




.png)


The call may have been short, but its weight can feel enormous. You were told you have hairy cell leukemia, and now your mind is racing ahead to the questions that matter most. How serious is this. What happens next. Am I going to be okay.
The first thing I'd want you to hear, if we were sitting together in clinic, is that this diagnosis usually does not behave like the fast-moving blood cancers many people fear when they hear the word leukemia. In modern practice, the outlook is often very favorable, and the hairy cell leukemia prognosis is best understood as a long journey that can be managed thoughtfully over time, not a single frightening number handed to you on day one.
That doesn't mean the diagnosis is minor. It means it is treatable, often very treatable, and your decisions, your follow-up, and your partnership with an experienced oncology team can meaningfully shape what comes next.
Receiving a Hairy Cell Leukemia Diagnosis
Many people arrive at this diagnosis after weeks or months of confusion. Maybe you felt more tired than usual. Maybe routine bloodwork came back abnormal. Maybe your doctor mentioned an enlarged spleen, or you ended up needing a biopsy and are now trying to decode unfamiliar words from a pathology report. If you're still preparing for or recovering from that test, this guide to the bone marrow biopsy procedure can help make the process less mysterious.
Hairy cell leukemia often creates a very specific emotional mix. Patients tell me they feel frightened because it's a leukemia, but also unsettled because they've never heard of it before. Rare cancers can do that. They leave you with too little context and too many unanswered questions.
Here is the reassuring part. The National Cancer Institute says hairy cell leukemia is “highly treatable but rarely cured,” and notes that many patients have prolonged survival. In the same source, Cancer Research UK reports that in England more than 90% of people survive at least 5 years after diagnosis, and one study found a median survival of 27 years, showing that many people live for decades after diagnosis (National Cancer Institute treatment summary).
You are not starting from a place of hopelessness. You are starting from a diagnosis that medicine has learned how to manage far better than many patients first assume.
That phrase, “rarely cured,” can sound discouraging at first. In practice, it usually means something more nuanced. Many people enter long remissions, return to normal routines, and need only periodic monitoring for years before any treatment question comes up again.
A good first goal isn't to know every answer immediately. It's to slow the noise, get clear on the facts of your own case, and ask: What type of hairy cell leukemia do I have, how is it affecting my blood counts and spleen, and when do we need treatment?
What Prognosis Means for Hairy Cell Leukemia
Prognosis is a forecast, not a verdict.
That distinction matters because people often hear a survival statistic and mistake it for a prediction about their own life. It isn't. A prognosis is more like a weather report. It uses what happened to many patients in the past to estimate what may happen for someone with similar features today. But just as weather changes with local conditions, your outlook depends on your own health, your disease pattern, and how well treatment works for you.

Terms that often confuse patients
A few words come up again and again in discussions about hairy cell leukemia prognosis.
| Term | What it means in plain language |
|---|---|
| Prognosis | The expected course of the disease, based on patterns seen in other patients and adjusted to your situation |
| Remission | The leukemia has become very quiet or hard to detect after treatment |
| Complete remission | Doctors can't find signs of active disease using the tests they are using at that time |
| Partial remission | The leukemia has clearly improved, but some evidence of disease remains |
| Relapse | The disease returns or becomes more noticeable again after a remission |
| Relapse-free survival | How long people stay in remission before the disease returns |
| Progression-free survival | How long people live without the disease worsening after a treatment |
Patients also ask about 5-year survival. This term causes a lot of unnecessary fear. It does not mean a person is expected to live only five years. Instead, it measures how many people are alive five years after diagnosis in a study group. For diseases like hairy cell leukemia, many patients live well beyond that point.
Why the same diagnosis can lead to different outlooks
Two people can both have hairy cell leukemia and still have very different experiences.
One person may be diagnosed after routine lab work, feel fairly well, and respond beautifully to first treatment. Another may arrive with lower blood counts, more symptoms, or a disease pattern that needs closer follow-up. Neither person has done anything wrong. Their disease biology and overall health are different.
Practical rule: When you hear a statistic, ask your doctor, “How much does this apply to me personally?”
That question moves the conversation from population averages to individual care. It's one of the most useful things a patient can say in the exam room.
A better way to think about prognosis
The most helpful frame is this: prognosis changes over time.
It changes when doctors learn more from your bone marrow biopsy, blood counts, and scans or exam findings. It changes after treatment, especially if you achieve a deep remission. It changes again if you stay well for years. In that sense, the hairy cell leukemia prognosis is not a fixed label. It's an evolving story shaped by observation, treatment response, and careful follow-up.
Key Factors That Shape Your Individual Prognosis
When oncologists talk about prognosis, we are really building a picture from several clues at once. We don't look at one lab value or one symptom in isolation. We look at the whole patient.
The patient matters, not just the disease
Age and general health shape how someone tolerates treatment and recovers afterward. This doesn't mean older patients can't do well. Many do. It means doctors tailor decisions around the body in front of them, including other medical conditions, current symptoms, infection risk, and how much reserve the bone marrow appears to have.
A simple example helps. If two patients have the same leukemia cells under the microscope, but one has strong blood counts and few symptoms while the other has more severe fatigue, infections, or bleeding concerns from low counts, their treatment urgency and recovery path may differ.
Disease burden changes the conversation
Doctors also assess how much the leukemia is affecting the body.
That often includes:
- Blood counts: Hairy cell leukemia commonly lowers normal blood cells. Those numbers help explain fatigue, infection risk, or bruising.
- Spleen involvement: An enlarged spleen can cause fullness, discomfort, or early satiety.
- Bone marrow involvement: The marrow is where blood cells are made, so heavier involvement can disrupt normal production.
This is why prognosis isn't just about the name of the disease. It's about how significantly the disease is interfering with day-to-day body function at the time you are assessed.
Treatment response is one of the strongest signals
How well the leukemia responds to the first treatment often tells us a lot.
Patients who enter a deep, durable remission after initial therapy often need fewer repeat treatments over time. That matters not only for disease control, but also because fewer treatment courses can mean less cumulative immune suppression and less disruption to normal life.
Some patients understandably focus only on the day treatment starts. I usually encourage them to think one step further ahead. The question isn't only “Can we treat this?” It's also “How completely can we quiet it down, and for how long?”
The depth of first remission often shapes the rhythm of the years that follow.
Genetics and disease subtype help personalize care
Hairy cell leukemia is not a one-size-fits-all diagnosis. Subtype and molecular testing can influence treatment choices, especially in relapsed disease. One important marker in classic hairy cell leukemia is the BRAF V600E mutation, which can open the door to targeted treatment strategies in the right setting. If you want a clearer picture of why this marker matters, this overview of the BRAF V600E mutation is a useful starting point.
For patients, the practical takeaway is simple. Ask your doctor not only what the diagnosis is, but also what features of your disease matter most. Good questions include:
- What subtype do I have
- How affected are my blood counts
- Is my spleen enlarged
- How much bone marrow involvement is there
- Were molecular markers tested
- What would count as a strong response in my case
Those questions turn a vague fear into a manageable plan.
How Modern Treatments Transformed the HCL Outlook
A diagnosis of hairy cell leukemia can make the future feel as if it has suddenly narrowed. Then treatment discussions begin, and many families are surprised by what they hear. In classic hairy cell leukemia, the outlook changed dramatically once doctors began using therapies that could produce deep remissions that often last for years.
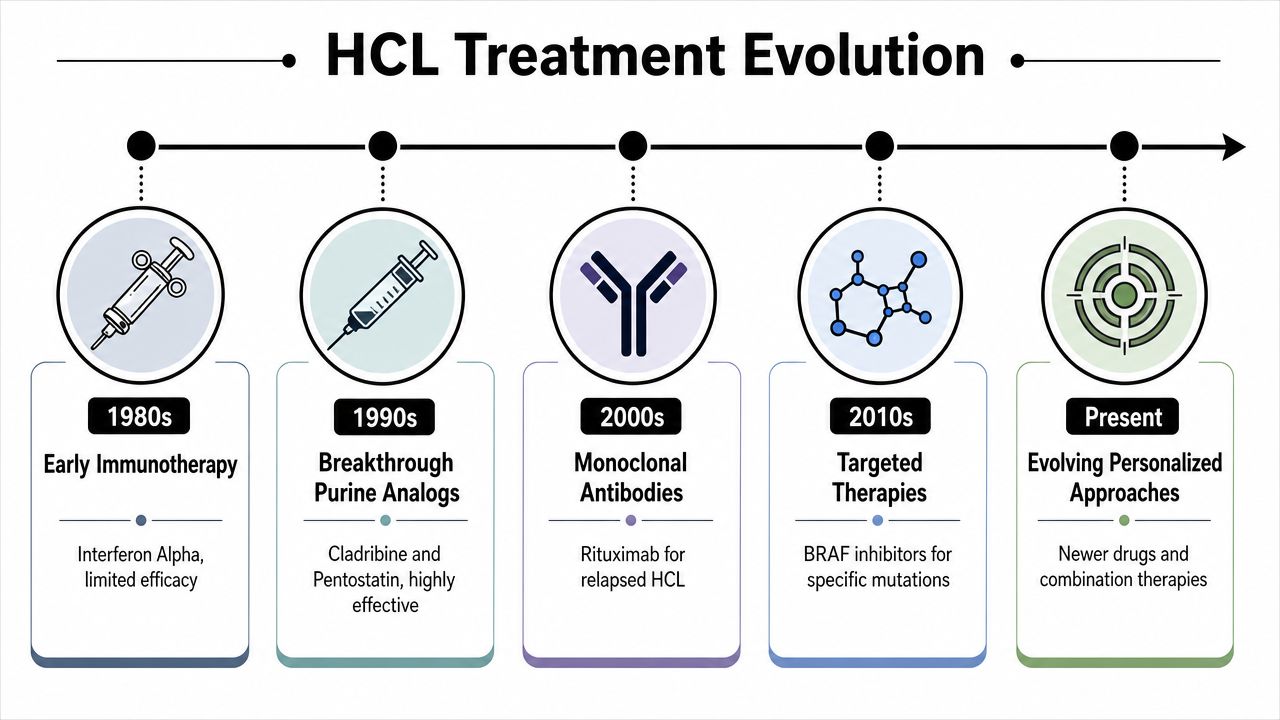
Why cladribine was such an important breakthrough
One of the biggest turning points in HCL care was the use of the purine analog cladribine. A single course of cladribine produces a complete response in about 90% of patients, and the median relapse-free survival is 11 years after first-line treatment. After a second-line treatment, the median relapse-free survival is about 7 years (NCBI Bookshelf overview of Hairy Cell Leukemia).
Those numbers matter, but their practical meaning is easier to grasp in everyday terms. For many patients, treatment is not an endless monthly cycle. It is often a strong first push that puts the disease into a long quiet period.
HCL often behaves less like a fire that needs constant spraying and more like a problem that can be brought under control, then watched carefully over time. That difference is a major reason prognosis discussions today are more hopeful and more individualized than they were in the past.
Relapse is part of the story, not the whole story
Relapse can happen. Saying that clearly helps patients prepare without assuming the worst.
If HCL returns, doctors still have options. Depending on the situation, treatment may include another purine analog, rituximab, or a targeted approach based on the biology of the leukemia. For readers who want a clearer sense of where antibody-based therapies fit into cancer treatment, this guide to what immunotherapy is for cancer offers helpful background.
The next step depends on details that are specific to you. Your oncologist will look at how long the first remission lasted, how your blood counts recovered, what side effects you had before, whether molecular testing shows a targetable mutation, and what matters most in your daily life. A younger patient trying to minimize time away from work may weigh options differently than an older patient focused on infection risk or other medical conditions.
Modern care changed prognosis from a number into a long-term plan
The biggest shift is not only better treatment. It is a better way of thinking about prognosis.
Years ago, prognosis was often discussed as if it were a fixed prediction. In HCL, it is more useful to see prognosis as a journey that can change with good decisions, good timing, and close follow-up. The goal is not only to treat the leukemia once. The goal is to build a plan that controls disease, protects quality of life, and preserves future options.
That takes partnership. Patients help this process when they report new fatigue, infections, bleeding, or abdominal fullness early, keep follow-up appointments, and ask direct questions about why one treatment is being chosen over another. Doctors help by explaining the tradeoffs clearly and adjusting the plan as the disease changes.
That kind of collaboration does more than improve communication. It often leads to better-timed treatment and a clearer path through remission, relapse if it occurs, and long-term survivorship.
Living Well After Diagnosis A Guide to Survivorship
After the first shock fades, many people ask a different question. Not “Will I survive this?” but “What will life look like after treatment?” That's the right question.
For many patients, survivorship after hairy cell leukemia becomes a long phase of monitoring, recovery, and rebuilding confidence in the body. A diagnosis can make people feel as if normal life has been put on hold forever. Often, it hasn't. It has changed, but it hasn't disappeared.
What long-term follow-up usually involves
Follow-up is how doctors watch for recovery, remission durability, and signs that the disease may be waking up again. Visits often focus on symptoms, physical exam findings, and blood tests. Some patients need more testing at specific times, especially if blood counts shift or symptoms return.
A survivorship mindset helps. Instead of thinking of follow-up as waiting for bad news, think of it as routine maintenance. You don't monitor because failure is expected. You monitor because early changes are easier to interpret and manage.
Here are practical pieces of survivorship care many patients find helpful:
- Keep a simple symptom log: Fatigue, infections, bleeding, abdominal fullness, or unusual changes are easier to discuss when written down.
- Track your blood count trends: You don't need to interpret every result alone, but it helps to know your own baseline.
- Ask about immune recovery: Some treatments can leave people more vulnerable to infection for a time.
- Build a follow-up calendar: Knowing when labs and visits are due reduces background anxiety.
What the long view can look like
The most encouraging part of survivorship in hairy cell leukemia is that long-term outcomes can be very strong. A 35-year follow-up study found that overall survival for patients with hairy cell leukemia was equivalent to the general population, with a standardized mortality ratio of 0.8, suggesting that long-term outlook can approach normal life expectancy (35-year follow-up study in PMC).
That doesn't mean every patient's path is identical. Some people need treatment again. Some have more complex courses. But this kind of long-term data gives patients permission to imagine a future that includes work, family plans, travel, exercise, and ordinary milestones.
A useful question for clinic visits: “What should I be doing between appointments to stay as healthy and prepared as possible?”
That question often leads to better conversations than “Am I cured?” because it focuses on the part of prognosis you can influence right now.
A good survivorship plan is practical
A strong plan usually includes who to call for new symptoms, when routine labs are due, what late effects to watch for, and how your oncology care fits with your primary care. It should also include the everyday pieces people sometimes overlook, such as vaccinations, infection precautions when relevant, and support for fatigue or emotional stress.
Patients do better when survivorship is active, not passive. You are not just “waiting to see what happens.” You are participating in the long-term stewardship of your health.
Navigating Your Cancer Care in New York City
Rare blood cancers raise a practical problem. Many excellent doctors may see only a small number of cases. That's one reason a second opinion can be useful, especially when the diagnosis is new, when test results feel unclear, or when the disease returns after remission.
In New York City, patients have access to academic centers, community oncologists, and specialty hematology practices. The goal isn't to collect opinions endlessly. It's to make sure the diagnosis is precise, the need for treatment is clear, and the treatment sequence makes sense for your situation.
When a second opinion makes the most sense
A second opinion is especially reasonable if:
- The diagnosis feels uncertain: Rare diseases sometimes need review of pathology and blood findings.
- Treatment is being recommended quickly: It's fair to ask whether treatment is needed now or whether observation is appropriate.
- You've relapsed: Later-line decisions can be more nuanced and may depend on prior response and molecular features.
- You want access to broader options: Some centers have more experience with uncommon disease patterns and targeted strategies.
What to look for in a treatment team
The best-fit team is usually one that explains things clearly, reviews pathology carefully, watches blood counts closely, and welcomes questions rather than rushing past them.
In a city as large as New York, convenience also matters. Treatment and follow-up are easier to sustain when the office location, infusion access, and communication style fit your real life. If you live in Brooklyn, Williamsburg, Bushwick, or nearby neighborhoods, it's reasonable to ask not only who has expertise, but who can also provide consistent outpatient follow-up without turning each visit into an ordeal.
You do not have to choose between medical sophistication and humane care. For a long-term illness, you need both.
Frequently Asked Questions About HCL Prognosis
Is hairy cell leukemia curable or chronic
The most honest answer is that it is usually treated as a chronic but highly manageable disease. Many people achieve long remissions after treatment and live full lives, but doctors remain careful because relapse can happen later. That's why follow-up matters even when you feel well.
Does a good prognosis mean I won't need treatment
Not necessarily. Some patients need treatment near diagnosis because their blood counts are low, their spleen is enlarged, or they have symptoms. Others may be monitored before treatment is started. A good prognosis means effective treatment options exist and long remission is often possible. It does not mean every patient can avoid therapy.
If I relapse, does that mean my outlook becomes poor
Not automatically. In hairy cell leukemia, relapse is often a management issue rather than a crisis in the way patients first imagine it. Doctors look at how long the first remission lasted, what treatment you had before, whether you tolerated it well, and what disease features are present now. Those details guide the next step.
Will I be on treatment forever
Usually not in the way people think of continuous cancer treatment. Many patients receive a course of therapy and then spend a long period in remission with monitoring rather than ongoing active treatment. If treatment is needed again later, the plan is reassessed based on the current situation.
What should I ask at my next appointment
Bring a short list. These questions often help:
- Do I need treatment now, or is watchful waiting appropriate
- What signs in my blood counts or symptoms are driving this decision
- What treatment are you recommending first, and why
- What would count as a complete response in my case
- How will we monitor me after treatment
- If the disease returns later, what options would likely come next
Should I worry about every abnormal blood test afterward
No. Trends matter more than one isolated value. Blood counts can fluctuate for many reasons. Your oncology team looks for patterns, not just single blips. If a result changes, ask what it means in context rather than assuming the worst.
How can family members actually help
Family support is most useful when it is practical. A relative or friend can attend visits, help track questions, organize lab reports, and notice symptom changes you may downplay. Emotional support matters too, but concrete help often lowers stress the most.
Where do hope and realism meet
They meet in the middle of good information.
Hope is not pretending the disease doesn't exist. Hope is understanding that this leukemia is often very responsive to treatment, that long remissions are common, and that your choices, your follow-up, and your partnership with experienced clinicians can influence the quality of the years ahead.
If you or a loved one is trying to make sense of a rare blood cancer diagnosis, Hirschfeld Oncology offers educational resources and information about patient-centered cancer care in Brooklyn and New York City. A thoughtful consultation can help clarify the diagnosis, review treatment options, and turn uncertainty into a practical plan.
.png)
.png)




