




.png)


Starting immunotherapy often feels like standing in two places at once. You're hopeful because this treatment can help your own immune system recognize cancer more effectively. You're also uneasy because the side effects don't behave like the side effects many families already know from chemotherapy.
A common question in clinic is simple and important: “If something changes, how do we know whether it's the treatment, the cancer, or just a bad week?” That's exactly where immune related adverse events enter the picture. These are side effects caused by an activated immune system. They can affect almost any organ, and they don't always show up on a predictable schedule.
The good news is that this is manageable when patients and clinics work as a team. The patients who do best are not the ones who stay silent and try to “push through.” They're the ones who report changes early, keep a running symptom log, and let the oncology team decide what needs attention now, what can be watched, and what needs urgent treatment.
Understanding Immunotherapy and Your Immune System
If you're receiving immunotherapy, your treatment is designed to help your immune system recognize and attack cancer cells more effectively. One practical overview of how these treatments are used is available through immunotherapy at Hirschfeld Oncology.
I often explain the immune system like a guard dog. A well-trained guard dog protects the house and reacts to intruders. Immunotherapy can make that guard dog more alert and more willing to act. That's the benefit.
The problem is that sometimes the dog also barks at the mail carrier. In medical terms, the immune system may begin attacking healthy tissue along with cancer. That inflammation is what causes immune related adverse events.
Immune related adverse events are not automatically a sign that treatment has failed. They mean the immune system has become active in a way that needs guidance.
That's why symptom reporting matters so much. A rash, cough, diarrhea, unusual fatigue, or new shortness of breath may seem unrelated at home. In clinic, those details can tell us which organ system may be inflamed and how quickly we need to respond.
What patients should remember
- Your body may signal trouble early: Small changes often matter more than dramatic ones.
- Timing can be unpredictable: Symptoms can appear during treatment, between cycles, or after treatment has been held.
- Early calls help: Most irAEs are easier to manage when we intervene before inflammation builds.
What Causes Immune Related Adverse Events
Checkpoint inhibitors work by releasing some of the immune system's normal restraints. In plain language, they take the brakes off T cells. That can be very effective against cancer, because T cells are some of the body's most powerful defenders.
But the same change can create misfires.
According to a review on T-cell mechanisms in irAEs, dysregulation of T cell subsets constitutes the primary immunopathological driver of immune-related adverse events, including activation of autoreactive T cells, imbalance in regulatory T cells, and persistence of tissue-resident memory T cells. The same review notes that affected tissues can functionally resemble classic autoimmune disease because immune tolerance has been lost, leading to organ-specific inflammation, as described in this ScienceDirect review on T-cell dysregulation in irAEs.
The brake system and the double hit
Under normal conditions, the immune system has built-in safeguards. Some cells activate inflammation. Other cells, including regulatory T cells, help prevent the immune system from attacking the body itself.
When checkpoint inhibitors block CTLA-4 or PD-1 pathways, they can shift that balance. Self-reactive T cells become more active. At the same time, the cells that usually calm things down may be less effective. That's why irAEs can look and behave like autoimmune conditions.
In some patients, especially those receiving combination checkpoint therapy, this becomes a “double hit.” More aggressive immune activation can produce stronger anti-cancer effects, but it can also raise the chance of clinically meaningful inflammation in healthy organs.
Why one person gets a rash and another gets thyroiditis
There isn't a single universal pattern. One patient may develop skin itching. Another may develop colitis, hepatitis, thyroid dysfunction, arthritis, or lung inflammation. The organ involved depends on where the immune system focuses its attack.
That uncertainty is frustrating, but it's also why careful monitoring works. We don't wait for one “classic” symptom. We listen for any new symptom that persists, worsens, or doesn't fit your usual pattern.
Clinical reality: The hardest irAEs to catch are not always the most dramatic. They're the symptoms patients explain away as stress, aging, reflux, allergies, or “just treatment fatigue.”
What does not work
A few habits repeatedly cause trouble:
- Waiting for the next appointment: A symptom that is mild on Monday may be serious by Thursday.
- Self-diagnosing from old side effects: Immunotherapy side effects don't follow the same rules as nausea after chemotherapy.
- Assuming normal vital signs mean everything is fine: Early inflammation can still be present even when someone looks stable.
Common Symptoms and Affected Body Systems
Patients rarely experience symptoms in neat textbook categories. A person may call about a cough and mention, almost as an aside, that they've also had loose stools and unusual fatigue. That combination matters. We sort symptoms by body system because it helps patients know what to watch and what to report.
A quick visual summary can help families keep the common patterns straight.
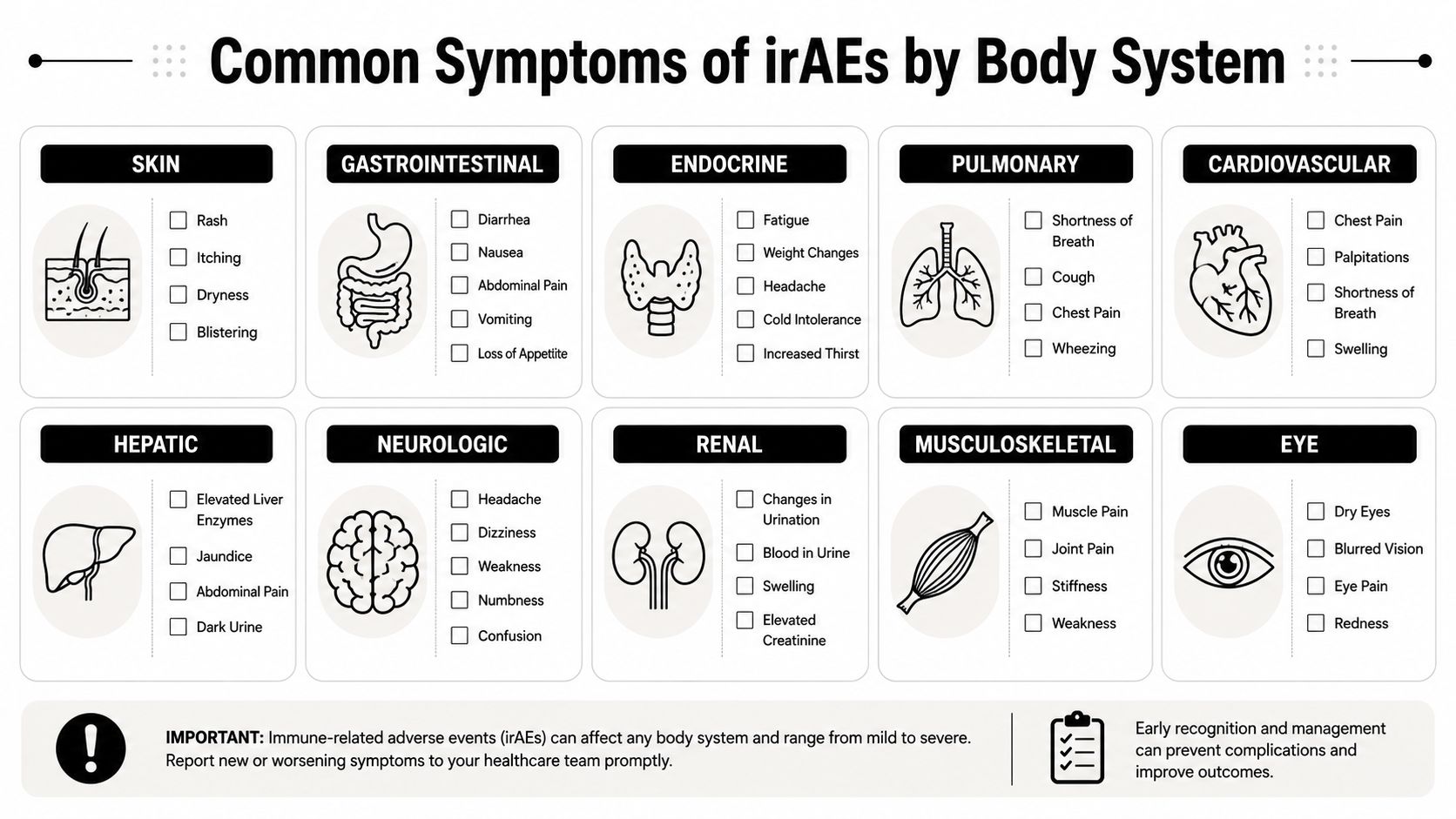
Skin and mouth
Skin reactions are among the most common irAEs. They may start subtly.
- New rash: Especially if it's spreading, raised, red, or tender
- Itching: Even without a dramatic visible rash
- Dry or peeling skin: Particularly if it becomes painful
- Mouth soreness or ulcers: If eating and drinking become uncomfortable
These symptoms are often manageable, but they still deserve a call. A mild rash can stay mild, or it can evolve.
Gut and digestion
The gastrointestinal tract is another frequent target. The pattern matters more than a single isolated episode.
- Diarrhea: More frequent stools than your usual pattern
- Abdominal cramping: Especially if it's new and persistent
- Blood or mucus in stool: This needs prompt attention
- Nausea with poor intake: Particularly when it's paired with weakness or dizziness
Patients often wait too long here because diarrhea feels common during cancer care. With immunotherapy, diarrhea may reflect colitis, and that can worsen quickly.
Lungs
New breathing symptoms should always be taken seriously.
- Shortness of breath: At rest or with activities that were previously easy
- New cough: Dry or persistent cough counts
- Chest tightness: Even if oxygen levels seem okay at home
- Breathing that feels “different”: Patients often describe this before the numbers change
A clinical overview of severe irAEs reports that ICI-related pneumonitis occurs in 2.5% to 5.0% of patients on monotherapy and 7% to 10% on combination therapy, with real-world incidence ranging from 7% to 19%. The same review notes that pneumonitis accounts for 35% of deaths in PD-1/PD-L1 inhibitor monotherapy, while immune-related myocarditis has an incidence of 0.09% to 2.4% and a fatality rate of 27% to 60%, making it the most dangerous irAE. These risks are outlined in this review of severe cardiovascular and pulmonary irAEs.
Any new chest pain, worsening shortness of breath, fainting, severe weakness, or a racing heartbeat should trigger immediate contact with your oncology team or emergency evaluation.
To hear the topic explained in patient-friendly language, this short video is useful:
Hormones and endocrine glands
Endocrine irAEs can be harder to spot because they don't always look dramatic.
| Body area | Symptoms worth reporting |
|---|---|
| Thyroid or pituitary | unusual fatigue, feeling cold, weight change, headaches, dizziness |
| Adrenal system | weakness, nausea, low appetite, lightheadedness |
| General hormone changes | mood shift, poor concentration, sleep disruption that feels out of proportion |
These problems often masquerade as “just cancer fatigue.” They shouldn't be dismissed.
Liver, nerves, and heart
Some irAEs are less common but more urgent.
- Liver concerns: Dark urine, yellowing of the eyes, right upper abdominal discomfort
- Nerve or muscle concerns: New numbness, weakness, drooping eyelids, trouble swallowing
- Heart concerns: Chest pain, palpitations, near-fainting, sudden exercise intolerance
If a symptom is new, persistent, and unexplained, report it. Patients do not need to decide which organ is involved before calling.
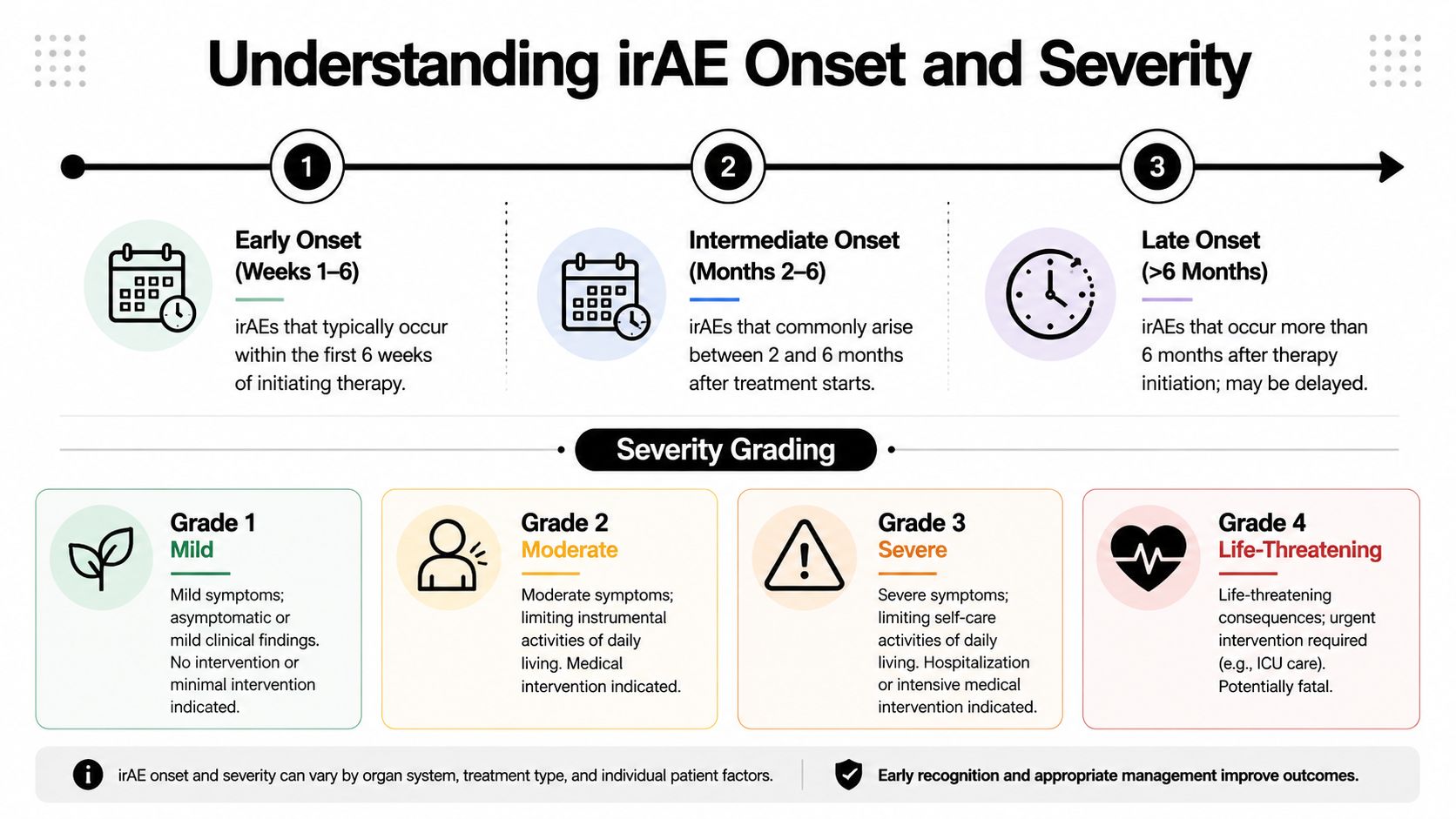
The Timing and Severity Grading of irAEs
One of the biggest misconceptions about immunotherapy is that if the first few treatments go smoothly, the risk has passed. That isn't how irAEs behave.
Some begin early. Skin reactions can show up sooner than deeper organ inflammation. Other problems emerge later, after the treatment has been working in the body for some time. A delayed symptom is still a treatment-related symptom until proven otherwise.
In a large cohort study of 795 patients hospitalized for irAEs after immune checkpoint inhibitor therapy, 14.7% of cases occurred 6 to 12 months after initial exposure and 10.8% presented more than 1 year after exposure. The same study found a median time to hospital admission of 2.7 months, with kidney-related and hematologic irAEs appearing especially often in the late setting, as reported in JAMA Network Open on late-onset hospitalized irAEs.
If you want a separate overview focused on timing patterns, this immunotherapy side effects timeline is helpful.
What grading means in real life
Doctors use a grading system to describe severity. Patients don't need to memorize formal criteria, but it helps to understand the logic.
- Grade 1: Mild symptoms. You're uncomfortable, but functioning. We may watch closely, use supportive care, and keep treatment going depending on the symptom.
- Grade 2: Moderate symptoms. Daily life is affected. This often changes the plan and may lead to holding immunotherapy.
- Grade 3: Severe symptoms. Normal activities become difficult or unsafe. These events usually require stronger treatment and closer monitoring.
- Grade 4: Life-threatening symptoms. These require urgent intervention and often hospitalization.
Why the timing matters
Late irAEs create two common problems. First, patients may not connect the symptom to treatment. Second, outside clinicians may not know immunotherapy is the likely trigger unless someone mentions it.
Delayed symptoms are often the most overlooked. A cough six months later still matters. So does new fatigue after treatment has stopped.
The practical takeaway is simple. Keep reporting symptoms for the entire period your oncology team tells you to remain on surveillance, even if treatment has been paused or completed.
How Doctors Diagnose and Monitor Your Symptoms
When a patient calls with a possible irAE, the first task is not to label it quickly. The first task is to answer a more important question: what else could this be? Infection, dehydration, blood clots, cancer progression, medication effects, and immune toxicity can overlap.
The first conversation
The workup usually starts with very specific questions:
- When did it start
- How fast is it changing
- What makes it worse
- What other symptoms are happening at the same time
- Did anything else change recently, including other medications
That history often tells us where to look next.
Tests that help sort it out
Blood work is commonly used to look for inflammation or organ irritation. Depending on the symptom pattern, the team may check liver function, kidney function, thyroid levels, blood counts, or markers that help evaluate heart stress.
Imaging may follow. A chest X-ray or CT scan can help when the issue is cough or shortness of breath. Abdominal imaging may help if pain or diarrhea is prominent. If the concern is endocrine, repeat lab trends often matter more than a single isolated result.
In some cases, a biopsy becomes the clearest way to distinguish immune inflammation from infection or cancer activity. Patients are often alarmed when a biopsy is recommended, but the reasoning is straightforward. The treatment paths are different, so the diagnosis must be as precise as possible.
Why routine monitoring matters even when you feel okay
Regular labs and symptom check-ins aren't busywork. They're how teams catch problems before the symptoms become obvious. Some irAEs declare themselves through bloodwork first. Others show up through a patient saying, “I'm not sure this is important, but I just don't feel like myself.”
That sentence matters more often than people realize.
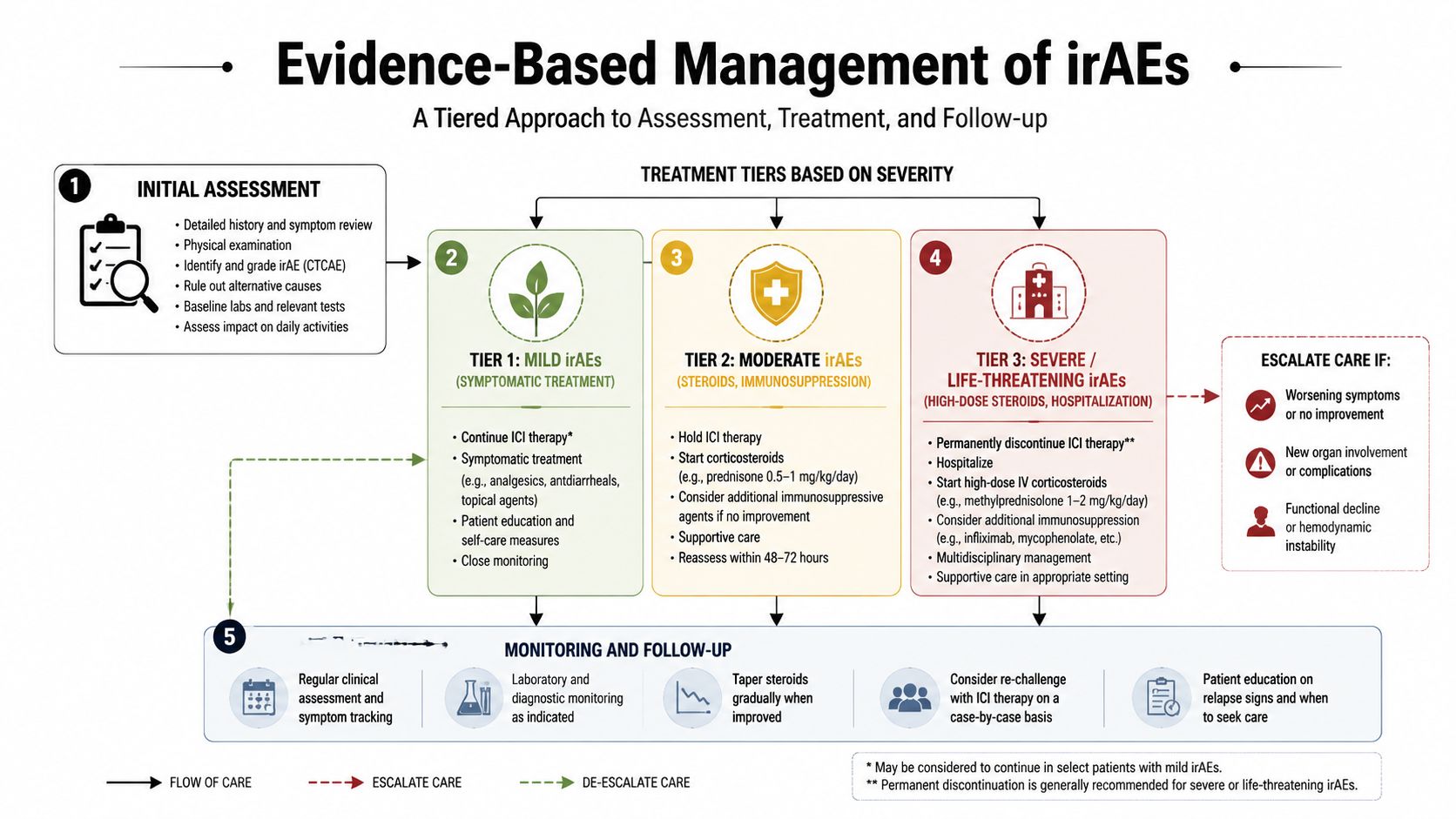
Evidence-Based Management of irAEs
Once an irAE is identified, treatment is guided by two things: which organ is involved and how severe the inflammation is. Good management is rarely dramatic. It is structured, stepwise, and responsive to change.
A broad clinical summary reports that the incidence of irAEs differs by inhibitor class, with adverse reactions occurring in about 54% of patients receiving CTLA-4 inhibitors, 27% receiving PD-1 inhibitors, and 17% receiving PD-L1 inhibitors. The same source states that when CTLA-4 and PD-L1 inhibitors are combined, incidence rises to 61%, and grade 3 or higher events occur in 22%, 7%, and 6% respectively for the single-agent classes. It also notes that management is tiered by severity, with corticosteroids used for grade 2 to 3 events and high-dose steroids or agents such as infliximab used for grade 3+ events, as outlined in Cancer Therapy Advisor's irAE management factsheet.
Mild problems and watchful treatment
Not every irAE needs aggressive intervention. Some mild skin reactions, mild itching, or limited symptoms can be handled with close follow-up and supportive medications.
That doesn't mean we ignore them. It means we match the response to the risk.
When steroids enter the picture
For many moderate irAEs, corticosteroids are the backbone of treatment. Drugs such as prednisone calm the immune system and reduce inflammation. If the problem is clearly immune-related and significant enough to interfere with daily function, immunotherapy is often paused while steroids begin.
Patients should know two things about steroids:
- They can work quickly, especially for inflammation-driven symptoms.
- They usually need a taper, because stopping abruptly can allow symptoms to rebound.
Severe events and escalation
When symptoms are severe, the treatment approach changes fast. Hospital-level care may be needed. High-dose steroids are commonly used, and if the irAE doesn't respond adequately, doctors may add another immunosuppressive medication such as infliximab for selected conditions like colitis.
Practical rule: The earlier a serious irAE is recognized, the more options we usually have and the less damage it tends to cause.
Chronic problems need a different mindset
Acute care is only part of the story. Some patients don't have a short burst of inflammation that resolves cleanly. They develop chronic endocrine or autoimmune-type issues that require long-term follow-up, medication adjustment, and coordination with other specialists.
That's one reason symptom tracking matters beyond oncology. Many families also juggle medications from other specialties. When side effects overlap, a careful framework helps. For that broader lens, this comprehensive guide for psychiatric medication side effects is a useful example of how structured monitoring can reduce confusion when multiple treatments are in play.
For patients comparing treatment experiences, this overview of cancer infusion side effects can also help distinguish common infusion reactions from immune-mediated toxicity.
What works and what usually backfires
- Works well: Early reporting, clear documentation, follow-up calls, gradual steroid taper when indicated
- Often backfires: Waiting until dehydration sets in, restarting treatment without reassessment, stopping steroids on your own because you feel better
Pausing Stopping and Restarting Immunotherapy
Few moments are more stressful than hearing that immunotherapy may need to be paused. Patients immediately wonder whether they're losing their chance to control the cancer. That fear is understandable, but it often oversimplifies the decision.
A pause is not the same as failure. In many cases, it is a strategic move to protect organs, reverse inflammation, and preserve options.
When a pause makes sense
Temporary interruption is common when symptoms are moderate or when the diagnosis is still being sorted out. If the team suspects an immune-mediated problem, it may be safer to hold treatment while evaluating the lungs, bowel, liver, endocrine system, or heart.
Permanent discontinuation is more likely when the irAE is life-threatening, very severe, or likely to recur with high risk. The decision depends on the organ involved, the speed of recovery, and whether the patient can be re-exposed safely.
Restarting can be reasonable
Nuance is important. Many patients hear only the risk side of the story. A more balanced perspective exists.
A review focused on rechallenge after irAEs reports that NSCLC patients who restart immune checkpoint inhibitors after temporary discontinuation have significantly longer progression-free survival and overall survival than those who do not, and that evidence supports the safety and efficacy of restarting in non-Grade 4 cases, as discussed in this review on ICI rechallenge after irAEs.
That doesn't mean every patient should restart. It means the conversation should be individualized, not reflexively shut down.
The decision framework patients can use
When discussing restart, ask your oncologist:
- Which organ was affected
- How severe was the event
- Has it fully resolved or stabilized
- Would restarting carry acceptable risk
- What monitoring plan would be used if treatment resumes
A carefully chosen restart after recovery can be a thoughtful cancer decision, not a reckless one.
The key is shared decision-making. Some patients accept a higher recurrence risk of toxicity because the anti-cancer benefit may be meaningful. Others decide the organ risk is too high. Both are reasonable when the decision is informed and individualized.
Your Urgent Reporting Pathway at Hirschfeld Oncology
When symptoms appear, the most important step is not guessing. It's contact.

Use a simple script when you call. State your treatment, the symptom, when it started, whether it's getting worse, and whether you have fever, chest symptoms, severe diarrhea, or trouble keeping fluids down. If you're short of breath, having chest pain, fainting, severe weakness, confusion, or rapid worsening, treat it as urgent.
For daytime concerns, call the clinic directly using the current office number you were given at registration or on your treatment paperwork. For nights, weekends, and holidays, use the after-hours contact instructions provided by your care team. If symptoms are severe or rapidly worsening, seek emergency care and make sure the treating team knows you're receiving immunotherapy.
Do not wait for the next appointment to mention a significant new symptom.
If you're navigating immunotherapy, late side effects, or difficult treatment trade-offs, Hirschfeld Oncology provides patient-centered cancer care, close symptom monitoring, and practical guidance for people facing complex or advanced cancers.
.png)
.png)




