




.png)


A chemo sore throat often starts gradually. Food feels scratchy. Water suddenly stings. By the next day, swallowing pills, eating toast, or even talking for long stretches can feel like work.
That change is frightening when you're already dealing with cancer treatment. Patients often worry it means something is going badly wrong, or that they'll have to choose between staying on treatment and being able to eat. In most cases, that's not the choice in front of you. A chemo sore throat is common, painful, and disruptive, but it is usually manageable with the right plan and quick communication.
The most useful approach is to act early, not wait until your mouth and throat are badly inflamed. Good care starts before infusion day, continues through treatment, and includes a clear threshold for when home remedies aren't enough.
Your Guide to Managing a Chemo Sore Throat
You finish an infusion, go home, and by that evening water feels sharp on the way down. The next morning, breakfast takes twice as long, your pills are harder to swallow, and you start wondering whether this is a minor irritation or something that could interfere with treatment.
That uncertainty is common. A chemo sore throat can affect eating, drinking, sleep, speech, and energy in a matter of days. It also has practical consequences. Patients often eat less, drink less, and wait too long to mention it because they assume it is just part of chemo.
Early planning makes a real difference. Before treatment starts, ask your oncology team whether your regimen commonly causes mouth or throat irritation, whether you should begin a bland rinse routine on day one, and what symptoms should trigger a same-day call. If you want a plain-language refresher on how chemotherapy affects fast-growing cells, that helps explain why the throat can become so sensitive during treatment.
Good management is specific and proactive. “Soft foods” is too vague to help when swallowing hurts. Patients usually do better with a clear plan for rinses, food texture, drink temperature, pain control, and a backup plan for days when intake drops.
For infusion center patients, the best time to prepare is before symptoms appear. Bring a water bottle, ask whether ice chips or cold water are appropriate with your regimen, keep a symptom note on your phone after each cycle, and report early burning or tenderness instead of waiting for visible sores. That gives your team a chance to adjust supportive care before small irritation becomes poor hydration, weight loss, or missed medications.
I advise patients to use three tracks:
- Start prevention before the first treatment
- Use daily soothing care at the first sign of pain
- Contact the oncology team promptly if swallowing, fluids, or fever become a concern
A sore throat during chemo should be treated as a symptom to manage early, not a test of endurance. The goal is straightforward. Keep you eating, drinking, and staying on treatment as safely and comfortably as possible.
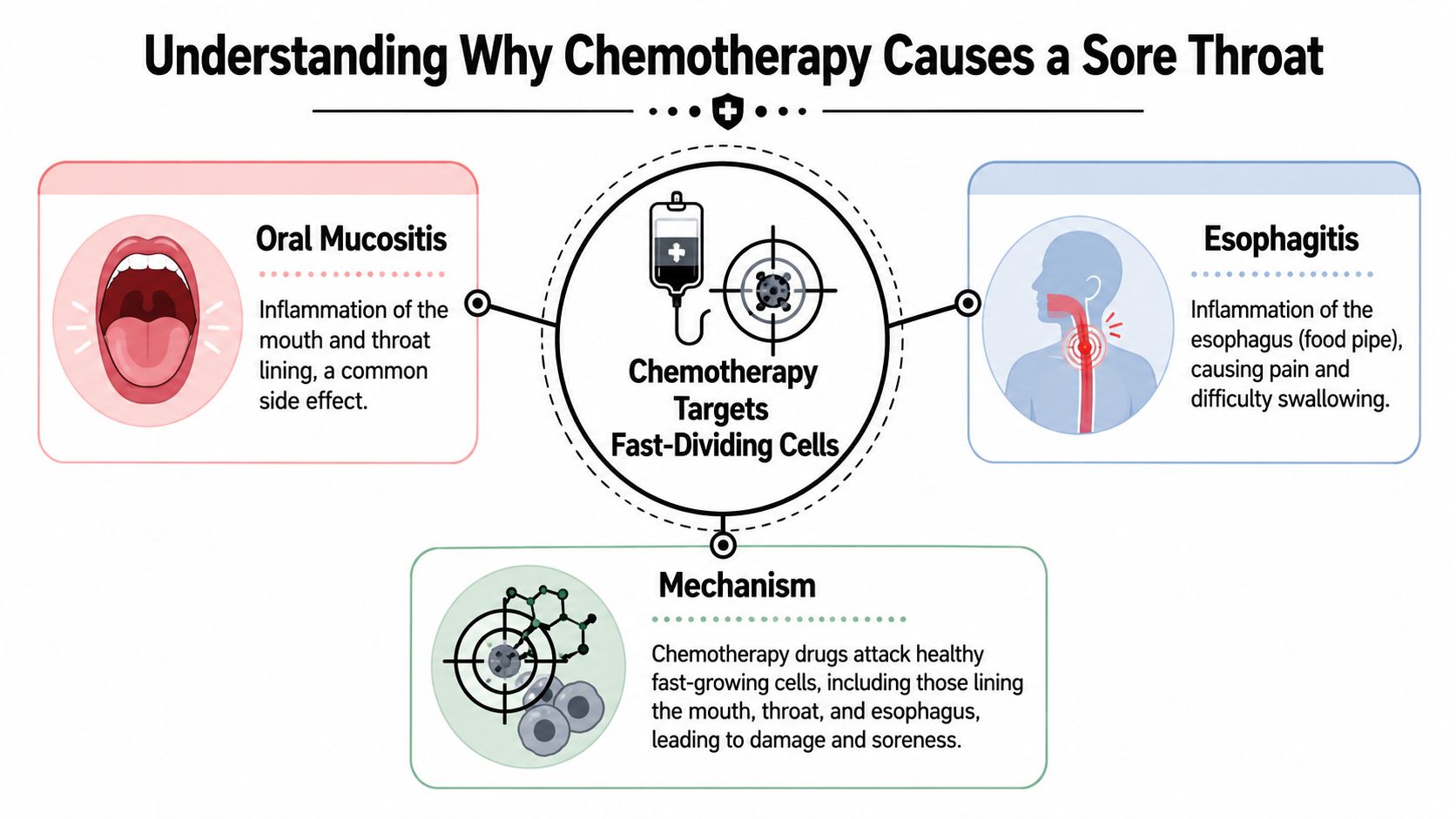
Understanding Why Chemotherapy Causes a Sore Throat
A patient often notices this a few days after an infusion. Water starts to sting. Toast feels sharp. Swallowing takes more effort than it should. In many cases, that pain is not an ordinary sore throat from a cold. It is treatment-related inflammation of the tissues lining the mouth and throat.
Fast-growing cells get caught in the crossfire
The usual reason is oral mucositis. That term means the moist lining of the mouth and throat has become inflamed and injured during treatment. If the irritation extends farther down the swallowing tube, clinicians may call it esophagitis. Patients usually describe both in plain terms. Swallowing hurts, eating is harder, and even talking can become uncomfortable.
Chemotherapy targets cells that divide quickly. Cancer cells fit that description, but so do many healthy cells in the mouth and throat. Those tissues normally repair themselves fast. During chemotherapy, that repair process slows down, the surface becomes more fragile, and everyday friction starts to matter. A plain-language review of how chemotherapy affects fast-growing cells helps explain why this side effect is so common.
That is why foods and drinks that were easy to tolerate before treatment can suddenly burn or scrape. Citrus, tomato products, alcohol-based mouthwash, hot coffee, crusty bread, and dry snacks often become painful because the lining has lost some of its usual protection.
Why severity differs from one patient to another
The same drug does not affect every patient the same way. Risk tends to rise with higher-intensity treatment, certain drug combinations, and treatment plans that include radiation, especially in the head and neck area. In practice, I also pay close attention to dental problems, poorly fitting dentures, dry mouth, and tobacco or alcohol use, because each one can add more irritation to tissue that is already healing slowly.
Head and neck cancer treatment is a common example. The Head and Neck Cancer Alliance notes that oral mucositis is one of the most common and debilitating side effects during chemotherapy or radiation for these patients. That matters before the first infusion, not just after symptoms start, because broken teeth, gum disease, and denture friction can turn mild tenderness into much more severe pain.
This is one of the trade-offs of effective cancer treatment. The goal is to damage cancer cells, but healthy fast-renewing tissue can be injured at the same time.
What the timing often feels like
A chemo sore throat does not always begin on treatment day. It may build gradually over several days in the cycle, then become obvious when normal meals suddenly feel difficult. Many patients first notice burning with acidic foods, then pain with swallowing, then a raw sensation even with bland liquids.
Common triggers include:
- Alcohol and tobacco, which irritate inflamed tissue
- Acidic foods such as citrus and tomatoes
- Hot drinks, which can sting sensitive lining
- Rough foods like chips, crusty bread, or dry crackers
- Ill-fitting dentures, because repeated friction worsens injury
For infusion center patients, this pattern is useful to recognize early. If symptoms reliably appear a few days after each cycle, tell your team that timing. It helps us decide whether you are dealing with expected mucositis, reflux, thrush, dehydration, or a medication effect that needs a different plan.
A few practical questions can improve care before the problem becomes severe: Which drugs in my regimen are most likely to irritate the mouth or throat? When during the cycle should I expect symptoms? Should I start a rinse routine before pain begins? If swallowing becomes difficult, when do you want me to call the same day?
Understanding the cause changes what helps. This is tissue injury from treatment, so the best response is early protective care, good symptom tracking, and prompt communication with your oncology team if eating, drinking, or swallowing starts to slip.
Proactive Prevention and Superior Oral Care
A sore throat is easier to prevent than to calm once swallowing already hurts. The patients who do best usually start their mouth care before the first infusion, not after the first painful week.
Start before the first infusion
Pre-treatment planning pays off here. Mayo Clinic advises regular bland rinses during cancer treatment, and many oncology teams recommend starting a sodium bicarbonate rinse routine before symptoms appear, especially if your regimen has a higher risk of mouth irritation. A simple mixture often used is 1 teaspoon of baking soda in 8 ounces of water, if your team agrees with that plan and timing.
The trade-off is simple. Prevention takes a few minutes several times a day. Rescue care often means poorer intake, more pain, and last-minute calls because eating and drinking fell off faster than expected.
For infusion center patients, this is the time to ask specific questions, not broad ones. Ask: Do you want me to begin rinses a few days before treatment? Is there any reason my regimen changes that plan? If I already have reflux, thrush history, or dentures, should my oral care routine be adjusted before cycle one?
If you want a closer look at new methods for reducing chemotherapy-induced oral mucositis, review them with your oncology team so the plan fits your drugs and your risk factors.
What daily oral care should actually look like
Good oral care during chemotherapy is gentle and repetitive. Aggressive products usually backfire.
A practical routine often includes:
- Soft brushing with a soft-bristle toothbrush after meals and before bed
- Bland rinses such as baking soda or salt water if your team recommends them
- Alcohol-free mouth products because alcohol can sting inflamed tissue
- Steady hydration to keep the mouth and throat from getting dry and more painful
- Lip balm to protect cracked lips and reduce mouth breathing discomfort
- Denture checks so rubbing spots are fixed early, before they turn into ulcers
I also tell patients to look at their mouth once a day in good light. Red patches, white coating, small ulcers, or new denture pressure points are easier to manage when caught early.
If your gums are tender between treatments, you can also discover natural gum care tips. Use outside advice carefully during chemotherapy, and clear new products with your oncology team first.
Infusion-day prevention that can make a real difference
For some regimens, ice chips during the infusion can help lower mouth exposure to the drug. This approach, called oral cryotherapy, is used selectively. It is practical in the infusion chair, but it is not right for every chemotherapy plan, and some patients find it unpleasant or too cold to tolerate.
A 2020 MASCC/ISOO clinical practice guideline supports oral cryotherapy for certain short-infusion chemotherapy drugs associated with oral mucositis risk. Ask your infusion nurse or oncologist whether your regimen is one where this makes sense, how long to do it, and whether there is any reason to avoid it in your case.
Questions worth asking before treatment starts:
- Do you recommend a dentist visit before my first cycle
- Should I begin baking soda rinses before treatment or wait until symptoms show up
- Is my regimen one where ice chips during infusion may help
- Which mouthwash ingredients should I avoid
- If dentures start rubbing, do you want me to leave them out more often
- What change in swallowing should prompt a same-day call
Early mouth care is not fancy. It is disciplined. That usually works better.
At-Home Remedies for Soothing a Sore Throat
A common pattern starts a few days after treatment. Water stings, toast feels abrasive, and even swallowing saliva gets your attention. At home, the job is simple. Soothe the tissue, keep fluids coming in, and make eating possible enough that you do not fall behind between infusions.

Rinses that are simple and worth doing
For many patients, the most reliable first step is a bland rinse used often and gently. The American Cancer Society's guidance on mouth and throat problems during cancer treatment supports frequent rinsing with mild solutions such as salt water or baking soda rinses to keep the mouth cleaner and more comfortable.
A practical home recipe is:
- 1/2 teaspoon of salt in 8 ounces of water, or
- 1/2 teaspoon of baking soda in 8 ounces of water
Use the one that feels better, or alternate them if your team agrees. Rinse several times through the day, especially after meals and before bed.
A few details matter:
- Swish gently
- Spit it out unless your oncology team told you to swallow it
- Mix it fresh regularly
- Use lukewarm or room-temperature water if extremes bother you
Patients in infusion centers often ask whether they should start rinses only after pain begins. In practice, many teams prefer patients to have supplies ready before the first cycle so there is no delay once symptoms show up. If your regimen has a higher mucositis risk, ask your nurse exactly when they want you to start and how often they want you rinsing at home.
Food choices that reduce friction
During a chemo sore throat, texture often matters more than nutrition labels. Soft, moist foods usually do best. Dry, rough, acidic, spicy, and very hot foods commonly make pain worse.
This side-by-side approach helps patients make faster decisions:
| Better tolerated | Often aggravating |
|---|---|
| Yogurt | Citrus fruits |
| Mashed potatoes | Tomato sauces |
| Smoothies | Chips and toast |
| Scrambled eggs | Spicy foods |
| Lukewarm oatmeal if tolerated | Very hot soup |
| Cottage cheese or soft pasta | Dry crackers |
The trade-off is straightforward. A food can be healthy on paper and still be the wrong choice for a raw throat. During active irritation, calories, protein, and fluids that you can swallow comfortably are usually more useful than forcing down foods that scrape and slow you down.
Cold or room-temperature foods often work better than hot meals. Not for everyone, but often enough that it is worth testing early in the day rather than waiting until dinner fails.
Small adjustments that make swallowing easier
Small changes can save a day of poor intake.
- Use a straw if it helps liquids bypass the most painful area.
- Take small bites and sips
- Add sauce, broth, or gravy to soften foods
- Choose high-calorie liquids when chewing feels like too much work
- Avoid alcohol and tobacco while the tissue is trying to heal
If gum irritation is part of the picture too, you can discover natural gum care tips. During chemotherapy, clear any new rinse, gel, herb, or oral product with your oncology team first. Natural does not always mean gentle on damaged tissue.
When taste changes are part of the problem
Sometimes the throat pain is only half the issue. Taste changes can make familiar foods seem metallic, bitter, flat, or strangely sweet. The National Cancer Institute notes that cancer treatment can change taste and smell, and that cooler foods, softer foods, and liquid nutrition may be easier to tolerate for some patients (NCI nutrition guidance).
That is useful because it gives you a plan. If warm meals suddenly seem unbearable, try chilled smoothies, cold oral nutrition drinks, pudding, yogurt, or blended soups served cool rather than hot. If one flavor becomes intolerable, switch categories entirely instead of forcing it. Sweet to savory, dairy to non-dairy, vanilla to fruit, thin liquids to thicker ones.
I usually tell patients to test options early and keep a short list of two or three foods and drinks that reliably go down. Bring that list to the infusion center if intake drops. It helps your team decide sooner whether simple home care is enough or whether you need prescription support.
A brief demonstration can help with meal planning:
If food suddenly tastes wrong, do not assume you are being difficult. Chemotherapy can change taste enough that temperature, texture, and timing decide whether you eat at all.
Medical Treatments and Pain Management Options
A common turning point happens a few days after infusion. Swallowing starts to hurt enough that water intake drops, meals get skipped, and sleep becomes fragmented. That is the point to stop trying to push through and ask for a treatment plan that is built for pain control, hydration, and safe swallowing.
Prescription support usually falls into three practical categories. Topical anesthetics numb the surface so eating and drinking are less painful. Coating or compounded rinses are used to protect irritated tissue and, in some clinics, combine several ingredients in one mouth rinse. Systemic pain medicines help when the soreness is deeper, more constant, or bad enough that a rinse alone will not carry you through the day.
Each option has trade-offs. A numbing rinse can make meals possible, but too much numbness can make swallowing feel clumsy and can increase the risk of burning your mouth with hot food or drinks. I usually advise patients to ask exactly when to use it, how long to wait before eating, and which textures are safest afterward. Those details matter more than the product name.
For some patients, the best plan is scheduled pain control rather than waiting until every swallow hurts. The Multinational Association of Supportive Care in Cancer and International Society of Oral Oncology oral mucositis guidance supports patient-controlled morphine for mucositis pain in the setting of hematopoietic stem cell transplantation, which reflects a broader oncology principle. Severe treatment-related mouth and throat pain often responds better when medication stays ahead of the pain rather than chasing it after it spikes (MASCC/ISOO mucositis guidelines).
What to ask your oncology team before the next infusion, especially if throat pain started early in the cycle:
- Should I have a prescription rinse ready at home before symptoms peak?
- Do you want me using the medicine before meals, on a set schedule, or only as needed?
- If my swallowing feels weak after a numbing rinse, what should I avoid?
- At what point do you want me to call for stronger pain control?
- If my intake drops, when do you want me to come to the infusion center for fluids or assessment?
- Does my chemotherapy regimen put me at higher risk for mouth or throat mucositis next cycle?
That last question is useful because not every regimen behaves the same way. Infusion center patients often do better when the plan is made proactively. If a prior cycle caused significant throat pain, your team may adjust supportive medications early, arrange follow-up calls, or bring you in sooner for hydration and symptom review instead of waiting for an emergency.
Some approaches usually make things worse:
- Alcohol-based mouthwashes, which sting and dry irritated tissue
- Delaying prescribed pain medicine until pain is severe
- Dry, rough, spicy, or very hot foods right after numbing medication
- Starting supplements or herbal products without an oncology pharmacist or clinician reviewing interactions first
If you're interested in broader supportive wellness discussions, you can explore Herbswell's adaptogen article. Keep in mind that “natural” does not automatically mean safe during chemotherapy, especially if you are also dealing with inflamed mouth or throat tissue.
If pain remains poorly controlled, hydration slips, or swallowing becomes too difficult, the treatment plan itself may need adjusting. That can include stronger analgesics, IV fluids in clinic, closer monitoring during the expected symptom window, or changes to the chemotherapy schedule when toxicity is outweighing the current supportive plan. Patients often hear that as a setback. In practice, it is careful oncology management.
Infection risk also changes the equation. A sore throat during chemotherapy is more concerning when white blood cell counts are low, which is why it helps to understand the connection between throat symptoms and low white blood cell counts during chemo. If your team is balancing pain control with fever risk, dehydration, and swallowing safety, they are not overreacting. They are trying to keep treatment on track without letting a manageable side effect become a dangerous one.
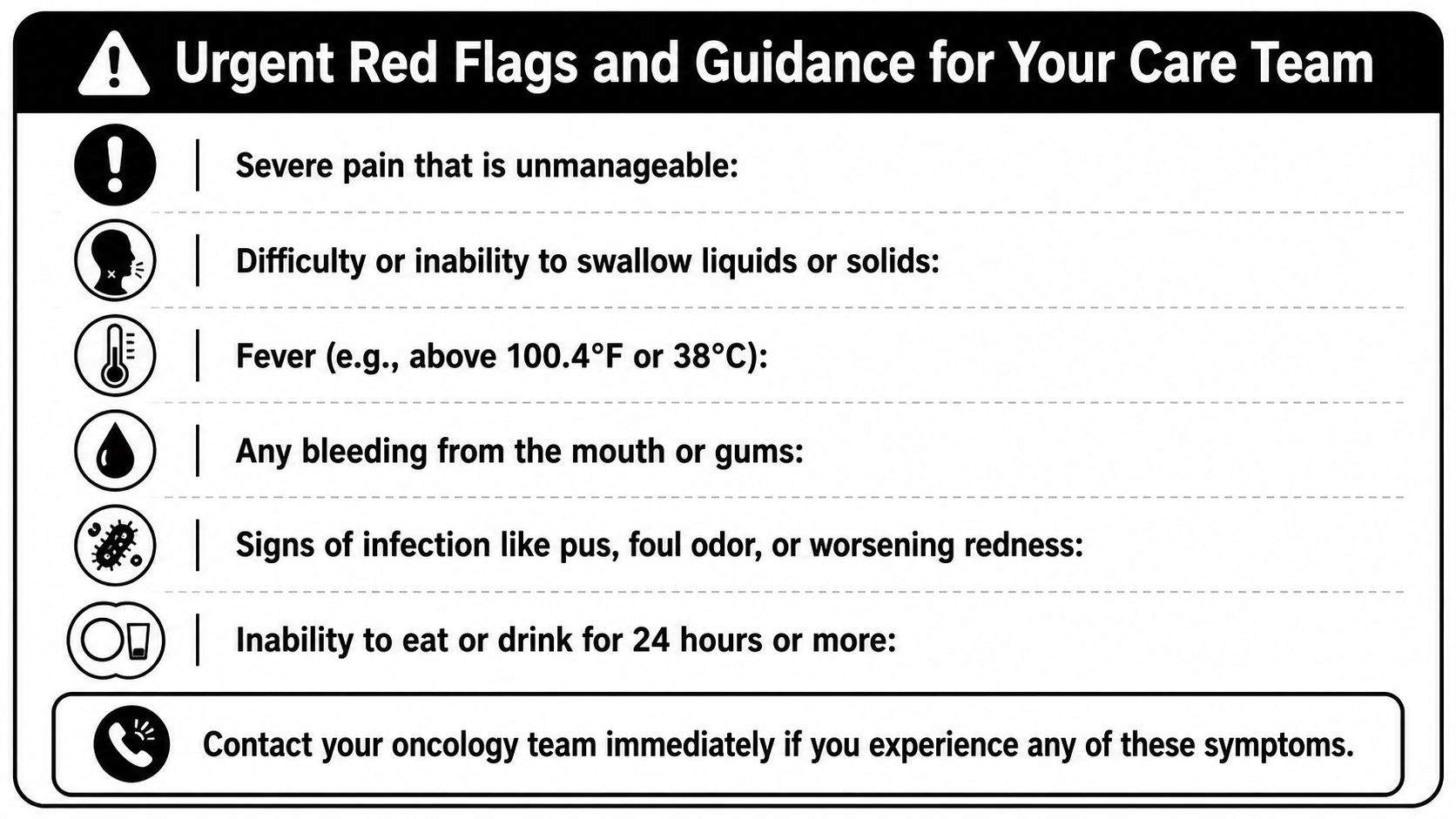
Urgent Red Flags and Guidance for Your Care Team
It is 8 p.m. after infusion. Your throat hurts more than it did this morning, swallowing water feels like work, and you are trying to decide whether this can wait until tomorrow. In that moment, the question is simple. Are you still safe to manage this at home, or do you need your oncology team tonight?
Red flags that should change your next step
For patients on chemotherapy, fever changes the situation quickly. A temperature of 100.4°F (38.0°C) or higher needs urgent medical advice, especially if you also have mouth sores, shaking chills, or feel suddenly weak. If you want a clear explanation of why infection risk rises during treatment, review this guide to low white blood cell counts during chemo.
Call your oncology team the same day, or use the after-hours number, if you have any of the following:
- Fever at or above 100.4°F (38.0°C)
- Trouble swallowing liquids or keeping up with fluids
- Pain that breaks through the medication plan you were given
- Bleeding from the mouth or gums
- New swelling, pus, foul odor, or rapidly worsening redness
- You cannot eat or drink for most of the day
- Dizziness, faintness, dark urine, or other signs of dehydration
- Shortness of breath, chest tightness, or a muffled voice
These symptoms matter because the throat can become inflamed, infected, or so painful that patients stop drinking before they realize how dehydrated they are. In the infusion setting, I want patients to plan for this before the first cycle, not after a rough night at home. Ask for the exact number to call after hours, find out whether your team wants you to go straight to the cancer center or the emergency department if fever starts, and keep a thermometer and a written symptom plan where you can reach them easily.
Questions to ask before problems escalate
The best time to ask for a rescue plan is before your throat starts to hurt. At a clinic visit or in the infusion chair, ask:
- If throat pain starts, what is the first step you want me to take at home
- Which mouth rinse do you recommend, and how often should I use it
- At what point should I call for stronger pain control
- How much fluid do you want me to drink each day, and when is low intake a concern
- Do you expect my symptoms to peak on certain days after treatment
- Am I at higher risk for mouth or throat sores with this regimen
- Should I bring anything to infusion, such as ice chips, a water bottle, or prescribed rinses
- Who should I call on nights, weekends, and holidays
Good oncology care is not just reacting to side effects. It is setting up a plan early so pain, dehydration, and infection are caught before they turn into an urgent visit. If your team adjusts supportive medications, brings you in for fluids, or changes the treatment schedule because swallowing is no longer safe, that is careful treatment management, not failure.
If you or someone you love is dealing with painful mouth or throat symptoms during chemotherapy, Hirschfeld Oncology offers practical guidance for patients navigating complex cancer treatment, including symptom management strategies that support comfort, nutrition, and safer outpatient care.
.png)
.png)




