




.png)


A rare cancer diagnosis often arrives in fragments. You hear an unfamiliar name, someone mentions pathology, then a scan gets scheduled, and suddenly your family is trying to learn an entire medical language in a weekend.
If you've been told you may have dendritic cell sarcoma, you're probably dealing with two hard things at once. First, there's the fear that comes with any cancer diagnosis. Second, there's the confusion of having a cancer so uncommon that many patients can't find clear, practical information written for real people.
This guide is meant to slow that moment down. I'm going to explain what this disease is, how doctors confirm it, what staging means, which treatments are commonly considered, and what questions matter most when you're choosing your next step. The goal isn't to overwhelm you with jargon. It's to help you understand what each part of the process means for your life, your decisions, and your sense of control.
Your First Step in Understanding a Rare Diagnosis
When a cancer is rare, people often worry that the uncertainty means no one knows what to do. That isn't true. It does mean the process has to be more deliberate.
With dendritic cell sarcoma, one of the first helpful mindset shifts is this: rarity changes how carefully the diagnosis needs to be checked, but it doesn't take away your options. Your care team still follows a logical path. They confirm exactly what the tumor is, figure out where it is and whether it has spread, then match treatment to the biology and location of the disease.
Families often get stuck on the name. They ask, “Is this a blood cancer, a sarcoma, or an immune problem?” That's a reasonable question because the words point in different directions. In plain terms, this is a cancer that arises from cells related to the immune system's communication network, and it often gets managed with the same careful planning used for other rare sarcomas.
Practical rule: For a rare diagnosis, the first goal isn't speed at any cost. It's diagnostic accuracy.
That's why second opinions, expert pathology review, and thoughtful treatment planning matter so much. If you remember one thing at this stage, let it be this: before deciding what treatment to start, make sure everyone agrees on what the tumor is.
What Is Dendritic Cell Sarcoma
Your immune system has many kinds of cells. Some do the fighting. Others do the scouting.
Dendritic cells are part of that scouting system. A simple way to think about them is as the immune system's intelligence officers. They collect information about threats and help direct the rest of the immune system toward the right target. When one of these cell types becomes cancerous, the result can be a dendritic cell sarcoma.
Why the name is confusing
The phrase combines two ideas that don't usually appear together in everyday conversation:
- Dendritic cell refers to a type of immune-related cell.
- Sarcoma means a cancer arising from connective or supporting tissues, or tumors that behave like that family of cancers.
That mix is why many patients initially hear different possibilities before the final diagnosis is confirmed. On scans or even under the microscope, these tumors can resemble other cancers.
The subtype most people mean
When doctors discuss dendritic cell sarcoma, they're often referring to follicular dendritic cell sarcoma, or FDCS. It was formally recognized as a distinct cancer entity in 1986, and it remains extraordinarily rare, accounting for less than 0.4% of soft tissue sarcomas in a recent hematology summary. The same pooled analysis of 462 reported cases found no age, gender, or racial predilection, and identified worse outcomes with young age, advanced stage, intraabdominal involvement, large tumor size, absence of lymphoplasmacytic infiltration, coagulative necrosis, and high mitotic count (hematology summary on FDCS epidemiology and risk factors).
That matters because rare doesn't mean harmless. Some dendritic cell sarcomas behave slowly. Others act much more aggressively depending on where they arise and what the pathology shows.
FDCS and IDCS at a glance
Not all dendritic cell sarcomas are the same. Two names patients may encounter are follicular dendritic cell sarcoma (FDCS) and interdigitating dendritic cell sarcoma (IDCS).
| Feature | Follicular Dendritic Cell Sarcoma (FDCS) | Interdigitating Dendritic Cell Sarcoma (IDCS) |
|---|---|---|
| Cell of origin | Follicular dendritic cells | Interdigitating dendritic cells |
| How often it comes up in patient education | More commonly discussed | Less commonly discussed |
| Typical clinical conversation | Often approached as a rare sarcoma with nodal or extranodal presentation | Often discussed as an even rarer immune-cell neoplasm |
| Diagnostic challenge | Can mimic spindle-cell tumors and other malignancies | Also requires specialist pathology review |
| Treatment planning | Usually individualized based on location, resectability, and pathology features | Also individualized because standard protocols are limited |
For patients, the practical point is simple. The exact subtype affects which pathology stains matter most, how your team interprets the tumor's behavior, and which treatment strategies make sense.
The disease name tells you where the tumor came from. It does not, by itself, tell you how it will behave. That depends on the full pathology and staging picture.
From Symptoms to a Definitive Diagnosis
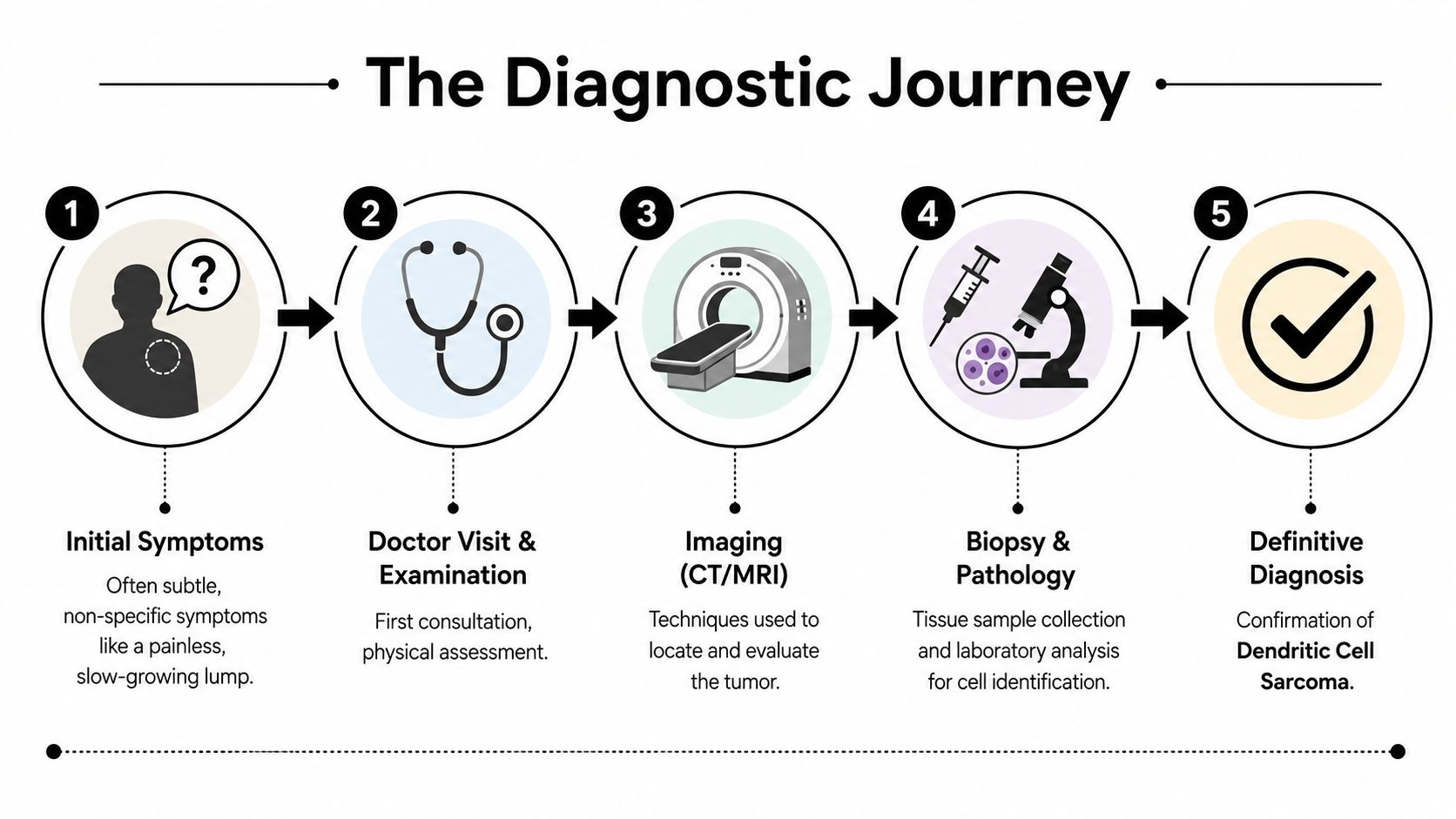
Many patients start with something that doesn't look dramatic. A lump in the neck. A fullness in the abdomen. A mass found on imaging that was ordered for another reason. Sometimes the lump is painless and slow-growing, which can make it easy to delay evaluation.
That pattern is one reason dendritic cell sarcoma can be hard to identify early. A rare tumor doesn't announce itself by saying it's rare. It often looks, at first, like one of many more common problems.
What usually happens first
A doctor begins with the basics. They ask how long the mass has been there, whether it has changed, and whether you've had symptoms such as pain, pressure, weight loss, or fatigue. Then comes the physical exam, which helps determine whether the mass seems superficial, fixed, enlarged, or associated with nearby lymph nodes.
After that, imaging helps answer practical questions:
- Where is the tumor located
- How large is it
- Is it pressing on nearby structures
- Does it appear localized or more widespread
A CT or MRI gives the map. If there's concern about spread, staging scans may be added. Imaging can suggest the problem, but it usually can't name the tumor with certainty.
Later in the process, many families find it helpful to keep their paperwork organized. If you're gathering reports from several offices, a practical walkthrough on filling out your medical records form can make it easier to collect pathology, imaging, and consultation notes in one place.
Why the biopsy matters so much
The biopsy is the turning point. It gives the pathologist actual tissue to study. That's how the team moves from “this looks suspicious” to “this is the specific tumor we're dealing with.”
Under the microscope, FDCS can mimic other spindle-cell neoplasms. That's why pathologists don't rely on appearance alone. They use immunohistochemistry, often shortened to IHC. I tell patients to think of these stains as special keys being tested in a lock. A general stain may tell you the tumor is abnormal. A lineage-defining stain helps show what type of cell it came from.
For FDCS, the most useful markers are CD21, CD23, and CD35, and using that focused panel helps reduce misdiagnosis risk because the tumor can resemble other cancers (pathology review of FDCS immunohistochemistry and morphology).
When the diagnosis is rare, the biopsy doesn't just confirm cancer. It identifies the cancer's lineage, and that changes everything that follows.
The tissue pattern can also provide clues. Pathologists may describe spindled-to-ovoid cells arranged in fascicles, storiform arrays, whorls, diffuse sheets, or vague nodules. Those words sound technical, but they serve a useful purpose. They tell the pathologist when to stop and ask, “Could this be FDCS?”
What patients should ask for
Once the pathology comes back, ask for the actual report and ask someone to walk through it with you in plain language. If you'd like a patient-friendly primer before that discussion, this guide on how to read a pathology report can help you make sense of terms such as margins, markers, mitotic activity, and necrosis.
A few questions are especially useful:
- Was the diagnosis reviewed by a pathologist familiar with rare sarcomas?
- Which immunohistochemical markers were positive?
- Is this definitely FDCS, or is there still uncertainty?
- Do the pathology features suggest a slower or more aggressive pattern?
That last question matters because treatment planning depends on more than the tumor's name. It depends on the details inside the report.
A short video can also help you understand how doctors move from suspicion to confirmation.
How Staging Guides Your Treatment Plan
Staging answers a practical question: Is this cancer confined to one area, or has it spread? For dendritic cell sarcoma, that question shapes whether treatment can focus mainly on local control, such as surgery, or whether the plan needs to address disease that may be more extensive or biologically aggressive.
Patients sometimes hear “indolent” and assume the situation is low-risk. That can be misleading. Some cases do behave more slowly, but doctors also look for features that signal a much tougher course.
What doctors are actually assessing
Staging involves more than assigning a label. Your team is combining information from scans, the biopsy, the pathology report, and the physical exam. They want to know:
- Size of the tumor
- Where it started
- Whether it invades nearby tissue
- Whether lymph nodes or distant organs are involved
- Which microscopic high-risk features are present
SEER notes that FDCS is often an indolent sarcoma, but tumors with significant cytologic atypia, extensive coagulative necrosis, a high proliferative index, size greater than 6 cm, or intra-abdominal location can follow a rapidly fatal course. The same summary also emphasizes complete surgical excision as the main treatment for most patients, with consideration of adjuvant chemotherapy and/or radiotherapy for deep, large, tissue-invasive, unresectable, or otherwise high-risk disease (SEER summary of FDCS prognosis and treatment approach).
How that changes decisions
A small, localized tumor in a favorable location raises different questions than a deep abdominal mass involving nearby structures. In the first situation, the team may focus on whether surgery can remove the disease completely. In the second, they may need to plan for a broader strategy that includes additional therapy or a staged approach.
Here's the key logic:
| Staging factor | Why it matters in planning |
|---|---|
| Localized disease | May support a surgery-first strategy if safe and feasible |
| Intra-abdominal location | Raises concern for more aggressive behavior and more complex surgery |
| Larger tumor burden | Can increase concern about recurrence and need for multimodality planning |
| High-risk pathology features | May push the team to discuss treatment beyond surgery alone |
Staging is not a grade on how “bad” your cancer is. It's a map for choosing the right intensity of treatment.
Specialized review offers the greatest help to families. The staging workup turns a frightening diagnosis into a plan with sequence and purpose.
Exploring Your Treatment Options for Dendritic Cell Sarcoma
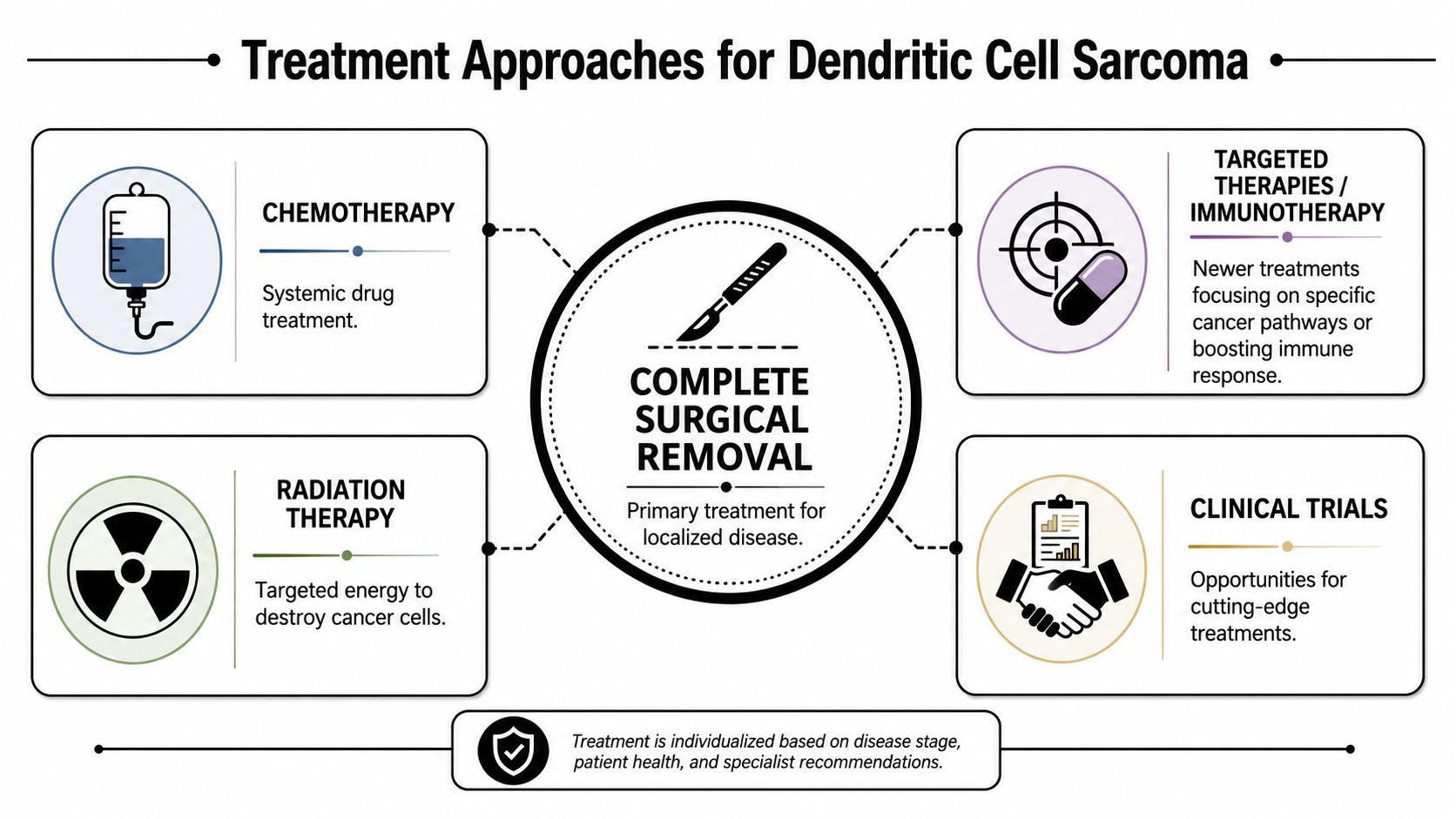
A family often arrives at this point with one urgent question: “What happens now?” For dendritic cell sarcoma, the answer usually comes from building a treatment plan in layers. The team first looks at what can be removed, then at what might need to be treated beyond the operating room, and then at whether the tumor's biology suggests a more personalized approach.
For many patients, surgery remains the center of that plan if doctors believe the tumor can be removed safely and completely. Surgery works like removing the visible roots of a weed. The goal is to take out all known disease while protecting nearby organs, nerves, and blood vessels as much as possible.
Surgery when the disease is localized
Published reviews and case series consistently describe surgery as the main treatment for localized follicular dendritic cell sarcoma, especially when complete resection is possible, as summarized in the SEER hematopoietic and lymphoid neoplasm database entry on FDCS.
That does not mean every operation is straightforward. A small lymph node tumor in an accessible area is very different from a mass deep in the abdomen, chest, or pelvis. In those more complex settings, the surgeon is asking two questions at once. Can the tumor be removed, and what will that surgery cost in terms of recovery, organ function, and long-term quality of life?
These are useful questions to bring to your visit:
- Is complete removal realistic
- What nearby structures could affect the operation
- Would surgery be the first step, or part of a sequence
- What would recovery likely look like for me
Radiation and chemotherapy in selected situations
Radiation may be discussed when the tumor sits in a place where local recurrence would be hard to treat, or when the surgical margin is close and the team wants added local control. In plain language, radiation is often used to clean up microscopic cells that surgery cannot see.
Chemotherapy is considered more often when the disease cannot be fully removed, has returned, has spread, or shows features that make the team worry surgery alone may not be enough. Because this cancer is rare, doctors often borrow from sarcoma and lymphoma treatment experience, then adjust based on the patient's pathology, overall health, and prior treatment history.
That uncertainty can feel unsettling. It also explains why specialist review matters so much. In rare cancers, the right plan is often less about following a rigid script and more about matching the treatment intensity to the true behavior of the tumor.
Options beyond surgery for advanced disease
Advanced FDCS still has treatment options. A review of published cases reported temporary responses to systemic chemotherapy in a meaningful portion of patients with advanced disease, and a genomic analysis identified homologous recombination-related alterations that may support biomarker-driven strategies such as PARP inhibition in selected unresectable cases (review of advanced FDCS treatment experience and molecular findings).
That matters because it changes the conversation from “there is no standard” to “we need a careful, individualized plan.” Those are not the same thing. One sounds like a dead end. The other points toward second opinions, molecular testing, and thoughtful use of available therapies.
A useful way to picture advanced treatment is to separate the goals:
- Control the known tumor burden with surgery, radiation, or drug therapy when possible.
- Treat disease that may be elsewhere in the body with systemic therapy.
- Look for tumor-specific clues through pathology review and molecular profiling that could widen the options.
Where immunotherapy and clinical trials fit
Because standard protocols are limited, patients should ask whether referral to a sarcoma center, repeat pathology review, broader molecular profiling, or a clinical trial makes sense. Some teams also discuss immunotherapy in selected cases, especially when conventional options are limited or the tumor's biology suggests a reason to consider it. If you want a plain-language overview before that discussion, this guide to what immunotherapy for cancer is can help.
One practical option patients in New York may explore is Hirschfeld Oncology, an outpatient oncology practice and infusion center that offers individualized cancer care approaches, including immunotherapy-based strategies and customized regimens for complex cases. It does not replace sarcoma specialty input or clinical trial evaluation. It is one example of the kind of patient-centered setting where detailed treatment discussions can happen with time, support, and coordination.
If the choices feel unclear, return to the core question. What is this treatment trying to accomplish for you right now: remove the cancer, reduce the chance of return in one area, control disease throughout the body, or buy time while your team gathers more information? Once that purpose is clear, the plan usually becomes easier to understand, and easier to live with.
Prognosis and Managing Life During and After Treatment
A common moment after treatment sounds like this: the scan is done, the operation or chemotherapy is over, and everyone asks the same question. What happens now?
With dendritic cell sarcoma, prognosis is rarely a simple yes-or-no answer. Because this cancer is uncommon, published outcomes come from small case series and retrospective reviews. Those reports are useful for setting expectations, but they are not a forecast for one specific person. Your age, where the tumor started, whether it was fully removed, and whether disease is limited to one area or has spread all shape what comes next.
One point is consistent across studies of follicular dendritic cell sarcoma. Recurrence can happen, including after treatment that initially appears successful. That is why follow-up care is not just waiting for the next scan. It works more like routine radar after a storm. The goal is to spot a problem early, while there are still options to address it.

What prognosis means in real life
Patients often hear terms like disease-free survival and overall survival and wonder if they mean the same thing. They do not.
Disease-free survival asks how long someone remains without visible return of the cancer after treatment. Overall survival asks how long people are alive, even if the disease returns and needs more therapy. For families, that difference matters. A recurrence is serious, but it does not automatically mean there are no next steps.
That is also why your oncologist may talk about prognosis in layers instead of one number. First comes cancer control. Then function. Then recovery. Then the long stretch of living with surveillance and uncertainty. Each layer affects daily life in a different way.
The follow-up plan matters because it turns uncertainty into a schedule
After active treatment, many people feel more anxious, not less. During treatment, there is a calendar, a purpose, and a team checking in often. After treatment, the quiet can feel unsettling.
A written surveillance plan helps. Ask your team:
- How often will I need scans or exams?
- What symptoms should prompt a call right away?
- If something changes, who should coordinate the next step?
- What side effects from surgery, radiation, or chemotherapy should I still expect months later?
Those questions sound simple, but they reduce confusion. They also help families tell the difference between expected recovery and warning signs that need attention.
Managing life during recovery and long-term follow-up
Recovery is not only about whether the tumor is gone. It is also about how your body and mind are functioning. If the tumor involved the abdomen, eating, bowel habits, or fullness may remain part of the conversation. If surgery affected movement or strength, physical therapy may matter as much as the next scan. If treatment caused fatigue, that fatigue deserves treatment too.
Small routines help more than people expect. Regular meals. Short walks. Sleep habits. A notebook for symptoms and questions. These are not minor details. They are part of cancer care because they affect strength, mood, and the ability to tolerate whatever comes next.
Some patients also benefit from asking whether tumor profiling could clarify future options if the disease returns. A plain-language overview of how precision oncology connects tumor biology to treatment choices can make those conversations easier to follow.
Hope comes from having a plan, not from pretending the risk is small
Hope in a rare sarcoma is not false reassurance. Hope comes from knowing what your team is watching, what symptoms matter, and what the backup options might be if the disease comes back. It also comes from being treated as a whole person, not just a pathology report.
That kind of care is easier when communication is clear and follow-up feels organized. Even an outside-facing guide for healthcare practices highlights something patients feel immediately: coordinated, humane care reduces confusion at the moments when families are already carrying too much.
The goal after treatment is not to live in fear of the next scan. It is to build a life that includes follow-up, recovery, and support, while keeping room for ordinary days again.
Why Expert Personalized Care Matters for Rare Sarcomas
Rare cancers expose the limits of generic oncology. When the disease is uncommon and standard protocols are thin, patients benefit most from teams that are comfortable with ambiguity, willing to review pathology carefully, and able to tailor treatment rather than forcing the case into a template.
That's the core value of personalized care. It doesn't mean experimental for the sake of being experimental. It means matching the plan to the tumor's location, pathology, stage, symptoms, and the patient's own goals. For some people, that means aggressive local control. For others, it means balancing disease control with function and quality of life. For still others, it means exploring biomarker-driven treatment or trial options.
Patients also notice the difference in how care is delivered. Clear communication, coordinated records, and responsive follow-up matter more in rare cancers because every handoff creates room for confusion. This guide for healthcare practices offers a useful outside perspective on the systems and habits that can make care feel more understandable and humane.
If you're weighing advanced treatment options, it may also help to learn how precision oncology connects tumor biology to individualized therapy choices. That mindset is especially relevant when standard pathways are limited.
If you or a loved one is facing dendritic cell sarcoma and want help making sense of pathology, staging, and treatment options, Hirschfeld Oncology offers consultations for patients seeking individualized cancer care. A careful review of records, symptoms, prior treatment, and possible next steps can help you move from uncertainty toward a plan that fits your specific situation.
.png)
.png)




