis
Anemia is a warning sign, not a final diagnosis. It operates much like a check-engine light. The light doesn't tell you exactly what's wrong, but it tells you the car deserves a careful look before you keep driving.
That is especially true when anemia shows up with any of these features:
- Persistent fatigue: Tiredness that doesn't improve with sleep.
- Shortness of breath: Breathlessness during activities that used to feel easy.
- Pale skin or dizziness: Signs that oxygen delivery may be reduced.
- Unexplained weight loss or appetite changes: Clues that there may be something broader going on.
- Visible or hidden bleeding: Blood in stool, black stool, heavy vaginal bleeding, or lab signs suggesting blood loss.
The reassuring part is that once we understand the cause, we can usually make a much better plan. The key is not stopping at the word “anemia.”
How Cancer Can Cause Anemia
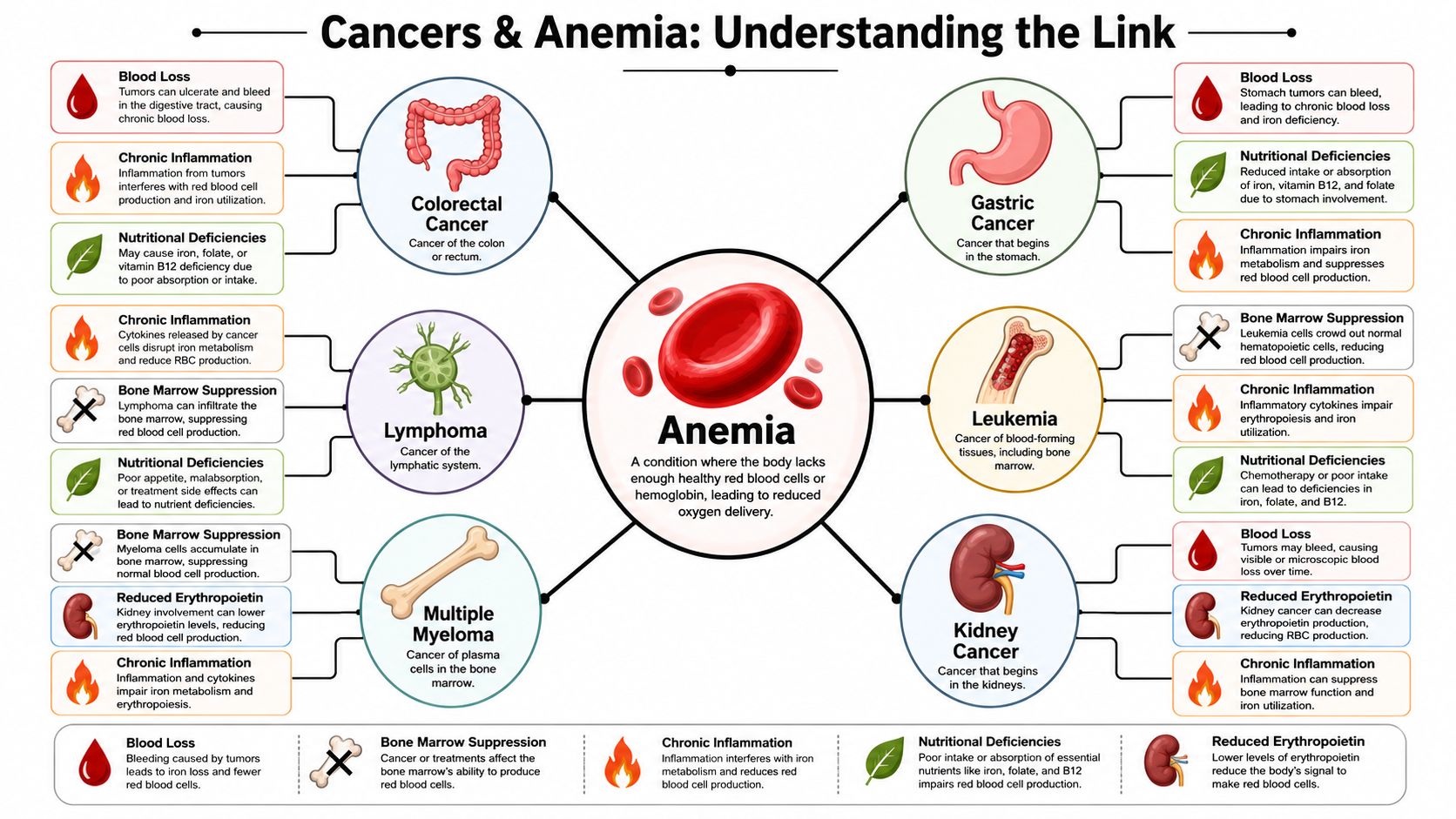
Cancer can lower red blood cell levels in more than one way. That's why two patients can both be anemic but need very different care. One may be losing blood slowly. Another may have bone marrow that can't keep up. A third may have inflammation that traps iron where the body can't use it well.
Four common pathways
Here are the main mechanisms behind cancers that cause anemia.
| Mechanism | Simple Explanation | Commonly Associated Cancers |
|---|---|---|
| Chronic blood loss | A slow leak from the body's plumbing. Small amounts of bleeding over time can drain iron stores. | Colorectal, stomach, cervical, ovarian, bladder |
| Bone marrow infiltration | The blood-making garden gets crowded out, so healthy red blood cells can't grow well. | Leukemia, lymphoma, multiple myeloma, myelodysplastic syndromes, metastatic cancers involving marrow |
| Inflammation-related anemia | The body acts like it's fighting a fire nonstop, and normal blood production gets disrupted. | Many advanced solid tumors and blood cancers |
| Nutritional deficiency or poor absorption | The body doesn't get or absorb the building blocks needed to make red blood cells. | Gastrointestinal cancers and cancers affecting appetite or digestion |
Blood loss can be hidden
Some cancers bleed in ways patients never see. A colon tumor, for example, may ooze small amounts of blood into the stool day after day. You may not notice red blood in the toilet, but over time the body loses iron faster than it can replace it.
That's why gastrointestinal cancers are so often part of the workup when someone has iron-deficiency anemia. The bleeding may be subtle, but the cumulative effect can be significant.
Bone marrow can be directly affected
The bone marrow is your blood cell factory. It makes red cells, white cells, and platelets. If cancer enters that factory, production slows or becomes abnormal.
Cancers that directly infiltrate or replace bone marrow, especially leukemia, lymphoma, multiple myeloma, and myelodysplastic syndromes, can cause anemia by suppressing erythropoiesis because red blood cells are produced in the marrow. Anemia is often an early presenting feature in these diseases, as explained by Cleveland Clinic's overview of anemia and cancer.
When bone marrow is involved, anemia isn't just a supply problem. It can be a factory problem.
Inflammation changes how the body uses iron
This is the part many families haven't heard about. A patient can have iron in the body and still struggle to use it properly. Cancer-related inflammation sends chemical signals that interfere with red blood cell production and iron handling.
A useful analogy is a pantry with food locked inside. The food exists, but the cook can't access it. In the same way, iron may be present in storage, yet unavailable where blood production needs it most.
Nutrition can also contribute
Some cancers reduce appetite. Others affect swallowing, digestion, or absorption. Treatment can add nausea, taste changes, or bowel changes. As a result, the body may become short on iron, folate, vitamin B12, or overall calories and protein needed for healthy blood production.
This is why an anemia workup shouldn't stop at a single lab value. The body is telling a story, and the details matter.
Specific Cancers That Often Cause Anemia
Some cancers are especially well known for causing anemia, but the reason differs by cancer type. That distinction matters because it shapes the tests doctors order and the treatments that help.
Gastrointestinal cancers
Colon and stomach cancers are classic examples because they often cause slow, ongoing bleeding. A patient may not see obvious blood, yet lab work shows iron deficiency and low hemoglobin.
In a study of patients with anemia, cancer was found in 5.6%, and among those cancer cases, colorectal cancer was the most frequently diagnosed malignancy at 22.5%, followed by advanced gastric cancer at 16.1%, according to the American Cancer Society discussion of anemia and cancer. If you're looking specifically at colorectal disease, this overview of colon cancer care gives more context on how these cancers are evaluated and treated.
Esophageal and other upper digestive cancers can create similar problems. Some lead to bleeding. Others make eating difficult, which adds nutritional strain on top of blood loss.
Blood and marrow cancers
Leukemia, lymphoma, multiple myeloma, and myelodysplastic syndromes belong in a different category. These are among the clearest cancers that cause anemia because they interfere directly with blood formation.
If the marrow is the factory floor, these cancers disrupt the workers, the machinery, or the space needed to produce healthy cells. Patients may develop anemia early, sometimes alongside frequent infections, bruising, bone pain, or abnormal white blood cell and platelet counts.
Gynecologic and urinary tract cancers
Cervical and ovarian cancers can contribute through abnormal bleeding, especially when symptoms have been dismissed as menstrual changes. Bladder cancer can do the same through blood loss in the urine, whether visible or microscopic.
This is one reason doctors ask detailed questions that may seem unrelated at first. Heavy periods, postmenopausal bleeding, darker stool, or pink urine can each point toward a different source of anemia.
Pancreatic, kidney, liver, and other advanced solid tumors
Not every cancer that causes anemia does so by obvious bleeding. Pancreatic, kidney, liver, and other advanced cancers often produce a more mixed picture. Inflammation, reduced appetite, impaired iron use, kidney effects, and treatment burden may all combine.
A cancer doesn't have to bleed to cause anemia. Some tumors change the body's chemistry enough to lower blood counts without any visible blood loss.
That's why a plain list of cancers only gets you part of the way. The more useful question is, how is this particular cancer causing anemia in this particular patient?
The Diagnostic Path from Symptom to Answer
Once anemia shows up on a lab test, the next step is to identify the pattern. Good diagnosis is less like guesswork and more like detective work. Each test answers a specific question.
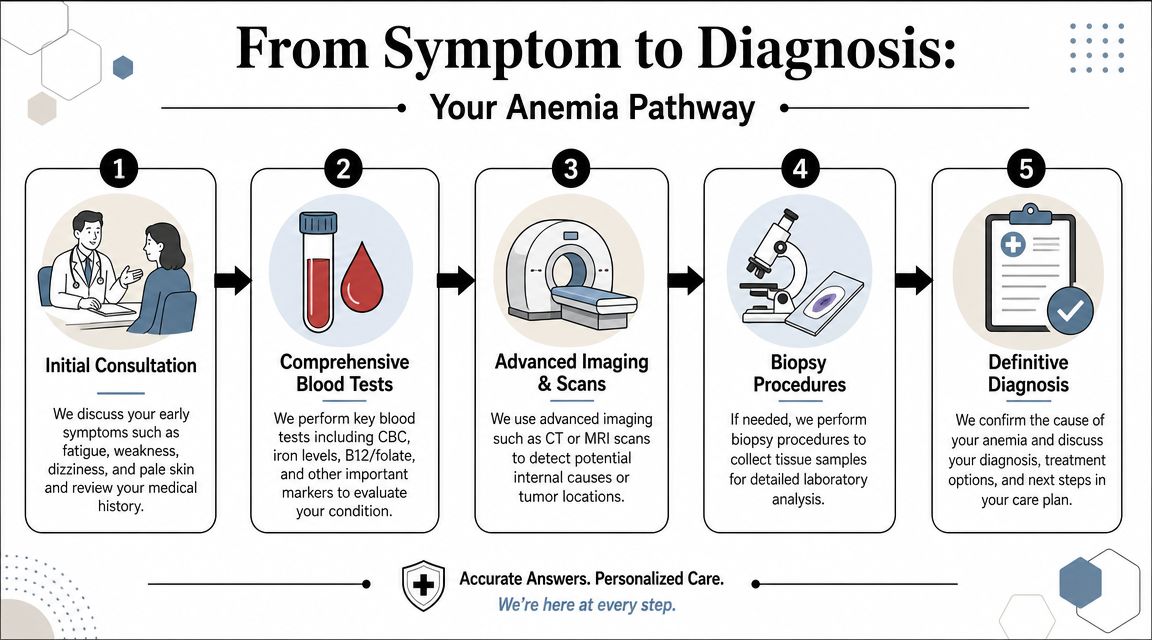
Start with the story
Doctors begin with symptoms and context. Fatigue matters, but so do shortness of breath, dizziness, black stools, appetite changes, weight loss, fevers, bone pain, or heavy menstrual bleeding. Age, medications, prior cancer history, kidney disease, and recent treatment all change the way we interpret the same blood test.
At this stage, specific details help more than general statements. “I get winded carrying groceries” is more useful than “I'm tired.”
Then read the blood work carefully
A complete blood count, or CBC, is like a headcount for the major blood cells. It shows whether red blood cells are low and whether white blood cells or platelets are also affected. That pattern can hint at whether the issue is blood loss, nutritional deficiency, marrow disease, inflammation, or treatment effect.
If you want a patient-friendly explanation of these measurements before your appointment, this guide to full blood count analysis is a useful primer.
Doctors often add tests such as:
- Iron studies: These help tell the difference between true iron deficiency and iron that is present but poorly available.
- Reticulocyte count: This shows whether the marrow is trying to respond by making young red cells.
- Vitamin levels: B12 and folate can matter, especially with poor intake or absorption.
- Kidney and liver tests: Organ function influences blood production and iron handling.
For a visual overview of how workups unfold, this short video can help:
When scans or procedures are needed
If iron deficiency suggests blood loss, the next step may be looking inside the gastrointestinal tract with endoscopy or colonoscopy. If the CBC shows multiple abnormal cell lines, or if blood cancers are suspected, doctors may recommend marrow testing.
A bone marrow biopsy procedure sounds intimidating, but it has a clear purpose. It lets the care team see whether the marrow is healthy, inflamed, infiltrated by cancer, or affected by a disorder such as myelodysplastic syndrome.
The most helpful test is the one that answers a focused question. Doctors aren't ordering everything at random. They're narrowing the possibilities step by step.
Diagnosis is about cause, not just confirmation
Families often ask, “How low is too low?” That matters, but the more important issue is why the anemia happened. A modest drop caused by hidden colon bleeding demands a different response than a similar drop caused by lymphoma in the marrow or by inflammation from advanced cancer.
That's why good evaluation feels layered. The blood count tells us there is a problem. The rest of the workup tells us what kind of problem it is.
Modern Approaches to Managing Cancer-Related Anemia
Treatment works best when it matches the mechanism. Older thinking often treated anemia as a simple shortage problem. If hemoglobin was low, the response was to transfuse, prescribe iron, or wait. Modern oncology takes a more precise approach.
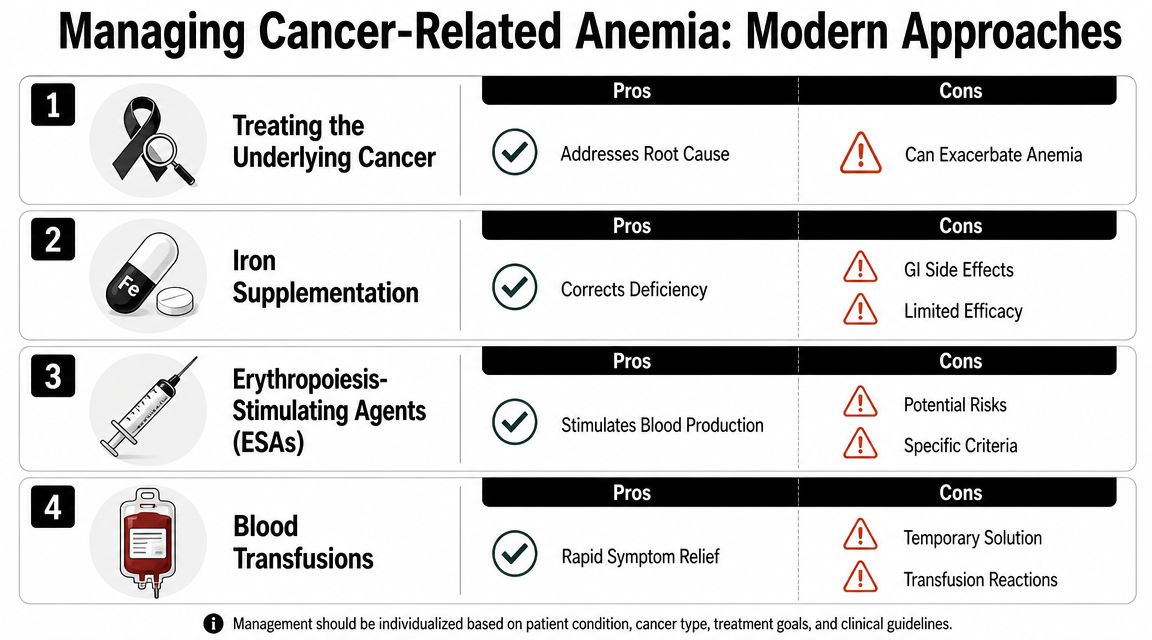
Treat the cause while relieving symptoms
The most durable fix is often control of the cancer itself. If a bleeding tumor is treated, blood loss may slow. If marrow disease improves, blood production may recover. If inflammation comes down, the body may use iron more effectively again.
But patients still need support in the meantime. Common options include:
- Blood transfusion: Helpful when symptoms are significant or anemia is severe and rapid relief is needed.
- Iron treatment: Oral iron may help in some settings, while intravenous iron can be considered when absorption is poor or when a quicker response is needed.
- Erythropoiesis-stimulating agents: These medications can help selected patients make more red blood cells, though they're not right for everyone.
- Nutritional support and symptom management: Addressing intake, nausea, and fatigue can make treatment more tolerable.
Why iron alone may not solve the problem
Modern care has changed most, notably with recent reviews describing cancer-related anemia as cytokine-mediated, with inflammation shortening red cell survival, suppressing erythroid precursors, and impairing iron use. That means a patient can be iron-restricted even with adequate iron stores, so the key question is not just whether they need iron, but why iron is unavailable, as outlined in this review on iron deficiency in cancer and cancer-related anemia.
In plain language, the body may be hoarding iron in storage while starving the bone marrow of usable iron. Giving more oral iron in that setting may not do very much. That's one reason patients sometimes say, “I've been taking iron and nothing's changing.”
A more nuanced treatment plan
A strong anemia plan usually asks several questions at once:
- Is the patient bleeding somewhere? If yes, that source needs attention.
- Is the marrow able to respond? If not, marrow disease, treatment effect, or infiltration may be involved.
- Is inflammation blocking iron use? If yes, iron strategy and cancer control both matter.
- Are treatment side effects adding to the problem? For many patients, that's part of the picture, especially with anemia from chemotherapy.
- What does the patient need right now? Fast symptom relief and long-term correction are not always the same thing.
Why specialist care matters
In such cases, a hematology-oncology team can add real value. The goal isn't to chase a single lab number. It's to identify the mix of blood loss, inflammation, iron restriction, marrow suppression, nutrition, and treatment effect that exists in front of you.
At Hirschfeld Oncology, Dr. Azriel Hirschfeld's medical oncology and hematology practice includes anemia and iron deficiency screening as part of broader cancer care. In practical terms, that means the team can evaluate whether a patient needs transfusion support, iron repletion, treatment adjustment, or a deeper search for the driver of the anemia.
Good anemia care is individualized. Two people with the same hemoglobin may need completely different treatment.
When to See a Specialist and How We Can Help
You should ask for specialist input when anemia is unexplained, keeps recurring, causes symptoms that interfere with daily life, or appears alongside signs that raise concern for cancer. Those signs can include unintended weight loss, bowel changes, dark stool, blood in the urine, swollen lymph nodes, bone pain, poor appetite, or a known cancer diagnosis with worsening fatigue.
Specialist care also makes sense when treatment hasn't helped. If someone has already tried iron but remains weak and short of breath, the problem may not be simple iron deficiency. It may be hidden bleeding, marrow involvement, inflammation-driven anemia, treatment effect, or a combination of several factors.
What patients and families should ask
A short list of questions can make appointments more productive:
- What type of anemia does this look like?
- Do the labs suggest blood loss, marrow suppression, or inflammation?
- Is more testing needed to look for a cancer or to understand a known cancer better?
- What will help fastest with symptoms, and what will address the cause?
- How will this affect treatment choices going forward?
Care should match the patient's goals
For patients with advanced or treatment-resistant cancers, anemia management is part of a bigger conversation. Some people need support to stay active enough for treatment. Others want symptom relief with the least disruption possible. Those priorities matter.
Hirschfeld Oncology serves patients in Brooklyn, including Williamsburg and Bushwick, with outpatient cancer care, infusion services, close monitoring, and treatment strategies designed to balance efficacy with tolerability. For families facing pancreatic, colorectal, gastric, breast, ovarian, bile duct, esophageal, and other complex cancers, that kind of coordinated care can make the path forward clearer.
If you or a loved one has anemia and no one has yet explained why, it's reasonable to push for answers. Anemia is often treatable. When it's connected to cancer, early recognition helps doctors choose better tests, better support, and better next steps.
If you need help making sense of anemia in the setting of cancer, Hirschfeld Oncology offers educational resources and access to consultation for patients and families navigating complex diagnoses and treatment decisions.
.png)
.png)




