




.png)


The phone call ends. You remember only fragments. A scan showed something. Someone said “mass,” “biopsy,” or “neurosurgery.” A family member asks what the doctor said, and you realize you can't put it into a clean sentence yet.
That's a very human place to be.
A diagnosis involving the brain or spinal cord often feels different from other cancer conversations because it touches the parts of you that think, speak, move, remember, and plan. Fear shows up fast. So does confusion. Many patients and families tell me the hardest part at first isn't making every decision immediately. It's understanding what's happening well enough to ask the next good question.
Your Guide to Navigating a CNS Cancer Diagnosis
When people hear central nervous system cancer, they often feel as if life has split into “before” and “after.” One day you're dealing with headaches, weakness, blurred vision, or a strange seizure. The next day you're trying to understand scans and pathology reports that sound like another language.
If that's where you are, slow down. You do not need to master everything today.
In the United States, brain and other nervous system cancer is uncommon, making up about 1.2% of all new cancer cases, but it still carries serious consequences. The SEER program projects 24,740 new cases and 18,350 deaths in 2026, and reports that the 5-year relative survival rose from 31.0% in 1993 to 34.2% in 2023 (SEER brain and nervous system cancer statistics). Those numbers matter for perspective, but they don't define what your own path will look like.
What helps early is turning shock into structure.
First anchor: your diagnosis is not just a tumor name. It includes where it is, how it behaves, what the biopsy shows, and what symptoms it's causing in your daily life.
That's why the first appointments matter so much. Your team is trying to answer practical questions: Is this a tumor that started in the brain or spinal cord? Is surgery possible? What symptoms need treatment now? What tests are still missing? If you're preparing for that first visit, this guide to what to expect at your first oncology appointment can help you organize questions, medications, and records.
A good roadmap doesn't erase fear. It makes fear less isolating. It gives you handles. And once you have handles, decisions start to feel possible.
What Is Central Nervous System Cancer
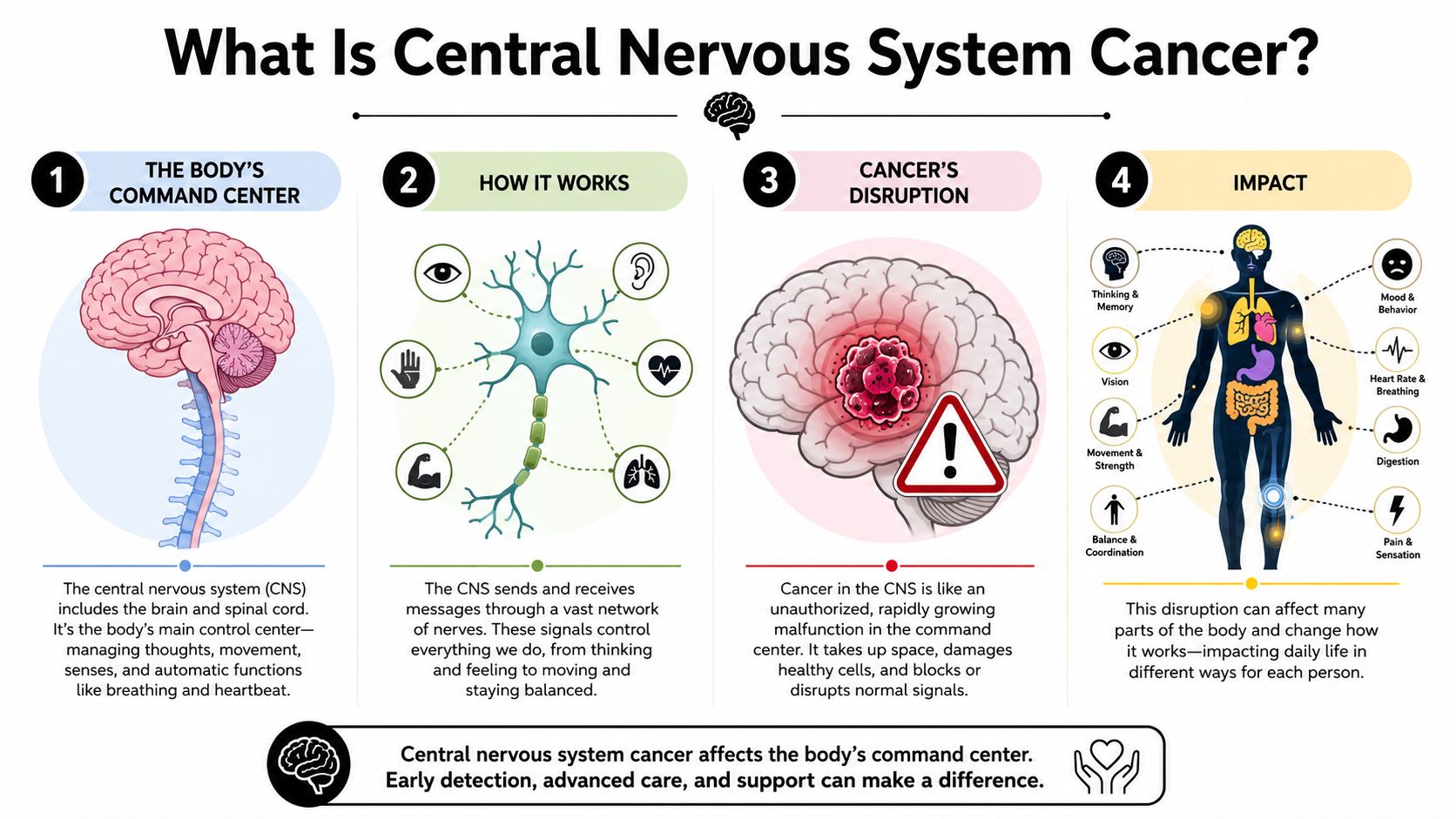
Central nervous system cancer affects the body's main communication network. The CNS includes the brain and spinal cord, which work together to receive information, process it, and send signals back out. That is how you speak, move, remember, balance, feel sensation, and control many automatic functions your body handles in the background.
A tumor in this area can disrupt those signals the way a problem in a home's electrical panel can affect many rooms at once. The concern is not only abnormal cell growth. It is also the fact that the growth is happening in tissue that controls daily life.
The first distinction that changes everything
Early on, doctors usually sort CNS tumors into two broad groups: primary and metastatic.
A primary CNS cancer begins in the brain, spinal cord, or nearby supporting tissues. In other words, it starts inside the central nervous system itself.
A metastatic CNS cancer begins somewhere else in the body and later spreads to the brain or spinal cord. Even after it spreads, it keeps the name of the original cancer. Lung cancer that has spread to the brain is still lung cancer. Breast cancer that has spread to the brain is still breast cancer.
This difference matters because treatment is built around the tumor's biology, not just its address in the body.
| Feature | Primary CNS Cancer | Metastatic CNS Cancer |
|---|---|---|
| Where it starts | In the brain, spinal cord, or nearby tissues | In another organ, then spreads to the CNS |
| How it is named | Named by the CNS tumor type | Named by the original cancer type |
| Treatment planning | Based heavily on tumor type, grade, location, and molecular features | Based on both the CNS involvement and the original cancer's biology |
| Key question | “What kind of brain or spinal tumor is this?” | “What cancer spread here, and how is it behaving now?” |
Why one CNS diagnosis can look so different from another
CNS tumors are a broad group of diseases, not a single illness. Doctors look at several layers at once: the tumor's cell type, how quickly it appears to grow, exactly where it sits, whether it can be removed safely, and what its molecular testing shows.
That is why two patients can both be told they have a brain tumor and still face very different decisions.
One tumor may be slow-growing and located in an area surgeons can reach more safely. Another may be smaller but sit beside tissue that controls speech, movement, or vision. A spinal cord tumor may create major symptoms even when it is not large, because there is so little extra space around those nerve pathways.
A CNS diagnosis has two core parts. What the tumor is, and where it is.
Families often find the second part surprising. In the brain and spinal cord, location can matter as much as size. A small tumor in a sensitive area can cause more trouble than a larger one in a less critical spot.
This is also where the patient journey starts to become more manageable. Once your team defines the tumor type and location clearly, the next questions become more practical. What symptoms need relief now? Which treatments are realistic? What can protect function and quality of life? For people with advanced or treatment-resistant disease, those answers may also include newer approaches designed to target the cancer more precisely while limiting added strain on the rest of the body.
Common CNS Cancer Types and Symptoms
When patients ask why they feel the symptoms they feel, I often use a neighborhood analogy. The brain isn't one uniform organ. It's more like a city with specialized districts. A tumor affects the functions handled in its neighborhood.
That's why the same diagnosis can look very different from person to person.
Tumor names you may hear
Some common primary CNS tumor categories include:
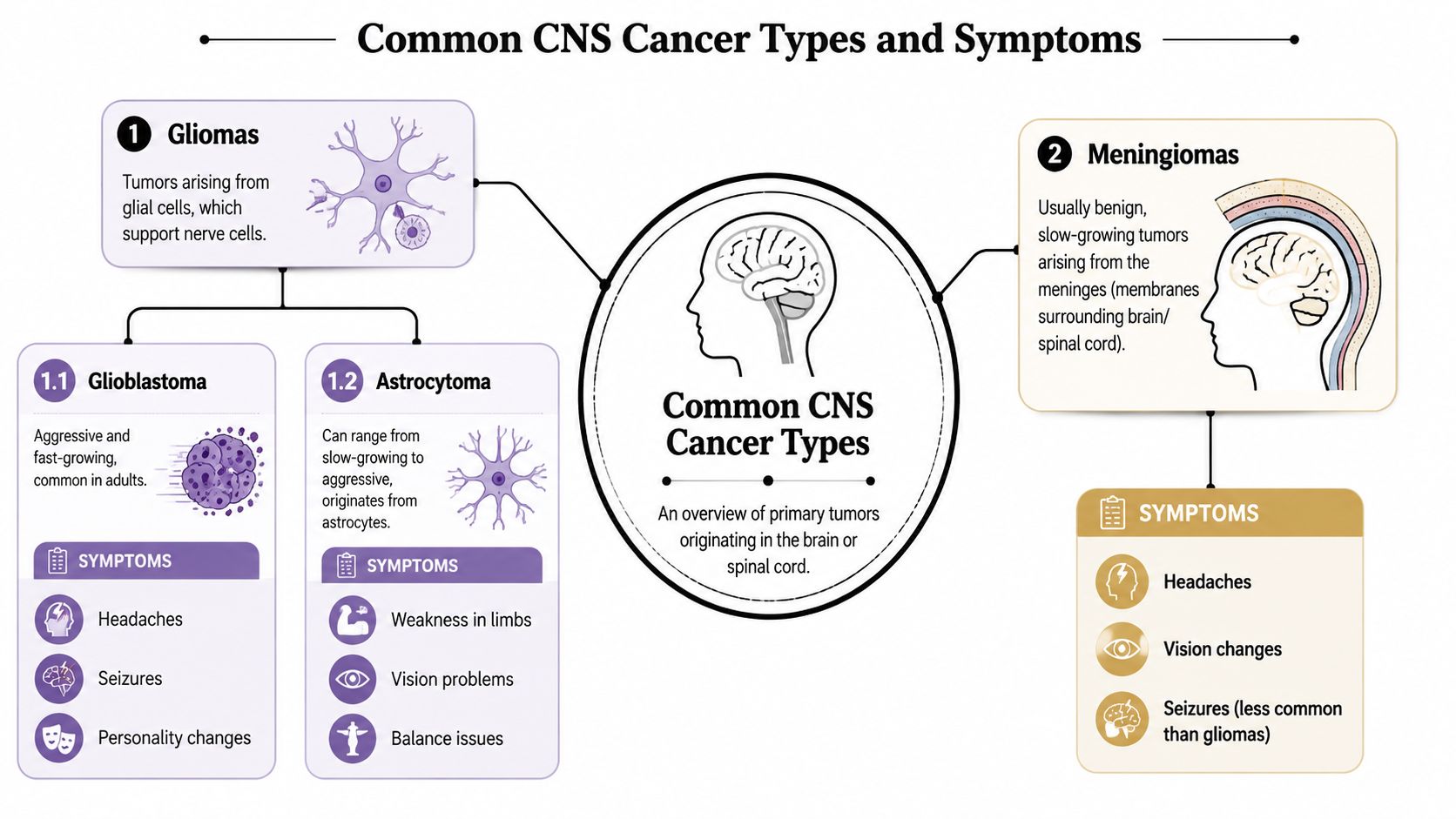
Gliomas
These begin in glial cells, which support and protect nerve cells. This is a broad family, not a single diagnosis.Glioblastoma
This is a fast-growing type of glioma. Families often hear about it early because it can cause symptoms that build quickly.Astrocytoma
This develops from astrocytes, a type of glial cell. Some astrocytomas grow more slowly, while others behave more aggressively.Meningioma
This arises from the meninges, the layers covering the brain and spinal cord. Many are not cancerous in the same way patients imagine malignant tumors, but they can still cause major problems because of pressure and location.
This short video gives a useful visual overview before the details become more technical.
Why symptoms depend on location
A frontal lobe tumor may show up first as personality change, poor judgment, apathy, or trouble organizing tasks. Families sometimes notice, “They just don't seem like themselves.”
A tumor near the motor cortex may cause weakness, clumsiness, or trouble using one arm or leg.
A tumor affecting visual pathways may cause blurred vision, missing part of the visual field, or trouble reading.
A tumor near language areas can lead to word-finding trouble. A person may know what they want to say but can't get the right word out. That can be frightening, especially when it appears suddenly.
Symptoms are often functional clues
Some of the more common symptoms patients report include:
- Headaches that are new, changing, or accompanied by nausea
- Seizures, even in someone with no seizure history
- Weakness or numbness in part of the body
- Balance problems or new falls
- Vision changes
- Speech or memory problems
- Mood or behavior changes
These symptoms don't automatically tell you the tumor type. They tell you what part of the nervous system may be under stress.
Sometimes the most useful question isn't “Why do I have this symptom?” It's “What function does this brain area control?”
That question helps many families make sense of what otherwise feels random. A seizure, personality change, and arm weakness may seem unrelated. In CNS disease, they can all trace back to where the tumor is sitting and what tissue it's affecting.
A symptom doesn't measure your strength
Patients often blame themselves for being tired, forgetful, or emotionally reactive. They shouldn't. CNS tumors can directly affect memory, speech, mood, sleep, and concentration. On top of that, antiseizure drugs, steroids, surgery, and radiation can also change how a person feels and functions.
That means “I'm not myself” is not a failure. It's clinical information. Tell your team clearly and early.
How Doctors Diagnose and Stage CNS Cancer
You hear the word "mass" after a scan, and the room seems to go quiet. Then the questions come fast. Is it cancer. What kind. How serious. What happens next.
Doctors answer those questions in steps, because each test adds a different piece of information. The early goal is not just to confirm that something is there. It is to learn where it is, what it is made of, and how it may affect daily life and treatment choices.
Diagnosis starts with location and function
A neurological exam is often the first structured clue. Your doctor checks strength, sensation, reflexes, balance, eye movements, speech, and memory. That exam works like a functional map. It can suggest which part of the brain or spinal cord is under pressure or irritation, even before the full imaging review is complete.
Imaging then shows the anatomy more clearly. MRI is usually the main scan in CNS care because it gives a more detailed view of soft tissue than CT in many situations.

Many patients are told they need contrast, often gadolinium, and that can sound alarming. In plain terms, the contrast helps certain abnormal areas stand out more clearly on the scan, which can help doctors define the borders of a lesion and plan the next step. If you have been wondering why one test was ordered instead of another, this guide to CT scan vs MRI explains the difference in patient-friendly terms.
Sometimes additional imaging is needed. A doctor may order spine MRI, advanced brain imaging, or scans of other parts of the body if the main question is whether the CNS lesion started there or spread from somewhere else.
A scan can suggest the diagnosis. Tissue confirms it.
An MRI can raise strong suspicion for a tumor, but the scan alone usually cannot give the final answer. For that, doctors often need tissue from a biopsy or surgery.
The pathology review tells the team what type of tumor is present and how abnormal the cells look under the microscope. That matters because two lesions can appear similar on imaging while requiring very different treatment plans.
Families often get tripped up by the words grade and stage. They are not interchangeable in CNS cancer care.
- Grade describes how aggressive the tumor cells appear biologically
- Tumor type identifies what kind of cells the tumor comes from
- Location explains what nearby functions may be at risk
- Extent of spread or removal helps shape prognosis and treatment planning
A simple question can keep this part of the discussion grounded: "What is the exact diagnosis in plain language, and what does that mean for treatment now?"
Staging is different in CNS tumors
For many cancers, staging focuses heavily on tumor size, lymph nodes, and spread to distant organs. CNS tumors do not always fit neatly into that model. Doctors are often more focused on the tumor's exact location, whether it can be safely removed, how it looks under the microscope, and whether it has spread within the brain, spinal cord, or cerebrospinal fluid.
That difference can be confusing, especially for families trying to compare CNS cancer with breast, lung, or colon cancer. In brain and spinal cord tumors, biology and anatomy often carry more day-to-day meaning than a traditional stage label.
Molecular testing has changed the picture
Modern diagnosis now goes beyond what a pathologist sees through the microscope. Current CNS tumor classification also uses molecular features to define the diagnosis more precisely. Markers such as IDH status, H3-related changes, CDKN2A/B loss, promoter alterations, and methylation patterns can refine the diagnosis and sometimes change the expected behavior of the tumor or the treatments worth considering (WHO CNS5 molecular classification review).
That level of detail can feel overwhelming at first. It also gives patients something important. A more precise map.
When a tumor is defined more accurately, the care team can make more specific decisions about surgery, radiation, drug therapy, clinical trials, and options for treatment-resistant disease. For patients in specialized centers, that can open the door to approaches designed to control disease while protecting function and quality of life as much as possible.
Standard and Emerging Treatment Strategies
After a CNS cancer diagnosis, families often want one clear answer. What is the treatment? In reality, treatment usually works more like a carefully sequenced plan, with each step chosen for a reason. The team is weighing two goals at the same time. Control the tumor, and protect the parts of life that matter every day, such as speech, memory, movement, and independence.
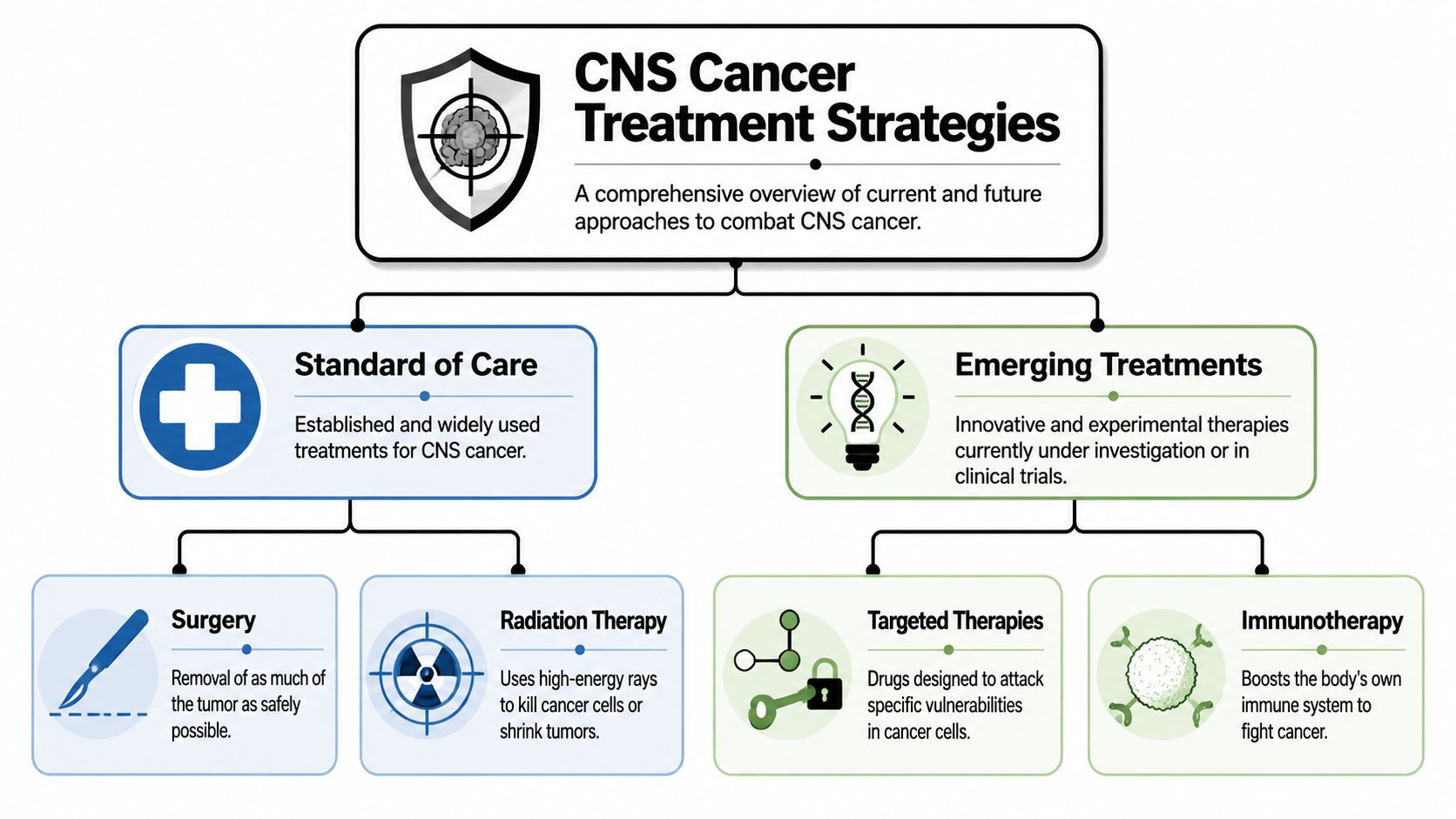
The standard toolkit
Surgery is often the first step if the tumor can be reached safely. Surgery may remove as much visible tumor as possible, reduce pressure inside the skull, or collect tissue so the diagnosis is precise. In the brain and spinal cord, the goal is not merely “take out more.” The goal is to remove what can be removed without causing avoidable harm.
Radiation therapy uses focused energy to injure tumor cells so they cannot keep growing. It may be used after surgery, instead of surgery, or for tumor areas that remain after an operation. The exact plan depends on where the tumor sits and how much nearby normal tissue needs protection.
Chemotherapy and other drug-based treatments may be used to lower the risk of the cancer returning, treat diffuse disease, or reach tumor cells that surgery cannot remove. Some CNS tumors respond well to these medicines. Others do not. That is one reason the exact tumor type matters so much.
How treatment decisions are becoming more precise
Treatment choices are now guided by more than the tumor's appearance under a microscope. Molecular testing can reveal changes inside the cancer cells that point toward a better treatment match. This has shifted care away from a one-plan-for-everyone model and toward decisions based on the tumor's biology, the patient's symptoms, and the life the patient is trying to preserve.
Two examples come up often in these conversations.
Targeted therapy is designed for tumors with a specific weakness, such as a mutation or pathway the cancer relies on.
Immunotherapy aims to help the immune system recognize and attack cancer cells more effectively. For a plain-language overview, this guide to what immunotherapy for cancer means can help families understand the basic idea before discussing whether it fits a CNS tumor.
Some specialists also adjust dose, schedule, or drug combination to reduce side effects while still treating the disease seriously. That approach can matter for older adults, people with neurologic symptoms, and patients who have already been through intensive treatment.
A useful example: primary CNS lymphoma
Primary CNS lymphoma, or PCNSL, shows how this field is changing. Standard treatment has long relied on methotrexate-based chemotherapy. At the same time, clinicians remain concerned about treatment-related effects on memory and thinking, especially when whole-brain radiation is used in patients who may be more vulnerable to neurotoxicity. Newer approaches being studied or used in selected settings include BTK inhibitors, immune modulators, CAR T-cell therapy, and bispecific antibodies, with continuing work on biomarkers that may help predict recurrence and guide treatment selection (End Brain Cancer Initiative overview of PCNSL).
That question matters in clinic every day. Families are not only asking whether a treatment can shrink a tumor. They are also asking what the treatment may do to concentration, personality, stamina, and the ability to live at home.
The strongest plan is the one that treats the cancer while protecting as much function and quality of life as possible.
For patients seeking outpatient evaluation of advanced cancer options in Brooklyn, one local practice, Hirschfeld Oncology, describes care built around immunotherapy, targeted therapy, low-dose chemotherapy, symptom management, and individualized regimens. That reflects a broader shift in CNS cancer care toward more personalized and often less toxic options, especially for disease that has returned or has not responded to standard treatment.
Symptom Management and Practical Guidance
Many people hear palliative care and think it means giving up. That misunderstanding causes real harm. In CNS cancer, symptom management should begin early because symptoms often affect daily life long before treatment is finished.
Palliative care means relief of suffering. It includes help with pain, headaches, nausea, seizures, sleep, mood, fatigue, constipation, appetite changes, thinking problems, and family stress. It can happen alongside surgery, radiation, chemotherapy, or newer therapies.
What symptom support looks like in real life
Patients often need practical strategies, not just reassurance.
For cognitive fog
Keep a single notebook or phone note for appointments, medication changes, and questions. Ask a family member to attend visits and take notes. Use alarms for medications and hydration.For fatigue
Stop measuring your day by pre-diagnosis standards. Break tasks into smaller units. Save your most mentally demanding work for the time of day when your energy is best.For mood and irritability
Remember that brain tumors, steroids, antiseizure drugs, and sleep disruption can all change emotional regulation. Report changes early. A sudden shift in behavior is a medical issue, not a character flaw.For seizure safety
Ask directly what to do if a seizure happens at home, when to call emergency services, and whether driving restrictions apply.
Younger adults often need different care conversations
Adolescents and young adults are often underserved in CNS cancer care. Brain and CNS tumors are the second most common cancer type in people ages 15 to 39 and a leading cause of cancer-related death in that age group. A Duke review highlights an estimated 12,848 AYA diagnoses annually and emphasizes issues many standard cancer pages barely address, including fertility preservation, school and work disruption, and long-term neurocognitive effects (Duke discussion of brain and CNS tumors in adolescents and young adults).
That changes the goals conversation.
A younger patient may be thinking about graduation, parenting, dating, career identity, fertility, and whether they'll be able to return to independent living. Those are not secondary concerns. They are central concerns.
If you're a younger adult, ask your team to address the life you're trying to return to, not just the scan you're trying to improve.
Questions worth bringing to clinic
Function first
What symptoms should improve with treatment, and which ones may take longer?Rehab needs
Would I benefit from speech therapy, occupational therapy, neuropsychology, or physical therapy?Daily living
Is it safe for me to work, drive, live alone, manage finances, or supervise children?Future planning
Are there treatments that could affect fertility, long-term memory, or school and career plans?
When patients ask these questions early, care becomes more humane and more useful.
Finding Hope with Advanced Care in NYC
A CNS cancer diagnosis often begins with a blur. One appointment leads to another. New words appear fast. Families are asked to make decisions while still absorbing what the diagnosis means.
Hope grows when the next steps become clearer.
In practice, that often means finding a team that can do two things at once. The first is treat the cancer with care that fits the tumor's biology and your overall health. The second is protect as much of daily life as possible, including thinking, mobility, speech, comfort, and independence. For some people, standard treatment close to home is the right path. For others, especially after recurrence, limited response, or difficult side effects, a second opinion can open up choices that were not fully discussed at the start.
Supportive care belongs in that plan from the beginning. Rehabilitation can help with strength, balance, endurance, speech, and recovery after surgery or during treatment. Families who want to understand how physical recovery fits alongside cancer care may find practical guidance in resources on oncology and physical therapy.
The larger point is reassuring. The first version of the story is rarely the final one. Pathology can be refined. Molecular testing can clarify options. Symptoms can often be treated more effectively than families expect. A careful review may identify a lower-toxicity approach, a clinical trial discussion, or a better way to match treatment intensity to your goals.
If you are in Brooklyn, Williamsburg, Bushwick, or elsewhere in NYC, it is reasonable to look for consultation that addresses both the cancer and the life around it. That includes treatment planning, symptom burden, quality of life, and what remains possible if the disease is advanced or resistant to prior treatment.
If you are exploring options for advanced or difficult-to-treat cancer, Hirschfeld Oncology offers consultations focused on individualized treatment planning, outpatient infusion care, symptom management, and discussion of therapies such as immunotherapy, targeted therapy, and lower-toxicity approaches when appropriate.
.png)
.png)




