




.png)


If you're reading this after a scan, a biopsy, or a conversation that left you with more questions than answers, you're not alone. Many people first encounter the phrase fallopian tube cancer in the middle of a frightening week. They may have gone in for bloating, pelvic discomfort, bleeding, or a mass found on imaging, and suddenly they're hearing unfamiliar terms that sound close to ovarian cancer but not quite the same.
That uncertainty can feel especially unsettling because the name itself raises immediate questions. Where did this cancer start. Does that change treatment. Is it treated like ovarian cancer. What happens if it has already spread. And if this is recurrent or advanced disease, are there options that aren't built around feeling sick all the time.
Those are reasonable questions. They deserve clear answers.
This guide is written in the tone I use with patients and families in clinic. Plain language. Honest explanations. Enough detail to help you make sense of what you're hearing, without burying you in jargon. Some parts will focus on the newer understanding of where many so-called ovarian cancers begin. Other parts will focus on the practical realities of diagnosis, treatment, recurrence, and quality of life.
Understanding Your Diagnosis and Finding Your Footing
A new cancer diagnosis often scrambles the usual order of things. People who are normally organized find themselves forgetting questions. Family members search online late at night and end up more alarmed than informed. It's common to feel like everyone is talking fast while you're still trying to understand the first sentence.
Start with this: a diagnosis is the beginning of a plan, not the end of the story.
Fallopian tube cancer develops in the thin lining of the fallopian tube. For many patients, the early details are confusing because the symptoms can resemble other gynecologic problems, and the final answer often isn't confirmed until surgery and pathology. That doesn't mean anyone missed something obvious. It means this disease can be subtle.
What patients usually need first
Before discussing treatment, three fundamental points typically require clarification:
- What exactly was found. Was there a mass, abnormal cells, fluid, or evidence of spread.
- How sure are we. Some findings raise suspicion, but the firm diagnosis usually comes from pathology.
- What happens next. The next step may be more imaging, bloodwork, surgery, chemotherapy, or a discussion about sequencing these treatments.
Practical rule: Bring one trusted person to appointments if you can. One person listens while the other asks questions and takes notes.
A steadier way to approach the first days
Try to think in short steps instead of trying to solve the whole future in one sitting.
- Get the exact diagnosis wording from the report or doctor.
- Ask where the cancer appears to have started and whether the team believes it behaves like a high-grade serous cancer.
- Find out what decisions are urgent and what can wait a few days.
- Write down symptoms and concerns, including pain, bleeding, appetite changes, constipation, sleep problems, and fear about treatment side effects.
You don't need to know everything today. You do need a care team that explains things clearly, listens carefully, and helps you move from shock to action.
What Is Fallopian Tube Cancer A Modern View
For a long time, fallopian tube cancer was described as a rare gynecologic cancer. That older picture is no longer the whole story. Research changed the field's understanding in a major way.
According to Cleveland Clinic's overview of fallopian tube cancer, reported incidence increased 4.19-fold between 2001 and 2014, largely because doctors and pathologists recognized that many cancers once labeled ovarian originate in the fimbriae, the finger-like ends of the fallopian tube.
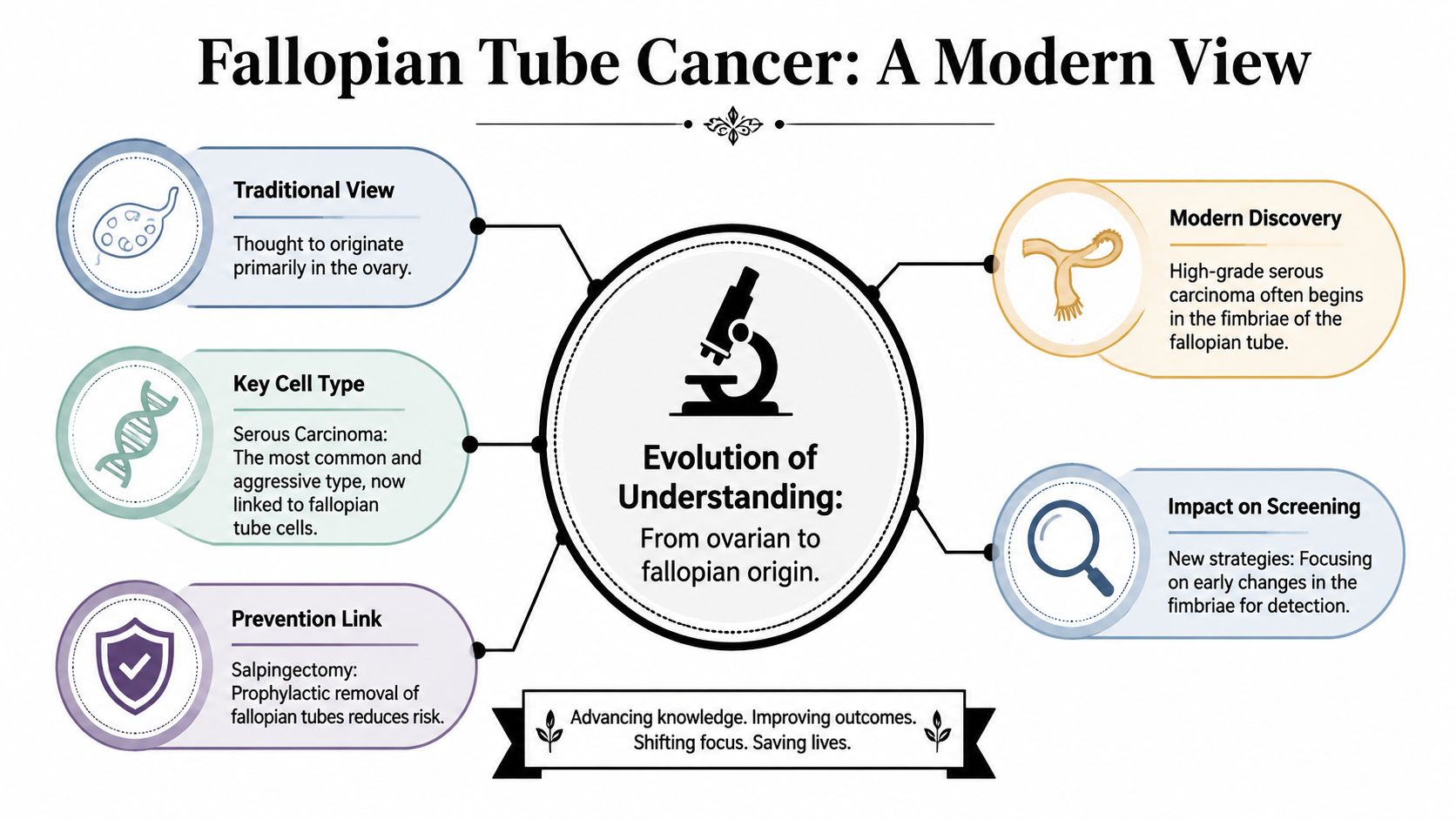
Why the fallopian tube matters so much
Think of the fimbriae as a fringe at the end of the tube, close to the ovary. In the modern view, that fringe can be the place where the first dangerous cellular changes appear. From there, cancer cells may spread to the ovary, pelvis, or abdominal lining. By the time the disease is found, it may look like "ovarian cancer" on scans or even during surgery, even though the earliest spark started in the tube.
That shift matters because origin affects how doctors think about:
- Prevention
- Pathology
- Risk-reducing surgery
- Early precancerous changes such as STIC lesions
- How patients understand their diagnosis
Many patients hear "ovarian cancer" and "fallopian tube cancer" used almost interchangeably in conversation. That's partly because these cancers often behave similarly and are often treated with similar principles. Still, origin isn't just a technical detail. It changes the story of how the disease begins.
The older definition and the newer reality
Historically, primary fallopian tube carcinoma was defined very strictly. Pathologists looked for features showing that the tumor arose from the tubal lining itself rather than spreading there from somewhere else. That older framework still matters under the microscope.
But in day-to-day oncology, the modern view has widened the conversation. A substantial share of high-grade serous cancers once grouped under ovarian cancer are now thought to arise in the fallopian tube. If you're also trying to understand how this relates to ovarian cancer care and overlap in treatment planning, that comparison can help make the terminology less confusing.
The name on a report tells part of the story. The tumor's biology, location, and pattern of spread tell the rest.
Why this changes prevention and screening conversations
When doctors suspect that many aggressive pelvic serous cancers begin in the fallopian tube, the prevention strategy naturally shifts upstream. Instead of focusing only on the ovary, doctors also think about the tube as the place where meaningful early intervention may happen.
This doesn't mean there is a simple screening test that catches every case early. There isn't. It does mean today's discussions about surgery, inherited risk, and pathology are more informed than they were years ago. For patients, that's not a small distinction. It can shape recommendations for relatives, future surgery decisions, and the meaning of a pathology report.
Recognizing Symptoms and Understanding Risk Factors
A common real-life scenario goes like this. Someone notices spotting after menopause, a heavier watery discharge, or a dull pelvic ache that keeps returning. At first, it is easy to blame stress, digestive trouble, fibroids, or normal aging. That uncertainty is one reason these cancers are often not recognized right away.

Symptoms that deserve attention
Fallopian tube cancer usually does not announce itself with one dramatic, unmistakable sign. It more often shows up as a pattern of symptoms that are persistent, unusual for you, or slowly becoming harder to ignore. Vaginal bleeding is a frequent warning sign, and abdominal or pelvic pain is also common.
Patients may notice:
- Abnormal vaginal bleeding, especially after menopause
- Pelvic or abdominal pain that does not fit their usual pattern
- Bloating or early fullness
- Watery or unusual vaginal discharge
- Pressure in the pelvis
- Changes in bowel or bladder habits
None of these symptoms confirms cancer. Many benign conditions can cause the same complaints. The key question is whether the symptom is new, unexplained, and lingering.
Postmenopausal bleeding deserves prompt medical attention every time. Even when the cause is not cancer, it should be checked.
Some families also hear the term CA-125 early in this process. If that blood test comes up in your visit, this explanation of what the CA-125 test can and cannot show can make the conversation easier to follow.
Why symptoms are easy to miss
Part of the difficulty is anatomy. The fallopian tubes are small and deep in the pelvis, so an early tumor may not cause obvious changes. Another part is the modern understanding of these cancers. Many high-grade serous cancers once labeled ovarian cancer are now believed to begin in the fallopian tube, which helps explain why the symptom pattern can feel vague and overlap with other pelvic conditions.
That can be frustrating for patients and families. You may have a strong sense that something is wrong and still not have a symptom that points neatly to one diagnosis.
Who may have higher risk
Risk factors do not predict the future with certainty. They help doctors decide who may need closer attention, genetic counseling, or a prevention discussion.
A few situations raise concern:
- A personal or family history of breast, ovarian, fallopian tube, pancreatic, prostate, or colon cancer
- An inherited mutation such as BRCA1, BRCA2, or Lynch syndrome
- A prior gynecologic cancer history
- Postmenopausal bleeding or new pelvic symptoms in someone with inherited risk
Inherited risk is especially important here because it can affect more than one decision at once. It may shape testing for relatives, the type of surgery recommended, and whether treatment choices later include targeted options that can control disease with less day-to-day toxicity for some patients.
Here's a patient education video that may help you organize the symptom picture before your next appointment.
An often missed prevention conversation
One prevention topic deserves much more attention. Opportunistic salpingectomy means removing the fallopian tubes during another planned pelvic surgery in someone who is not having surgery for a known tube cancer.
According to the National Cancer Institute's ovarian cancer prevention information, this approach can lower the risk of ovarian and fallopian tube cancer for average-risk women who are already undergoing pelvic surgery, while preserving ovarian function and hormones when the ovaries are left in place.
Many people hear "remove the tubes" and worry that menopause will start right away. In this setting, that is usually not the goal. The discussion is often about removing the tubes and keeping the ovaries, based on the growing evidence that many aggressive pelvic serous cancers begin in the tubes.
If you are already planning pelvic surgery for another reason, ask a direct question: "Should we talk about removing the fallopian tubes for cancer prevention in my situation?"
This conversation is not limited to people with a known inherited mutation. It can also apply to average-risk women who want to understand whether a preventive step makes sense during a surgery they are already having.
The Path to Diagnosis and Staging
A common first visit goes like this. Someone comes in because of bloating, pelvic pressure, or bleeding that does not feel normal. An ultrasound finds a mass or fluid. Bloodwork adds another clue. Then the hardest part begins. Waiting for enough pieces to come together so the team can say what this is, where it started, and how far it has gone.
That waiting can feel endless. It helps to know that diagnosis happens in steps because each step answers a different question.
The first clues
The process often starts with a careful history and physical exam. From there, doctors may order a transvaginal ultrasound, CT scan, or MRI, depending on the symptoms and what the exam shows. These tests can reveal a pelvic mass, thickening, fluid, or signs that cancer may have spread. They rarely prove the exact starting point on their own.
Blood tests may be part of the picture too. One of the best known is CA-125. As explained in this CA-125 blood test overview, it can support the evaluation, but it cannot confirm fallopian tube cancer by itself.

What CA-125 can and cannot tell you
CA-125 works like a smoke alarm. It may signal that something is wrong, but it cannot tell you exactly where the fire started. Some people with advanced gynecologic cancer have a high CA-125. Some with earlier disease do not. Noncancerous conditions can raise it as well.
Doctors use this test in context. They compare it with symptoms, imaging, the exam, and later, with treatment response. For many families, confusion starts here because a blood test feels as if it should give a yes or no answer. This one does not. It is a clue.
Why pathology matters so much
The clearest answer usually comes from tissue examined by a pathologist. Sometimes that tissue is obtained during surgery. In other cases, a biopsy from another area of disease helps establish the diagnosis first.
This part has become more important as our understanding has changed. Many cancers once labeled as "ovarian cancer" are now believed to begin in the fallopian tube, especially high-grade serous cancers. In practical terms, that means your team is not only asking, "Is this cancer?" They are also asking, "Where did it start?" That question can shape how the disease is described, how risk is discussed with family members, and how treatment choices are framed.
Pathology reports often answer several questions at once:
- Where the cancer most likely began
- What type of cells are present
- How abnormal and fast-growing the cells appear
- Whether cancer has entered nearby tissue or lymph channels
- Whether disease is found outside the tube or ovary
If that sounds highly technical, it is. But there is a simple idea underneath it. The pathologist is building the cancer's fingerprint.
Staging in plain language
Staging describes how far the cancer has spread. It is a map, not a prediction.
A simple way to read that map is below:
| Stage idea | What it generally means |
|---|---|
| Earlier stage | Disease appears limited to the tube, ovary, or nearby pelvic structures |
| More advanced stage | Disease is present more widely in the pelvis, abdomen, lymph nodes, or beyond |
For many patients with fallopian tube cancer, staging is confirmed during surgery because that is when the team can directly inspect the abdomen and pelvis, remove visible disease, and send tissue for careful review. In advanced or recurrent disease, staging and treatment planning often overlap. The team is trying to answer two questions at once. How extensive is the cancer, and what approach is most likely to control it while protecting day-to-day function.
That second question matters greatly. Some patients can go straight to surgery. Others benefit from starting with systemic treatment first, especially if the cancer appears widespread or if a lower-toxicity strategy is needed to stabilize symptoms and preserve strength. A thoughtful staging workup helps make those decisions with more confidence and less guesswork.
Exploring Your Cancer Treatment Options
A treatment plan often starts with a very human question. What gives this patient the best chance of controlling the cancer while preserving strength, comfort, and daily function?
That question matters because fallopian tube cancer is now understood differently than it once was. Many cancers long labeled "ovarian" appear to begin in the fallopian tubes, especially high-grade serous cancers. In practice, that means treatment often follows principles used across these closely related gynecologic cancers, while still being individualized for each patient.
Standard treatment often begins with surgery and chemotherapy
For many patients, treatment includes surgery, chemotherapy, or both in sequence. Surgery is used to remove as much visible cancer as possible and to confirm exactly what type of cancer is present. You may hear the terms cytoreduction or debulking. They both refer to the same basic goal: leaving behind as little visible tumor as possible so the next treatment has less disease to chase.
Chemotherapy often includes carboplatin and paclitaxel. These medicines circulate through the body, treating cancer cells that surgery cannot see. Some patients have surgery first and chemotherapy after. Others start with chemotherapy because the cancer appears too widespread for an effective first operation, or because their body needs a gentler first step before major surgery.
The sequence matters. Two patients can have the same diagnosis on paper and still need different first moves.
How doctors decide what comes first
Families are often surprised that the decision is not "Which treatment is best?" The question is, "Which treatment should come first, and why?"
Doctors put several clues together. Imaging shows where the cancer appears to be. Blood tests such as CA-125 can add context, although they do not make decisions by themselves. Very high preoperative CA-125 levels can suggest a heavier disease burden in some advanced cases, which is one reason a team may consider chemotherapy before surgery rather than forcing an operation that is unlikely to remove enough tumor. Physical exam findings, symptoms, and sometimes laparoscopy also help shape that call.
A helpful comparison is road repair. If a few damaged sections can be fixed cleanly, surgery may come first. If the damage is spread across a wider area, it can make more sense to reduce the burden first and then operate under better conditions.
A simple way to think about treatment goals
| Treatment Type | Primary Goal |
|---|---|
| Surgery | Remove visible disease and confirm the diagnosis |
| Chemotherapy | Treat cancer cells throughout the body |
| Targeted therapy | Match treatment to tumor biology when appropriate |
| Immunotherapy | Help the immune system respond in selected situations |
| Supportive and palliative care | Reduce symptoms and protect day-to-day function during any phase of care |
Targeted therapy and more individualized treatment
Targeted therapy is more specific than standard chemotherapy. Instead of attacking fast-growing cells broadly, it aims at a weakness the cancer depends on. That weakness may come from the tumor itself or from an inherited mutation found on genetic testing.
This is one reason molecular testing matters so much in advanced or recurrent disease. It can identify whether a tumor may respond to a more individualized plan, including maintenance treatment or a drug chosen for a particular mutation or pathway. If you want to understand how research studies fit into those choices, this guide to cancer clinical trials and treatment options can help.
For patients and families, the practical question is simple. Does this treatment fit the biology of the cancer and the realities of the patient's life?
Lower-toxicity options matter in advanced and recurrent disease
Advanced or recurrent disease often brings a different set of priorities. Cancer control still matters, but so do stamina, appetite, nerve function, bowel function, sleep, and the ability to remain present for daily life.
That is why good treatment planning is not about choosing the strongest-looking regimen on paper. It is about choosing an approach a patient can live with. Sometimes that means a standard combination. Sometimes it means adjusting dose or schedule. Sometimes it means selecting a treatment with a lighter side-effect burden because prior therapy has already caused neuropathy, fatigue, low blood counts, or other limits.
This patient-centered approach is especially important in outpatient oncology settings that care for people with recurrent disease over time. Close follow-up can catch small problems before they become bigger ones. A drop in appetite, dehydration, pain, or constipation may sound minor in isolation, but together they can derail treatment if nobody addresses them early.
Supportive care also includes physical recovery. After pelvic surgery, chemotherapy, or long stretches of inactivity, some patients benefit from expert pelvic floor care as part of broader symptom support.
Immunotherapy and newer options
Immunotherapy is not used for every case of fallopian tube cancer. Its role depends on the tumor's molecular features and the broader clinical picture. In selected patients, testing may show a reason to consider an immune-based treatment or another newer option.
The key idea is fit. A newer drug is useful only when there is a clear reason to expect benefit and an honest plan for monitoring side effects. In some cases, the best progress comes from a new therapy. In others, it comes from using established treatments in a more precise, more tolerable way.
Palliative care supports treatment at every stage
Palliative care is medical care focused on symptoms, stress, and quality of life. It can be added at diagnosis, during chemotherapy, after recurrence, or alongside active cancer treatment.
It helps with pain, nausea, constipation, fatigue, anxiety, sleep problems, and hard family conversations. It also helps patients clarify their goals when choices become complicated.
Many families hear the term and worry it means treatment is stopping. In reality, palliative care often helps patients stay on treatment more comfortably and more safely. That is a meaningful part of cancer care, especially when the road is long.
Survivorship Clinical Trials and Looking Ahead
Life after diagnosis isn't divided neatly into "treatment" and "done." Many patients live in a middle space that includes surveillance, side effect management, fear of recurrence, and rebuilding daily life around a changed body.
That phase deserves just as much attention as the original treatment plan.
The physical side of survivorship
After treatment, some people are surprised by what lingers. Fatigue may hang on. Neuropathy may make fingers or feet feel numb, tingling, or clumsy. Digestion, sleep, sexual health, and pelvic comfort may all need active support.
Rehabilitation can help more than patients expect. For pelvic pain, weakness, pressure, or recovery after gynecologic treatment, expert pelvic floor care may be a useful supportive resource to discuss with your team.
The emotional side is medical too
Many patients look "fine" to other people while carrying constant uncertainty internally. Scan anxiety, body image changes, grief, intimacy concerns, and the strain on caregivers are real parts of survivorship.
A few signs that extra support may help:
- Persistent fear that crowds out daily life
- Trouble sleeping because of recurrence worry
- Withdrawal from family or normal routines
- Feeling numb, irritable, or emotionally flat for long stretches
These concerns aren't separate from cancer care. They are part of it.
You don't have to wait until you're falling apart to ask for counseling, symptom support, or help coping.
Monitoring and recurrence planning
Follow-up care usually includes ongoing visits, symptom review, and testing chosen by your oncology team. The purpose is not only to look for recurrence, but also to understand recovery, treatment effects, and new problems early.
If recurrence happens, that doesn't erase prior progress. It means the treatment strategy needs to be reconsidered. Some recurrent cancers still respond meaningfully to therapy. Others require a shift toward symptom relief, lower-toxicity disease control, or a trial-based option.
Clinical trials as a forward path
Clinical trials should not be viewed only as a last resort. They can be a proactive way to access emerging therapies and contribute to better treatment for future patients. If you'd like a patient-friendly overview of how studies work, who may qualify, and what informed consent really means, this guide to cancer clinical trials is a helpful starting point.
Trials aren't right for everyone. But they are worth discussing earlier than many people realize, especially in advanced or recurrent disease where standard options may offer diminishing returns.
Partnering with Your Care Team and Finding Resources
The most important member of the care team is the person living with the cancer. That's not a motivational slogan. It's a practical truth. You are the one experiencing the symptoms, the side effects, the trade-offs, and the goals that matter most.
The best treatment plan isn't just medically sound. It is also aligned with what matters to you.
Questions worth bringing to your next visit
Some patients freeze during appointments because they don't know where to begin. A written list helps. You don't need to ask every question at once, but these are useful starting points:
- About the diagnosis. "Where do you think this cancer started, and how confident are you about that?"
- About the goal. "Is the goal to cure, control, shrink, or relieve symptoms?"
- About the plan. "Why are you recommending surgery first, chemotherapy first, or another sequence?"
- About side effects. "Which side effects are most likely with this treatment, and which ones should trigger a call right away?"
- About daily life. "How might treatment affect work, caregiving, eating, sleep, and mobility?"
- About recurrence. "If this treatment stops working, what would the next options be?"
- About genetics. "Should I have genetic counseling or testing, and should family members know anything specific?"
- About support. "Who helps with pain, nutrition, emotional support, and practical issues?"
Tools that make communication easier
Patients often do better when they can review plain-language education between visits and keep track of their questions. Some clinics now use digital patient engagement tools for clinics to organize education, reminders, and follow-up communication in a way that's easier for patients and caregivers to manage.
That kind of support doesn't replace a doctor. It makes the relationship work better by helping patients absorb information at a human pace.
A strong oncology partnership should leave you better informed after each visit, not more confused.
If you're seeking another opinion, that's reasonable. If you need a team to explain the same issue twice, that's reasonable too. Good care includes clarity, patience, and room for your questions.
If you or a loved one is facing fallopian tube cancer, ovarian cancer, or recurrent gynecologic cancer and want a thoughtful discussion of advanced, lower-toxicity treatment options, Hirschfeld Oncology offers patient-centered guidance, outpatient infusion care, and consultation for complex cases in New York City.
.png)
.png)




