




.png)


A lot of people reach this decision at a moment when they're already overloaded. You may have just heard that you need a mastectomy. You may be trying to absorb pathology reports, treatment timing, work plans, and family logistics, and then someone adds another major question: reconstruction.
For many patients, that's when the room starts to feel smaller. You're asked to make choices about a body that may not feel predictable right now, and the words used in clinic can sound technical and distant. What most people want is simpler. What will I look like? What will feel most like me? What will still make sense years from now?
Navigating Your Breast Reconstruction Journey
A patient might say it this way: “I understand why I need cancer treatment. I'm less sure how to choose what comes after.” That's a very reasonable place to be. Reconstruction isn't only about shape. It's about comfort, identity, recovery, clothing, intimacy, and the practical rhythm of daily life.
Some people know immediately that they want to use their own tissue if possible. Others begin by assuming an implant will be the only option, then learn there are reconstructive approaches that use living tissue from another part of the body. Still others worry they won't be a candidate because they've had prior surgery, radiation, or a body type that doesn't fit the “usual” examples they've seen online.
The right reconstruction choice isn't the one that sounds most advanced. It's the one that fits your anatomy, your treatment plan, and the life you want to return to.
That's why the “why” matters so much. A flap procedure is often chosen not because it is simpler, since it usually isn't, but because some patients want a breast reconstruction that feels softer, behaves more like natural tissue, and may better match their long-term goals. For people navigating survivorship concerns beyond surgery, resources on breast cancer survivorship can also help frame the bigger picture.
Families often ask what they should focus on during consultations. A good starting point is this short list:
- Your priorities: Do you care most about avoiding implants, achieving a softer feel, limiting donor-site scars, or reducing future maintenance?
- Your treatment context: Have you had or will you need radiation? Prior abdominal surgery? Ongoing systemic therapy?
- Your tolerance for recovery: Flap reconstruction can offer meaningful benefits, but it asks more from you up front.
When you understand the reason behind the recommendation, the options become less abstract and more personal.
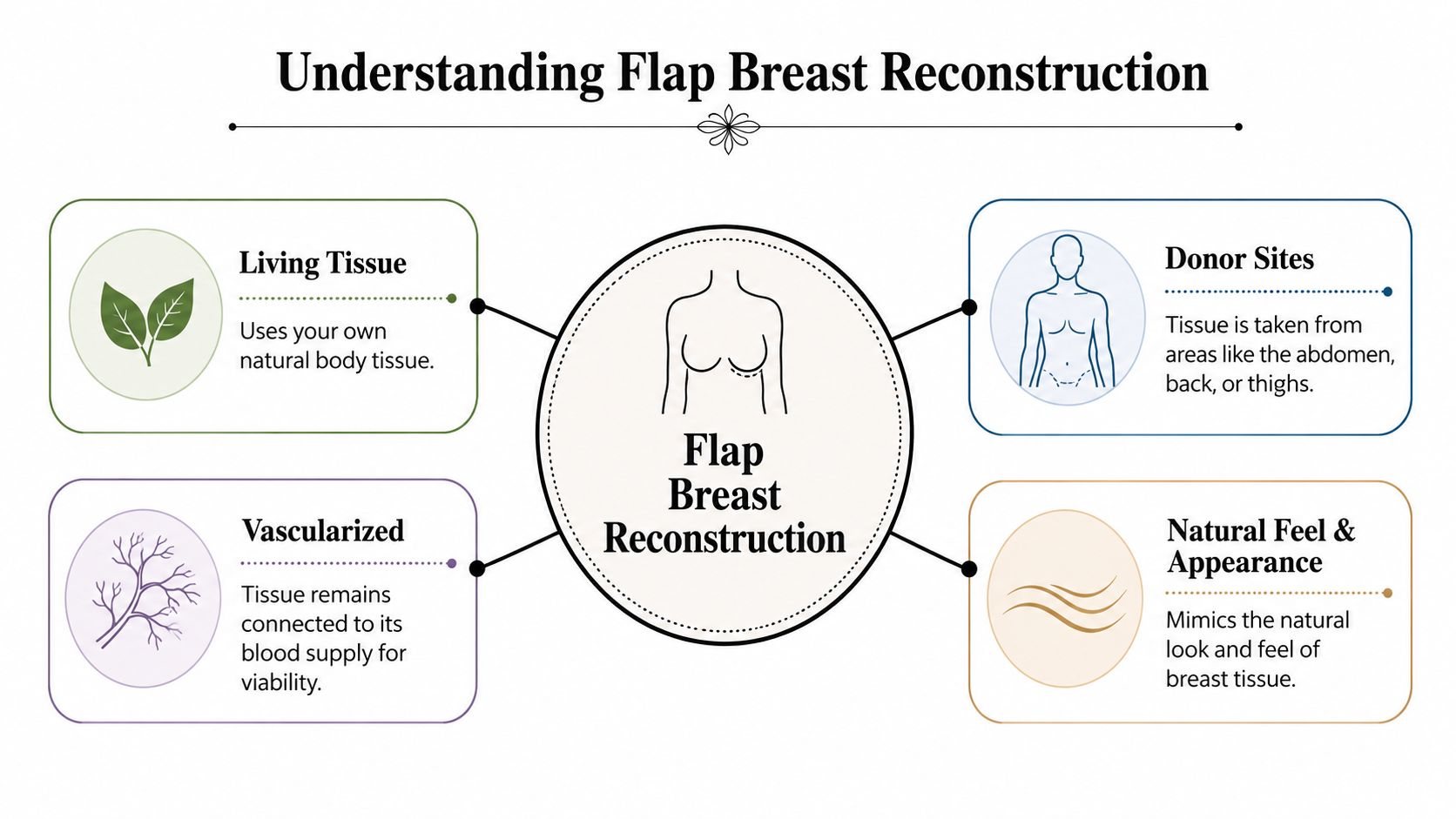
Understanding Flap Breast Reconstruction
Flap breast reconstruction is also called autologous reconstruction, which means the surgeon uses your own tissue rather than a manufactured implant. The tissue usually includes skin and fat, along with the blood vessels that keep that tissue alive. It may come from the abdomen, thigh, back, or another donor site depending on your body and surgical history.
A useful way to think about it is as a living puzzle piece. The surgeon takes tissue from one area where your body has extra soft tissue, then shapes that tissue into a new breast mound. In many flap operations, microsurgery is used to reconnect tiny blood vessels in the chest so the transferred tissue continues to live in its new location.
Why using living tissue changes the experience
An implant is a device. A flap is your own tissue. That difference shapes many of the long-term conversations patients have with surgeons.
Because the reconstructed breast is made from your own tissue, many patients are drawn to the possibility of a result that feels warmer, softer, and more integrated with the body. It is still surgery, and it still has scars and tradeoffs, but it is not the same as placing a prosthetic device under the skin.
There's also an important historical point here. Flap reconstruction is not an outdated option that survived only in a few specialty centers. In U.S. practice data, total breast reconstruction procedures rose from 137,808 in 2020 to 151,641 in 2022, and a market-share analysis found that plastic surgeons performed 95.8% of free flap reconstructions, with no clinically significant trend loss for free flap reconstruction over the prior two decades, as reported in U.S. reconstructive breast procedure statistics and free flap market-share analysis.
What often confuses patients
Many people hear “flap” and think it always means muscle is moved. That isn't always true. Some flap procedures spare muscle and mainly transfer skin and fat. Others may involve more donor-site impact. That's one reason flap reconstruction isn't one operation. It's a family of operations.
Another point of confusion is timing. A flap can sometimes be done at the time of mastectomy, and in other cases it's done later. The timing depends on cancer treatment, radiation plans, healing needs, and surgeon judgment.
Practical rule: Don't ask only, “What flap do I qualify for?” Ask, “Why does this flap match my goals better than the alternatives?”
That question usually leads to a much more useful consultation.
Exploring the Major Types of Flap Procedures
The easiest way to understand flap options is by donor site. Where the tissue comes from affects scar placement, donor-site recovery, tissue volume, and how much muscle function might be affected.
Abdominal flaps
For many patients, the abdomen is the first area discussed because it can provide a generous amount of soft tissue.
The DIEP flap is one of the most important advances in autologous reconstruction. It transfers abdominal skin and fat while preserving the rectus abdominis muscle and fascia. That muscle-sparing approach is associated with less postoperative pain, less abdominal wall weakness, and a lower hernia risk than older TRAM-based reconstruction, as described in this review of DIEP flap reconstruction and muscle preservation.
The TRAM flap also uses abdominal tissue, but the classic tradeoff is greater impact on the abdominal wall because it involves a muscle-bearing flap. In plain terms, it may be a good option in some circumstances, but many patients and surgeons prefer muscle-sparing approaches when feasible.
Thigh-based flaps
Not every patient is a good abdominal-flap candidate. Some are slender. Some have had prior abdominal surgery. Some want to avoid an abdominal donor-site scar.
That's where thigh-based options enter the conversation.
The PAP flap uses tissue from the upper posterior or inner thigh region. It has become an important alternative for patients who don't have enough abdominal tissue or can't safely use the abdomen. The TUG or gracilis-based family of flaps also draws from the thigh, though the exact donor-site and muscle involvement differ.
For smaller-breasted patients, or for those who prioritize preserving the abdomen for personal or medical reasons, these alternatives can be very meaningful. The key is that they aren't “second-best” by definition. They're different tools for different bodies.
Other flap approaches
The latissimus-based flap from the back may be considered in some situations. In selected smaller defects, surgeons may also use local or regional tissue rearrangement instead of a full free flap. That matters because more surgery isn't always better surgery. For certain defects, a more limited flap can be the smarter fit.
Here's a simple comparison to organize the options.
| Flap Type | Donor Site | Muscle Impact | Key Consideration |
|---|---|---|---|
| DIEP | Abdomen | Preserves rectus muscle | Good option when abdominal tissue is available and muscle-sparing is a priority |
| TRAM | Abdomen | Greater abdominal wall impact | Older approach that may still be used in selected cases |
| PAP | Thigh | Preserves muscle | Useful when the abdomen isn't a viable donor site |
| TUG or gracilis variant | Thigh | Involves gracilis-related donor-site considerations | May suit selected smaller-volume reconstructions |
| Latissimus-based flap | Back | Uses back tissue with donor-site tradeoffs | Can help in specific reconstructive scenarios |
A practical way to compare them during a consultation is to ask these three questions:
- Where will the scar be? A scar hidden in a lower abdominal crease feels different from one along the thigh or back.
- What function could be affected? Muscle-sparing procedures matter because donor-site strength and comfort matter.
- How much tissue is available? The donor site needs to provide enough soft tissue for the breast size and shape you want.
Patients often come in expecting a menu with one “best” answer. Flap reconstruction usually works differently. It's more like tailoring. The surgeon matches the operation to your anatomy and your priorities.
Are You a Candidate for Flap Reconstruction
Candidacy is rarely a simple yes or no. It's a balance of anatomy, medical history, cancer treatment, and what matters most to you.
The consultation checklist surgeons actually think through
Flap reconstruction is a long, technically demanding microsurgical operation, so patient selection matters. Prior radiation, body habitus, smoking history, and overall health directly influence flap choice and complication risk, according to this discussion of patient selection in DIEP flap reconstruction.
That may sound intimidating, but it should feel clarifying. Your team isn't trying to exclude you. They're trying to match you to the safest and most durable option.
A consultation often centers on questions like these:
- Overall health: Can your body safely handle a long operation and recovery?
- Smoking history: Smoking affects blood flow, and flap surgery depends on healthy blood vessels.
- Body habitus: Do you have enough tissue in the abdomen, thigh, or another donor site for your goals?
- Prior surgeries: Old scars, especially on the abdomen, may change which blood vessels are usable.
- Cancer treatment plan: Will radiation be part of treatment, or has it already been given?
Why radiation changes the discussion
Radiation can make tissues tighter, less elastic, and more difficult to reconstruct. That doesn't mean reconstruction is off the table. In some situations, it shifts the advantage toward bringing in healthy, well-vascularized tissue from another part of the body.
That's one reason flap reconstruction is often discussed seriously in patients with irradiated tissues. Healthy transferred tissue can sometimes provide a more durable contour and better tissue quality in that setting.
If you're sorting through cancer treatment details while also trying to understand surgery, reading about invasive breast cancer can help put the reconstruction decision into the larger treatment picture.
Prior surgery or radiation doesn't automatically make you a poor candidate. Often, it simply means your surgeon has to think more creatively.
Questions worth bringing to your visit
Rather than asking only, “Am I a candidate?” try asking:
- Which donor sites are realistic for my body?
- How does my radiation history affect your recommendation?
- If my first-choice flap isn't ideal, what is your next choice and why?
- What tradeoff matters most in my case, breast shape, donor-site recovery, or complication risk?
Those questions usually lead to more honest and useful answers than a simple thumbs-up or thumbs-down.
The Surgical Journey and Recovery Path
Recovery becomes easier to manage when you know what the milestones usually feel like. Flap surgery is a major operation, and it involves healing in two places: the chest and the donor site.
A visual overview helps many families keep the sequence straight.
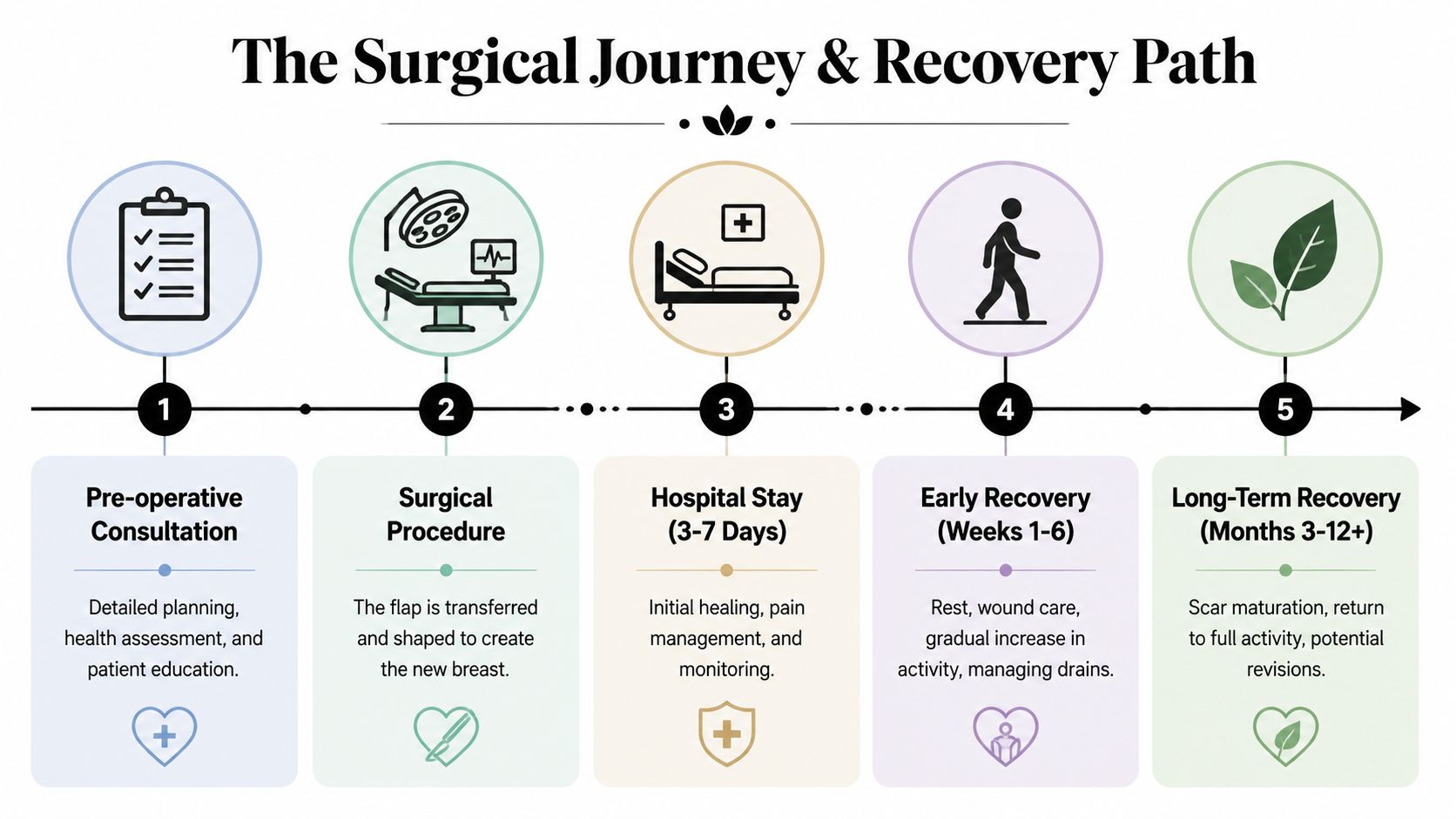
The first hospital days
Right after surgery, your team watches the flap closely. The reason is simple. A newly transferred flap depends on a healthy blood supply, so nurses and surgeons monitor color, warmth, and circulation carefully.
Most patients remember the first day as a blur of rest, vital signs, and getting comfortable enough to shift position. Then comes the first walk. It's often short, slow, and more important than it looks. Walking helps the lungs, circulation, and overall recovery.
You'll also be learning practical skills:
- Drain care: Surgical drains are common after mastectomy and reconstruction.
- Protective movement: You'll be shown how to stand, sit, and get in and out of bed with less strain.
- Pain control: The goal is manageable pain, not pretending you feel nothing.
If you're anxious about that part, this guide on drains after mastectomy can make the early recovery period feel less mysterious.
The first weeks at home
Home recovery usually feels less dramatic than people fear, but more tiring than they expect. You're healing from a long operation. Even simple tasks can take more effort for a while.
Many patients do best when they think in phases rather than deadlines.
- Early phase: Rest, short walks, nutrition, hydration, incision care.
- Middle phase: More upright movement, more independence, less drain-related hassle.
- Later phase: Gradual return to normal routines as swelling settles and strength returns.
For some patients, the abdomen won't be the right donor site at all. In that setting, thigh-based flaps such as the PAP flap are increasingly used because they preserve muscle, have low donor-site morbidity, and are especially useful when abdominal tissue is limited or prior abdominal surgery changes candidacy, as noted in this review of PAP flap use when the abdomen isn't viable.
Here's a patient education video that may help you picture the process more clearly.
What patients often ask about healing
“Will I feel normal right away?” Usually, no. But most people improve in layers rather than all at once.
The final shape also doesn't appear on day one. Swelling settles. Scars soften. Small refinements may happen later. Recovery asks for patience, but most patients feel better once they understand that healing is a process, not a single finish line.
Outcomes That Matter Patient Satisfaction and Aesthetics
The technical details matter, but they aren't why most patients choose flap reconstruction. They choose it because they're hoping for a result that feels more like part of their body and less like something added to it.
That hope is not just emotional. It lines up with patient-reported outcomes. In a nationwide cohort of more than 2,000 women, flap reconstruction was associated with greater satisfaction with the breasts and better psychosocial and sexual well-being at two years compared with implant reconstruction. Earlier comparison data also found 78.7% satisfaction among flap patients versus 31.6% in the implant group, with higher satisfaction scores for DIEAP flaps and an odds ratio of 8.438 for nipple-areola complex projection satisfaction after correction, as summarized in this report on higher satisfaction and quality-of-life outcomes after flap reconstruction.

Why satisfaction can be higher
A flap reconstruction is made of living tissue. That changes how many patients describe the result over time. They often focus less on the word “reconstructed” and more on the fact that the breast feels soft, warm, and physically part of them.
For some, the deciding factor is movement and aging. Your own tissue tends to change with your body. If your weight shifts, the breast may change with you in a more natural way than an implant does.
The deeper reason this choice matters
Breast reconstruction isn't only a visual decision. It can affect body image, intimacy, clothing confidence, and how at ease you feel moving through ordinary life. For some patients, part of recovery includes consciously finding emotional balance while their body and identity are both adjusting after treatment.
A few long-term benefits patients commonly value include:
- Natural softness: Your own tissue usually feels different from a device-based reconstruction.
- Durability: There's no implant to rupture or deflate.
- Body connection: Many patients say the result feels more integrated into their sense of self.
A good reconstruction doesn't erase what you've been through. It can help your body feel less divided by it.
That's often the strongest “why” behind flap breast reconstruction. Patients aren't choosing complexity for its own sake. They're choosing the possibility of a result that supports quality of life long after active treatment ends.
Finding Your Path with Hirschfeld Oncology
A family often reaches this point with a notebook full of questions and no single answer that fits neatly on the page. One person wants the softest, most natural feel possible. Another is worried about healing time, prior surgeries, or whether radiation has changed the options. Both concerns are reasonable.
By this stage, the choice usually stops being about procedure names and starts being about daily life after treatment. What will feel most like your body. What can work safely with your cancer care. What gives you the best chance of feeling comfortable, dressed, active, and at ease with the result over time.
Some patients do well with tissue from the abdomen. Others need a thigh-based flap because of body shape, prior surgery, or blood supply. Some are better served by waiting until treatment is further along. Patients who have been told they are "not the usual candidate" often still have options. The question is not whether they fit a standard template. The question is which plan best matches their anatomy, medical history, and goals.
At Hirschfeld Oncology, that discussion begins with the full picture. Cancer treatment timing, pathology, radiation plans, healing concerns, and reconstruction goals all matter together. Reconstruction is not a separate cosmetic decision floating outside the rest of your care. It works more like part of the same map, and the route needs to make sense as a whole.
If you are in Brooklyn, Williamsburg, Bushwick, or elsewhere in New York City, come with the questions you have now, not the questions you think you are supposed to have. Ask which option fits your body. Ask how treatment could affect timing. Ask what tradeoffs matter most if your priority is long-term softness, durability, symmetry, or a shorter recovery.
The strongest plan usually starts with a careful conversation, clear expectations, and a surgeon who is willing to explain the why behind each recommendation.
.png)
.png)




