




.png)


A lot of people first hear the word immunotherapy in a blur.
One day you're talking about biopsy results, scans, and whether you can still eat comfortably. The next day, someone says there may be a treatment that helps your own immune system recognize the cancer. For many patients and families, that sounds both promising and confusing. Is it chemotherapy? Is it gentler? Does it work for everyone? Does it replace surgery, or happen alongside it?
Those are the right questions.
Gastric cancer immunotherapy has changed the treatment options, but it hasn't turned stomach cancer into a simple disease. What it has done is give doctors a more precise way to match treatment to the biology of a tumor. That matters, because the key point isn't just that immunotherapy exists. It's that some patients are far more likely to benefit than others, and the difference often comes down to biomarker testing, treatment timing, and careful follow-up.
This guide is meant to make that path clearer. I'll walk through what immunotherapy does, why biomarker results matter so much, what approved options patients may hear about in clinic, and what practical questions to ask before the first infusion.
A New Chapter in Gastric Cancer Treatment
When a patient sits across from me after a new diagnosis, the conversation usually starts in the same place. They want to know what happens next, how serious this is, and whether treatment can still make a meaningful difference.
If immunotherapy comes up, families often react in one of two ways. Some assume it's a breakthrough that works for nearly everyone. Others think it sounds experimental and distant, like something available only at major research hospitals. The truth sits in the middle. It isn't a miracle fix, and it isn't science fiction either. It's now part of real treatment planning for some people with gastric cancer.
What makes this moment different from the past is that doctors can now use tumor biology to guide decisions more directly. Instead of treating every advanced stomach cancer as though it behaves the same way, we now look for signals that help predict who may benefit from immune checkpoint drugs.
Why this feels different
Traditional chemotherapy attacks fast-growing cells. Immunotherapy works differently. It tries to help the body's immune system identify and attack cancer cells that have learned how to hide.
That shift has changed the conversation in clinic. Patients are no longer just asking, "What drug can shrink this?" They're also asking, "What does my tumor testing show?" and "Am I the kind of patient this treatment is meant for?"
Gastric cancer care has become more personalized. That can feel overwhelming at first, but it also gives you more specific questions to ask and more ways to make an informed decision.
What families usually need most
In the first few visits, patients don't need more jargon. They need a way to organize the flood of information.
A useful starting framework is this:
- What is the goal of treatment: Is the plan aimed at controlling metastatic disease, preparing for surgery, or reducing the risk of recurrence?
- What does my biomarker testing show: This often shapes whether immunotherapy is likely to help.
- Will immunotherapy be used alone or with chemotherapy: In gastric cancer, combination treatment is often part of the discussion.
- What should I expect day to day: Many fears ease once patients understand the schedule, monitoring, and side effects.
That kind of clarity doesn't remove the stress. But it does give you back a sense of footing.
How Immunotherapy Fights Gastric Cancer
The easiest way to understand immunotherapy is to think of your immune system as a security team.
Its job is to patrol the body, recognize what doesn't belong, and remove threats. Cancer becomes dangerous partly because it learns how to avoid that security team. It can look less suspicious than it should. In some cases, it also sends signals that tell immune cells to stand down.
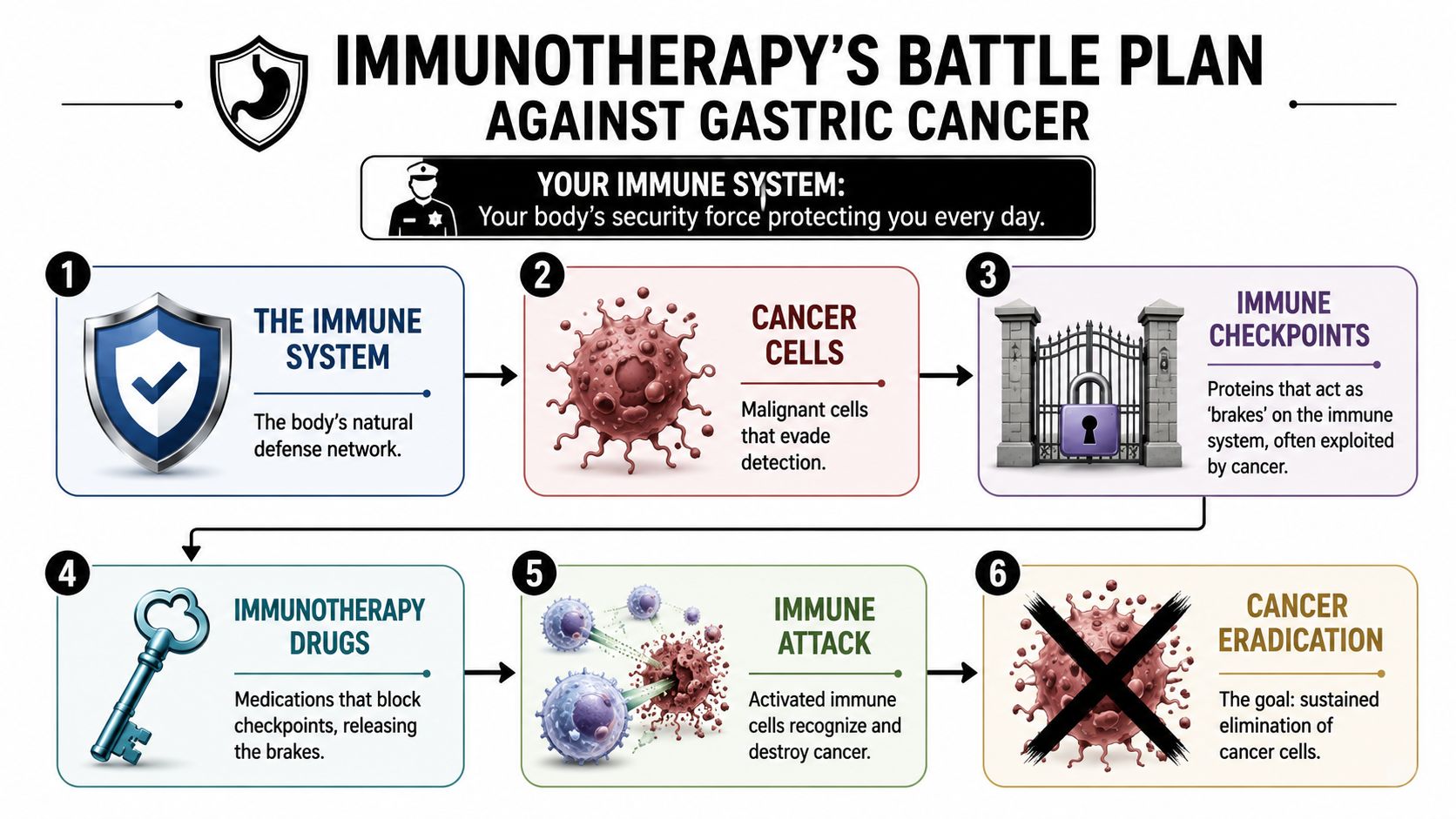
Releasing the brakes
One of the most important pathways in gastric cancer immunotherapy involves PD-1 and PD-L1.
You don't need to memorize those names. What matters is the idea. PD-1 is like a brake pedal on certain immune cells, especially T-cells. PD-L1 is one of the matching signals that can press that brake. When the two connect, the immune cell gets a message that says, in effect, "don't attack."
Some gastric cancers use that system to protect themselves.
Drugs such as pembrolizumab and nivolumab block that interaction. They interrupt the "stand down" signal, which can help T-cells recognize the cancer again. If you'd like a broader primer on the basics, this overview of how immunotherapy works in cancer care gives a helpful foundation.
What that means in plain language
Immunotherapy doesn't directly burn through cancer the way many people imagine chemotherapy does. It changes the conversation between the tumor and the immune system.
A simple way to picture it:
- The tumor hides by using immune checkpoints.
- The immune system hesitates because it receives a stop signal.
- The checkpoint inhibitor blocks that signal.
- The immune system has a better chance to respond.
That doesn't guarantee a response. Some tumors still resist treatment, and some patients benefit much more than others. But this is the core reason immunotherapy can work at all.
Why doctors often combine it with chemotherapy
Patients often ask, "If immunotherapy helps my immune system, why do I still need chemo?"
That's a fair question. In gastric cancer, doctors often use them together because they attack the disease in different ways. Chemotherapy can reduce tumor burden more directly, while immunotherapy may help the immune system sustain pressure on the cancer.
Practical rule: When your oncologist recommends immunotherapy plus chemotherapy, it usually means they're trying to use two different treatment strengths at the same time, not that one treatment failed.
That combination approach is one reason biomarker testing matters so much. It helps estimate whether adding immunotherapy is likely to be worthwhile.
Who Is a Candidate for Immunotherapy
The most important truth about gastric cancer immunotherapy is that it is not one-size-fits-all.
Two patients can have tumors in the same organ, similar scans, and similar symptoms, yet have very different odds of benefiting from the same immune checkpoint drug. The reason often lies in biomarkers, which are test results that tell us something about how the tumor behaves.
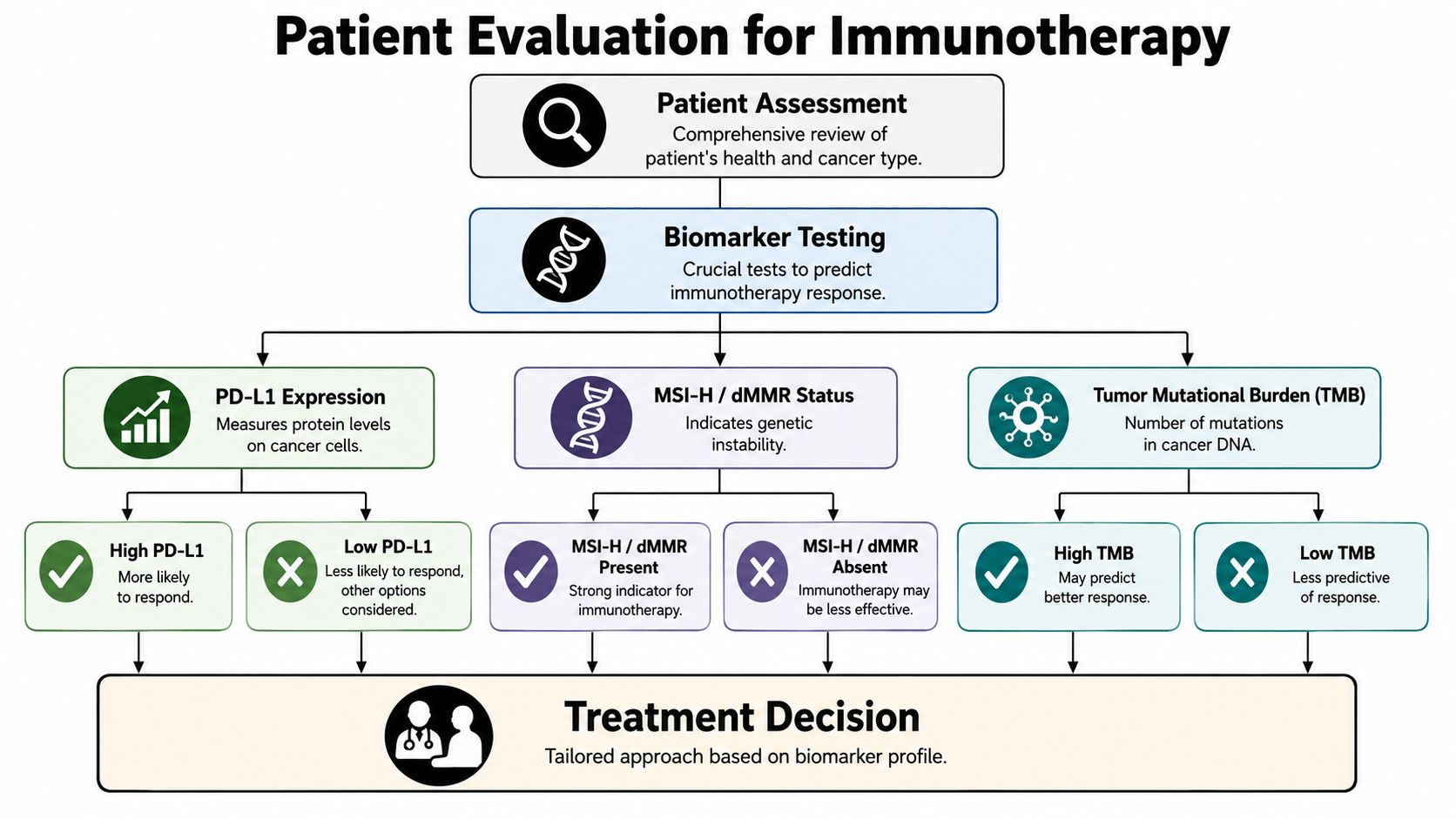
PD-L1 and the CPS score
One biomarker you may hear about early is PD-L1. In gastric cancer, doctors often discuss it using something called the Combined Positive Score, or CPS.
CPS measures PD-L1 staining cells, including tumor cells, lymphocytes, and macrophages, divided by the total number of tumor cells, multiplied by 100. Clinical evidence shows that immune checkpoint inhibitors are strongly stratified by CPS. Patients with CPS ≥1 can see overall survival benefit, and the benefit is more marked in the CPS ≥10 subgroup, while patients with CPS <1 show negligible survival advantage, according to this review of PD-L1 CPS and checkpoint inhibitor outcomes in gastric cancer.
In plain language, a higher CPS doesn't promise success. But it does make immunotherapy a more biologically sensible option.
MSI and mismatch repair
Another major biomarker is MSI-H, short for microsatellite instability-high, or dMMR, which refers to mismatch repair deficiency.
These tumors tend to stand out to the immune system more clearly, which is one reason they often respond better to immunotherapy. In practice, many oncologists consider MSI or mismatch repair status one of the most important predictive markers when deciding whether immune checkpoint treatment belongs in the plan.
If you're new to this language, this guide to cancer biomarkers and what they mean for treatment decisions can help decode the terms before your next appointment.
The tests patients should ask about
Biomarker testing isn't a side issue. It's central to treatment planning.
Here are the questions I want patients to feel comfortable asking:
- Was my tumor tested for PD-L1: If yes, ask for the actual CPS result, not just whether it was "positive."
- Was my tumor tested for MSI or mismatch repair deficiency: This can strongly influence the role of immunotherapy.
- Do HER2 results affect this decision: HER2 status can shape which combination strategies are considered.
- Was enough tissue available: Sometimes testing is delayed because the original biopsy sample was limited.
Bring a notebook or ask for printouts. Many treatment decisions make more sense once you can see the actual pathology and biomarker language in front of you.
A simple way to think about biomarkers
Patients sometimes hear "marker" and imagine a tiny lab detail that may or may not matter. In reality, biomarkers are more like road signs. They don't tell you exactly what the trip will feel like, but they do help point your oncologist toward the right lane and away from treatments less likely to help.
Approved Immunotherapy Options for Gastric Cancer
Once biomarker testing is underway, the next question is practical. Which immunotherapy treatments are used in gastric cancer today?
For many patients with advanced or metastatic HER2-negative gastric or gastroesophageal junction adenocarcinoma, the main conversation involves checkpoint inhibitors used with chemotherapy in the first-line setting. "First-line" means the first major treatment used for that stage of disease.
Pembrolizumab plus chemotherapy
A major milestone came on November 16, 2023, when the FDA approved pembrolizumab plus fluoropyrimidine- and platinum-based chemotherapy as a first-line option for locally advanced unresectable or metastatic HER2-negative gastric or gastroesophageal junction adenocarcinoma. In the phase III KEYNOTE-859 trial, median overall survival was 12.9 months with pembrolizumab versus 11.5 months with placebo, median progression-free survival was 6.9 months versus 5.6 months, and overall response rate improved from 42% to 51%, as summarized by the AACR overview of the FDA approval and KEYNOTE-859 results.
Those numbers may seem modest when read on a page. But in gastric cancer, they represent a real shift. They show that adding an immune checkpoint inhibitor can produce measurable benefit in a disease where durable systemic options have long been limited.
Nivolumab plus chemotherapy
Another first-line option in HER2-negative advanced gastric cancer is nivolumab combined with fluoropyrimidine and oxaliplatin chemotherapy. Reported trial data show a statistically significant median overall survival improvement, with a hazard ratio of 0.74 and median overall survival of approximately 14.4 months versus 11.1 months for chemotherapy alone.
For patients, the practical point is this: if your oncologist talks about nivolumab or pembrolizumab with chemotherapy, that isn't an unusual or fringe recommendation. It's part of modern treatment planning for selected patients.
What HER2-negative means in this context
Patients often think a "negative" test result sounds bad. Here it describes a tumor subtype.
HER2-negative means the cancer does not overexpress the HER2 protein in the way HER2-positive tumors do. That matters because HER2 status helps determine which drug combinations make sense. It doesn't tell the whole story on its own. It just helps your team sort through the right treatment categories.
A quick summary can make the information easier to scan:
| Treatment context | What patients often hear in clinic | Why it matters |
|---|---|---|
| First-line | "This is the initial treatment plan for advanced disease" | It sets the backbone of care |
| HER2-negative | "This tumor doesn't fit the HER2-positive pathway" | It affects which combinations are considered |
| Immunotherapy plus chemo | "We're pairing checkpoint blockade with standard drugs" | It uses two treatment mechanisms together |
If you're handed a long treatment name, ask your oncologist to translate it into three plain questions: What is the goal, why this combination, and how will we know if it's helping?
Balancing Hope with Realistic Expectations
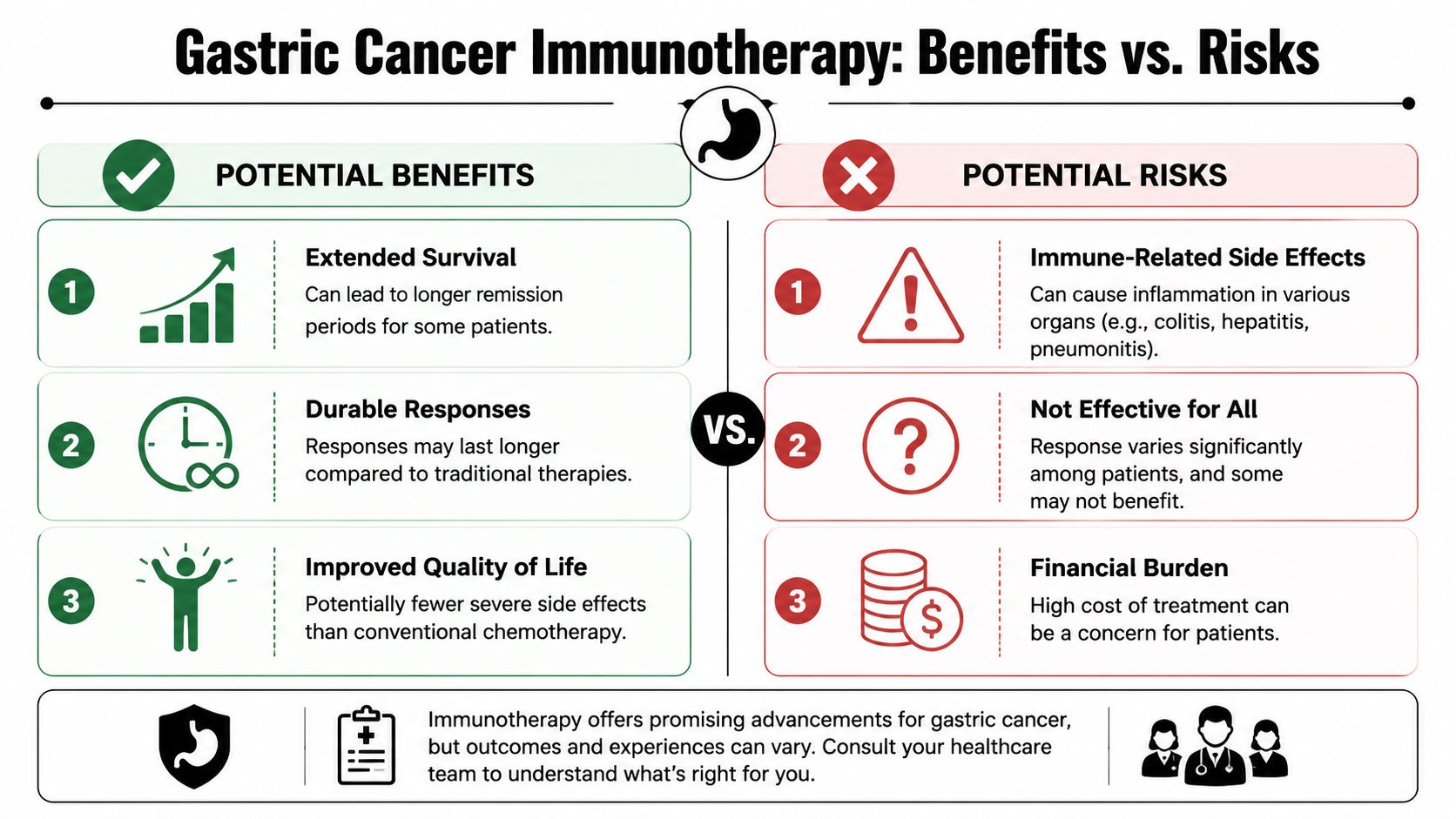
One of the hardest jobs in oncology is telling the truth without taking away hope.
With gastric cancer immunotherapy, both matter. There is real reason for optimism. Some patients do have meaningful responses, and some responses last longer than we used to expect from systemic treatment alone. At the same time, not every patient benefits, and the side effects are different from standard chemotherapy.
What hope should be based on
The strongest hope is informed hope.
A critical question is who benefits from immunotherapy. Overall benefit is concentrated in biomarker-defined subgroups, and broad messaging can obscure that MSI-H and other responsive groups are a minority of gastroesophageal adenocarcinomas. Experts also note that even in responsive tumors, many still favor combining immunotherapy with chemotherapy rather than relying on immunotherapy alone, as discussed in this expert conversation about who benefits from gastric cancer immunotherapy.
That doesn't make immunotherapy less important. It makes patient selection more important.
The side effects are different, not absent
Many people hear "immunotherapy" and assume it must be easier than chemotherapy. Sometimes it is. But "different" is a better word than "easy."
Because these drugs activate the immune system, side effects can come from inflammation in healthy tissues. You may hear your care team call these immune-related adverse events.
Common issues patients report include:
- Fatigue: This can build gradually and sometimes feels different from ordinary tiredness.
- Skin changes: Rash or itching may show up early and should be reported, even if it seems minor.
- Diarrhea: This can signal bowel inflammation, not just a routine stomach upset.
- Breathing symptoms: New cough or shortness of breath always deserves prompt attention.
- Hormone-related changes: Some patients develop thyroid or other endocrine problems that show up as weakness, mood changes, or unusual temperature sensitivity.
Call your oncology team early if something changes. With immunotherapy, small symptoms can matter more than patients expect.
A balanced way to think about treatment
I often tell families to hold two ideas at once.
First, this treatment can be meaningful and, for the right patient, worth pursuing. Second, it requires close observation, honest conversations, and a willingness to adjust the plan if the biology or side effects point in a different direction.
That balance is not pessimism. It's how good cancer care works.
Navigating Your Immunotherapy Journey
The day treatment starts, many patients stop worrying about abstract science and start worrying about practical things. How long will I be there? Can I eat first? What if I feel fine one day and strange the next?
Those questions deserve direct answers.

Questions to bring to your next visit
A short written list can completely change the quality of an appointment. Consider asking:
- What is my exact treatment goal: Control of metastatic disease, preparation for surgery, or lowering recurrence risk?
- Which biomarker results are driving this plan: Ask for PD-L1, MSI or dMMR, and HER2 results in plain language.
- Why are you recommending immunotherapy with chemotherapy, rather than one or the other alone: This helps you understand the logic of the backbone.
- How often will I get treatment and scans: A calendar reduces anxiety.
- Which symptoms should trigger a same-day phone call: Don't rely on guesswork.
- Should I ask about a clinical trial: In some settings, especially around surgery, this can matter.
What an infusion day often looks like
Every center runs a little differently, but the rhythm is usually familiar. You check in, have vital signs taken, review symptoms, and often get lab work. A nurse confirms the treatment plan, and the infusion itself is given through an IV or port.
Most of the time, the experience is quieter than people expect. Patients read, nap, listen to music, or sit with a family member. At practices such as Hirschfeld Oncology, outpatient infusion care may also include close symptom monitoring and individualized treatment planning, which is especially important when patients are trying to balance treatment intensity with quality of life.
Where clinical trials fit
Patients often hear exciting headlines and assume those therapies are standard everywhere. That's not always the case.
Recent progress in stomach cancer is often defined by perioperative trial results. Mayo Clinic has described the current standard for locally advanced stomach cancer as including neoadjuvant chemo-immunotherapy followed by surgery and adjuvant therapy, with published studies reporting complete response rates up to 20%, while also noting that patients still need help understanding whether these options are standard care or mainly available in trials, as outlined in this review of recent innovations in stomach cancer care from Mayo Clinic.
That means a good question is not just "Is there a new treatment?" It's "Is this standard for my situation, or is it something I could access through a trial?"
Before deciding, some patients find it helpful to hear a specialist discuss how these treatment choices are framed in practice.
What helps at home
The best home strategy is simple and consistent.
- Track symptoms daily: Write down bowel changes, appetite, energy, cough, fever, rash, or pain.
- Report early: Don't wait to see if a possible immune side effect "passes."
- Keep medications organized: Include over-the-counter drugs and supplements in your list.
- Bring support to visits: A second set of ears helps when decisions feel complicated.
The patient who does best is not always the one who feels the strongest. It's often the one who reports changes quickly and stays closely connected to the care team.
Find Your Path with Personalized Cancer Care
The central message in gastric cancer immunotherapy is both hopeful and practical. Treatment has improved, but the improvement depends on matching the right therapy to the right tumor and the right patient.
Biomarkers such as PD-L1, HER2, and MSI status now sit near the center of decision-making. That shift matters because, before 2021, there had been no overall survival improvement in advanced disease until trials such as CheckMate 649 and KEYNOTE-859 established the value of a biomarker-selected approach, as discussed in this analysis of recent advances in gastric cancer care. If you'd like to better understand how these tumor-specific results guide treatment planning, this overview of molecular testing in cancer care is a useful next step.
For patients and families, that means the next best move is rarely guessing. It's getting your pathology, biomarker testing, treatment goals, and tolerability discussed in one clear conversation.
A careful oncology team can help translate complex science into concrete decisions. That includes deciding whether immunotherapy belongs in the plan, whether it should be paired with chemotherapy, how to monitor for immune-related side effects, and when a clinical trial may be worth discussing.
You don't need to understand everything at once. You do need a team that can explain your options plainly, answer your questions openly, and adjust the plan as your situation evolves.
If you're looking for Hirschfeld Oncology in the New York City area, a consultation can help turn a complicated diagnosis into a more specific plan. Dr. Azriel Hirschfeld and his team provide outpatient cancer care that includes immunotherapy, personalized treatment strategies, and close monitoring for patients with complex and advanced-stage diagnoses, including gastric cancer. A thoughtful visit can clarify your biomarker results, review standard and emerging options, and help you decide what path fits your goals and tolerability.
.png)
.png)




