




.png)


It’s one of the first questions that comes up after a cancer diagnosis: Will chemotherapy make me infertile? The honest answer is, it might. But it’s never a given.
For some, the effects are temporary. For others, they can be permanent. The outcome really boils down to your specific treatment plan, your age, and your overall health before starting. Understanding your personal risk is the first step to feeling in control and making decisions you’re confident in.
Your Guide to Chemotherapy and Fertility Risks

When you're facing cancer, the last thing you need is more uncertainty, especially around something as personal as your ability to have children. That’s why we want to cut through the confusion and replace fear with facts.
Think of this as your starting point for a critical conversation with your oncology team. We’ll walk through the main variables that determine your risk so you can approach those discussions with clarity and confidence.
The Main Factors Influencing Your Risk
Your individual risk isn't based on one single thing. Instead, it’s a combination of several factors that, together, create a unique picture of how your body might respond to treatment. We’ll get into the specifics of each of these later, but it’s helpful to see the big picture first.
Here’s a high-level summary of the main factors that determine how chemotherapy might impact your fertility.
Quick Guide to Chemotherapy and Fertility Risk Factors
Knowing these variables gives you a framework for understanding your own situation. It turns a big, overwhelming question into specific, manageable points you can go over with your doctor, ensuring you can advocate for your future family-building goals.
How Chemotherapy Impacts Male and Female Fertility
To understand whether chemo can affect your ability to have children, it helps to know what’s happening inside your body during treatment. The impact on fertility isn't the same for men and women, so let's walk through what you can expect.
Chemotherapy is designed to be a powerhouse against rapidly dividing cells. That's fantastic for fighting cancer, but the medicine can’t always tell the difference between a cancer cell and other healthy, fast-growing cells—like the ones crucial for reproduction. We cover this in more detail in our guide on how chemotherapy works.
The Impact on Female Fertility
For women, a good way to think about your ovaries is like a bank account that holds all the eggs you'll ever have. You're born with this "account"—your ovarian reserve—and you can only make withdrawals over your lifetime, never new deposits.
Certain chemotherapy drugs can act like a thief, making large, unplanned withdrawals from this account. This can cause two distinct problems:
- It can reduce the number of eggs. The treatment might destroy a large portion of your eggs, leaving your "account balance" much lower than it should be.
- It can damage the quality of remaining eggs. Even the eggs that survive the treatment might be damaged, making it harder for them to lead to a healthy pregnancy down the road.
This damage can trigger premature ovarian insufficiency or even early menopause, which effectively shortens the window you have to conceive. The risk really depends on the specific chemo drugs used and your age during treatment—younger women generally start with a higher ovarian reserve, offering a bit more of a buffer.
The Impact on Male Fertility
For men, the story is a bit different. Picture the testes as a factory that is constantly manufacturing new sperm. Unlike the fixed number of eggs in women, this factory is built for continuous, non-stop production.
Chemotherapy can throw a major wrench in this factory's assembly line. The drugs are especially tough on the spermatogonial stem cells, which are the "master cells" that kick off the entire sperm production process. When these critical stem cells are damaged or wiped out, the factory's output can grind to a halt.
This can lead to oligospermia (a very low sperm count) or, in more severe cases, azoospermia (the complete absence of sperm). For some men, the factory shutdown is temporary, and production slowly ramps back up months or years after treatment. For others, the damage is permanent, and the factory unfortunately never reopens.
Evidence shows that male cancer survivors can face significant fertility hurdles from chemotherapy. In one landmark study, by the time they reached age 45, only 50% of male childhood cancer survivors had been able to father a child, compared to 80% of men who hadn't had cancer. This stark difference really drives home the profound and lasting impact chemo can have. You can read the full study from the Fred Hutchinson Cancer Research Center to learn more.
Knowing how these treatments work is the first step toward having an informed conversation with your doctor about your personal risks and the steps you can take to protect your future.
Of course. Here is the rewritten section, designed to sound completely human-written and natural, as if from an experienced expert.
Your Personal Risk: What Does This Mean for Me?
It’s one thing to talk about general risks, but the only question that really matters is, "How will chemotherapy affect my ability to have children?" The truth is, there’s no single answer. The impact on your fertility is deeply personal, and it comes down to a few key factors: your age, the specific drugs in your treatment plan, and the total dose you receive.
Think of it like a combination lock. Each of these elements is a number in the sequence, and together they determine your individual risk. Getting a clear picture of these factors is the first step in having a productive conversation with your oncologist and turning worry into a concrete plan.
Age: The Starting Point for Your Fertility
Your age when you begin treatment is probably the single most important factor. Younger patients—both men and women—simply have more to work with. Women start with a larger ovarian reserve (a greater number of eggs), and men have more robust sperm production. This gives your body a bigger buffer, making it more likely your reproductive system can weather the treatment and bounce back.
If you’re older when starting chemotherapy, you're beginning with a naturally smaller reserve. That smaller buffer means your reproductive system is more vulnerable to the damage chemo can cause, and the odds of a full recovery are lower.
The Drugs: Which Ones Carry the Most Risk?
Not all chemo is created equal when it comes to fertility. Some drugs are known to be particularly harsh on the ovaries and testes, while others have a much lower risk profile. The specific drug, or cocktail of drugs, in your plan is a critical piece of the puzzle.
To give you a better sense of this, we've broken down some common chemotherapy drugs by their general risk level.
Chemotherapy Drug Risk Levels for Fertility
This table is a guide to help you understand where your prescribed treatment might fall. Remember, it's a starting point for a conversation with your doctor, not a final diagnosis.
Your oncologist can explain exactly what this means for you, based on the unique combination and dosage they have planned for your treatment.
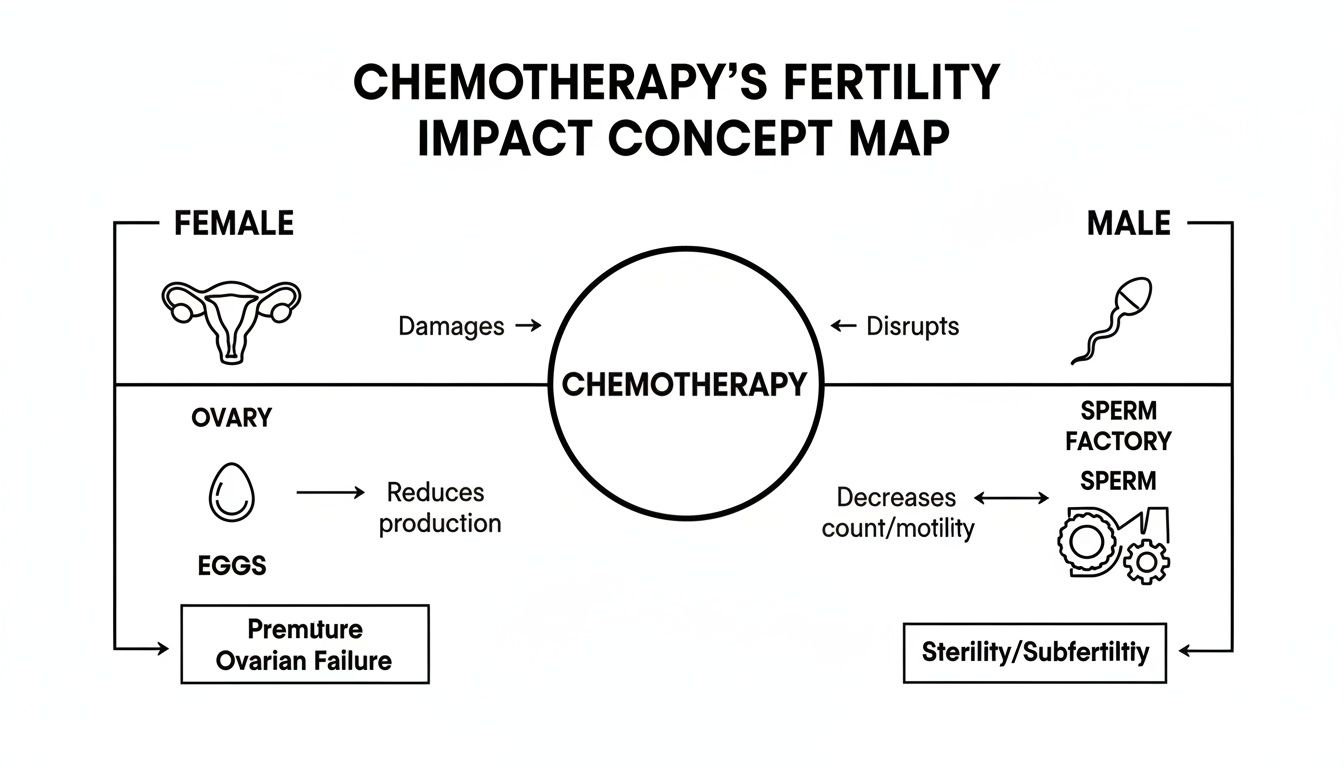
As you can see in the diagram below, these drugs work in different ways to impact the reproductive system—either by depleting a woman's finite supply of eggs or by interrupting the constant production of sperm in men.
The Dose: How Much and for How Long?
Finally, it’s not just which drug you receive, but the total amount you get over time. This is what we call the cumulative dose. Higher total doses and longer treatment schedules increase the likelihood of lasting damage to your reproductive organs.
It’s a bit like sun exposure. A few minutes in the sun is harmless, but spending hours in it day after day greatly increases your risk of a serious burn. In the same way, the cumulative effect of chemotherapy can eventually overwhelm your body's natural ability to repair itself.
It's critical to understand that even if fertility seems to return after treatment, the window for having children may be much shorter. A woman's period might come back, but her underlying egg supply is almost always diminished.
For instance, a powerful UCSF study on Hodgkin's disease survivors highlighted this perfectly. The rate of infertility jumped from 18% for women diagnosed at age 20 to a staggering 57% for those diagnosed at 35. This was true even for women who didn't experience immediate ovarian failure. You can discover more about these UCSF study findings and see just how closely age and treatment are linked.
The Critical Role of Radiation Therapy
While chemotherapy is a systemic treatment that travels throughout your entire body, radiation therapy is a different beast entirely. It’s a targeted, high-energy attack aimed squarely at a specific area. If chemotherapy is like a widespread storm, you can think of pelvic radiation as a direct lightning strike.
When that lightning strike is aimed at the pelvic region—where the ovaries, uterus, and testes live—the damage to fertility can be swift and severe. This concentrated energy can destroy a woman's eggs, a man's sperm-producing cells, and even harm the uterus itself, making it difficult to carry a pregnancy down the road.
Direct Damage to Reproductive Organs
With radiation, its impact on fertility all comes down to two things: location and dose. Unsurprisingly, treatment directed at or near the pelvis poses the greatest threat.
- For Women: Radiation to the ovaries can effectively wipe out the egg supply, triggering premature ovarian failure and early menopause. If high doses hit the uterus, it can cause scarring and reduce vital blood flow. This might prevent a fertilized egg from implanting or make it impossible for the uterus to support a growing baby.
- For Men: When radiation is aimed at the testes, it can destroy the delicate stem cells that are responsible for making sperm. This can cause sperm counts to plummet or stop production altogether, resulting in permanent infertility.
The dose makes a massive difference. Pelvic radiation is considered the highest-risk cancer treatment for infertility, with measurable damage starting at doses as low as 2 Gray (Gy). Doses over 24 Gy, research shows, almost always cause permanent infertility in younger patients.
In fact, a major German study found that pelvic radiotherapy was the single biggest risk factor for infertility among childhood cancer survivors, increasing the odds by a staggering 20 times. You can discover more about these radiotherapy findings to understand the data.
Indirect Effects on Fertility
Even when radiation isn't aimed anywhere near your pelvis, it can still throw a wrench into your reproductive system. A perfect example is cranial radiation, which is radiation therapy directed at the brain.
Your brain contains the pituitary and hypothalamus glands—the command center for your body's entire hormonal network. These glands send out the signals that tell the ovaries and testes what to do and when. Radiation to this command center can scramble those signals, leading to hormonal chaos that shuts down reproductive function.
Think of it like the power going out at the main control tower. Even if the factory (the ovaries or testes) is in perfect working order, production grinds to a halt without instructions from headquarters.
This hormonal disruption can stop periods in women and sperm production in men, creating a state of infertility that may be temporary or, in some cases, permanent.
To learn more about how radiation works and its broader impacts, you can check out our detailed guide on the effects of radiation therapy. Understanding both the direct and indirect risks is absolutely essential for having a complete conversation with your care team about protecting your future.
Proactive Steps to Preserve Your Fertility

Hearing that chemotherapy could affect your fertility is tough, but this is the moment to turn concern into action. You have real, effective options to protect your dream of having a family down the road. The one non-negotiable? All of this has to happen before your first treatment.
Taking this step is about more than just a medical procedure; it’s about taking back some control and making a plan for the life you want to live after cancer. By looking into fertility preservation, you’re making a powerful investment in your own future.
Fertility Preservation Options for Men
For men about to start chemotherapy, the go-to method is sperm banking, which is just a clinical term for freezing sperm (cryopreservation). It's a non-invasive and remarkably fast process that can be wrapped up in a matter of days.
Here’s what you can expect:
- Consultation: First, you’ll meet with a fertility specialist to walk through the details.
- Collection: You'll provide one or more semen samples in a private setting at the clinic. For the best results, clinics often recommend banking a few samples over several days.
- Freezing and Storage: The lab team analyzes your samples, adds a special solution to protect the sperm during freezing, and stores them in liquid nitrogen.
This method works incredibly well. Once frozen, sperm can be stored for decades without any loss of quality. Even if you’re on a tight schedule, banking just one sample can be enough to keep your options open.
Fertility Preservation Options for Women
For women, the process is more complex, but the technology is just as empowering. The two main approaches are egg freezing and embryo freezing. Both start with a process that looks a lot like the first phase of in-vitro fertilization (IVF) and need to be completed before chemo begins.
The entire timeline usually takes about 2-3 weeks from start to finish.
- Ovarian Stimulation: For about 10-14 days, you’ll give yourself daily hormone injections. These medications encourage your ovaries to mature a group of eggs at once, instead of the single egg that typically develops each month.
- Monitoring: You'll visit the clinic frequently during this period for bloodwork and ultrasounds. This is how your specialist tracks the follicles (the sacs that hold the eggs) and fine-tunes your medication dosage.
- Egg Retrieval: When the eggs are ready, you’ll have a minor procedure. It’s done under light sedation, so you’ll be comfortable. A doctor uses a thin, ultrasound-guided needle to collect the eggs from your ovaries, which usually takes less than 30 minutes.
From there, it’s your choice. The retrieved eggs can be frozen on their own (oocyte cryopreservation), or they can be fertilized with sperm from a partner or a donor to create embryos, which are then frozen (embryo cryopreservation).
The decision between freezing eggs or embryos is deeply personal. Egg freezing gives you more future flexibility if you aren’t sure about a partner. Embryo freezing historically had a slight edge in success rates, but modern egg-freezing technology has dramatically closed that gap.
As you consider these paths, it can be helpful to learn about other ways to support your body's health, such as preparing your body for IVF in the weeks leading up to your procedure.
The Urgency of Timing
With any of these preservation methods, timing is everything. The entire process—from consultation to freezing—has to be finished before your first infusion of chemotherapy or your first radiation session. Once treatment is underway, it’s often too late to collect healthy eggs or sperm.
This is why you need to bring this up with your oncologist as soon as your treatment plan is discussed. Ask them for an immediate referral to a reproductive endocrinologist (a fertility specialist). Many fertility clinics have fast-track programs specifically for new cancer patients because they understand the clock is ticking. Don't wait to have this conversation.
How to Talk to Your Doctor About Fertility
A cancer diagnosis is an avalanche of information. It's completely normal to feel overwhelmed, and bringing up something as personal as fertility can feel like one more heavy thing to carry. But this conversation is one of the most important you’ll have. Taking charge of your future family options is a crucial part of your care, and the time to start is right now.
Thinking about this discussion can feel intimidating, but it doesn't have to be. The best way to cut through the noise and anxiety is to walk in prepared with a simple list of questions.
Your Essential Question Checklist
Having a few key questions written down does two things: it makes sure you don't forget to ask something vital, and it clearly signals to your care team that your long-term quality of life is a top priority. A prepared patient helps make the conversation focused and incredibly productive.
Here are the critical questions to get the dialogue started:
- What specific risk does my recommended treatment plan pose to my fertility?
- Based on my age and the drugs you've chosen, what is my personal risk profile?
- Is the potential infertility likely to be temporary or permanent?
- What is my timeline? How long do I have to pursue fertility preservation before my treatment must begin?
- Can you refer me to a fertility specialist, ideally one who has experience with cancer patients?
These questions give your oncologist a direct path to understanding what matters to you beyond the cancer itself. It opens the door for a collaborative plan that treats the whole person, not just the disease. For more ideas, check out our guide to essential questions to ask your oncologist.
Making the Referral to a Specialist
That last question on the list—the one about a referral—is your most important next step. While your oncologist is the expert on cancer, a reproductive endocrinologist is the specialist who can walk you through your preservation options, like egg, embryo, or sperm freezing. They are the experts in "oncofertility," the field that bridges cancer care and reproductive medicine.
Don’t be afraid to be direct. A simple statement like, "I want to explore my fertility preservation options. Can you give me an immediate referral to a specialist?" is powerful and gets the ball rolling quickly.
Time is absolutely critical here. Any preservation procedure must be completed before your first dose of chemotherapy or radiation. The good news is that most fertility clinics have fast-track programs for cancer patients and can often get you in for a consultation within a day or two. Your oncology team can coordinate with them to make sure this process doesn’t delay your primary treatment. By asking these questions, you become your own best advocate and ensure your future dreams are a valued part of your present care plan.
Common Questions About Chemo and Infertility
A cancer diagnosis is overwhelming, and when treatment might affect your ability to have children, the questions can feel even heavier. Let's tackle some of the tough, personal questions that come up when we talk about chemo and fertility.
We want to give you clear answers to help you understand your options and feel more prepared for conversations with your doctors.
If My Period Returns After Chemo, Does That Mean My Fertility Is Back to Normal?
This is such a hopeful sign, but unfortunately, it's not the full story. While the return of your period shows your ovaries have started to function again, it doesn’t guarantee your fertility is the same as it was before treatment.
Think of your egg supply, or ovarian reserve, like a bank account. Chemotherapy almost always forces a significant withdrawal from that account. Even when your monthly cycles restart, your "balance" of eggs is lower, which can mean you have a shorter window of time to conceive in the future.
The only way to know for sure is to get a professional assessment. A reproductive specialist can run blood tests and perform an ultrasound to get a true picture of your ovarian reserve. This evaluation will give you the real answers you need about where you stand.
Is It Too Late for Fertility Preservation if I’ve Already Started Chemo?
Don't assume you've missed your chance. While it's always best to preserve fertility before treatment starts, it isn't always too late. The answer really hinges on your specific chemotherapy drugs and where you are in your treatment schedule.
In some cases, your oncologist may be able to find a safe window to pause treatment just long enough for you to go through egg, embryo, or sperm freezing. Whether this is possible depends on your type of cancer, how aggressive it is, and the exact drugs you’re receiving.
You need to have this conversation with your oncology team immediately. They are the only ones who can determine if this is a safe option for you and coordinate with a fertility specialist to see what's possible. The sooner you ask, the more options you might have.
The most important thing is to speak up. Never assume it's a lost cause or that you shouldn't ask. Your medical team is there to help you navigate every part of your care, and that includes quality-of-life concerns like your future family.
How Do I Find and Pay for a Fertility Specialist?
Finding the right specialist and figuring out the costs can feel daunting, but you don't have to do it alone. Your best starting point is your own oncology team.
Oncologists and patient navigators typically have strong relationships with reproductive endocrinologists who focus on oncofertility—the specific field where cancer care and reproductive medicine meet. A direct referral from your doctor is usually the quickest path to getting an appointment.
You can also search for certified clinics and specialists through organizations like the Society for Assisted Reproductive Technology (SART).
Navigating the Costs of Preservation
Paying for fertility services is becoming more manageable, thanks to growing awareness and support.
- Insurance Coverage: Many states now require insurers to cover fertility preservation when medical treatment puts fertility at risk. It's definitely worth investigating your state's laws and the details of your specific insurance plan.
- Non-Profit Assistance: Several fantastic non-profit organizations provide grants and financial aid just for cancer patients who need to preserve their fertility.
- Clinic Programs: Don't hesitate to ask fertility clinics directly about their own financial aid programs or if they offer discounts for oncofertility patients.
Groups like The Livestrong Foundation and Team Maggie for a Cure are incredible resources for financial help. Your hospital’s social worker or patient navigator can be your best ally in finding and applying for these programs.
At Hirschfeld Oncology, we believe that complete cancer care means looking after the whole person, not just treating the disease. If you’re worried about how your treatment could affect your fertility or need help figuring out the next steps, we are here to guide you. To discuss a personalized care plan that puts your health and your future first, please request a consultation through our website.
.png)
.png)




