




.png)


The words metastatic breast cancer can make everything else in the room go quiet. Many people hear only fragments after that. Stage 4. Spread. More treatment. Maybe immunotherapy.
If that's where you are right now, your questions are reasonable. Is immunotherapy used for breast cancer? Is it only for certain people? What do those biomarker results mean? What will treatment feel like in real life?
Immunotherapy for metastatic breast cancer isn't a cure-all, and it isn't the right fit for every subtype. But it has transformed the treatment approach for some patients, especially in specific biomarker-defined settings. What matters most is matching the right treatment to the biology of your cancer, your prior treatment history, and your goals.
A New Chapter in Treating Metastatic Breast Cancer
For years, treatment conversations for metastatic breast cancer centered mostly on chemotherapy, hormone therapy, and targeted drugs. Those treatments still matter. But immunotherapy added a new option by helping the immune system recognize cancer that it had previously ignored.
That shift matters because metastatic breast cancer is no longer understood as one single disease with one single pathway. Different subtypes behave differently. Some tumors are far more likely to respond to immune-based treatment than others.
One sign of progress is survival over time. Among patients ages 18 to 49 with metastatic breast cancer, five-year survival rose from 18% in 1992 to 1994 to 36% in 2005 to 2010, a change discussed alongside the growing use of newer targeted and immune-based strategies in FORCE's review of metastatic breast cancer remission and immunotherapy.
What this means for patients
Improved survival statistics don't tell any one person's story. They don't predict exactly how your cancer will behave or how well a treatment will work for you. But they do show something important: the outlook for metastatic breast cancer has changed, and treatment options are broader than they used to be.
Families often worry that "metastatic" means there are no meaningful choices left. That's not true. In many cases, there are multiple lines of treatment, biomarker tests that open specific options, and clinical trials that may fit later if standard therapy stops working.
Metastatic breast cancer is often treated as a long-term illness. The goal may be to shrink cancer, slow its growth, control symptoms, and preserve quality of life for as long as possible.
Why immunotherapy feels different
Chemotherapy attacks fast-growing cells. Targeted therapy blocks specific growth signals. Immunotherapy works differently. It tries to help your own immune system find and attack cancer cells.
For some patients, that difference isn't just scientific. It's practical. A treatment that teaches the immune system to keep working can sometimes produce responses that last longer than expected. That possibility is one reason immunotherapy gets so much attention, even though it still helps only selected groups of patients.
How Immunotherapy Teaches Your Body to Fight Cancer
Cancer doesn't survive only because it grows quickly. It also survives because it hides. Your immune system is built to notice danger, but cancer cells can learn how to blend in and send "don't attack me" signals.
That's the basic idea behind immunotherapy for metastatic breast cancer. Instead of directly poisoning cancer cells, these drugs try to remove the camouflage.
A visual can help make that clearer.
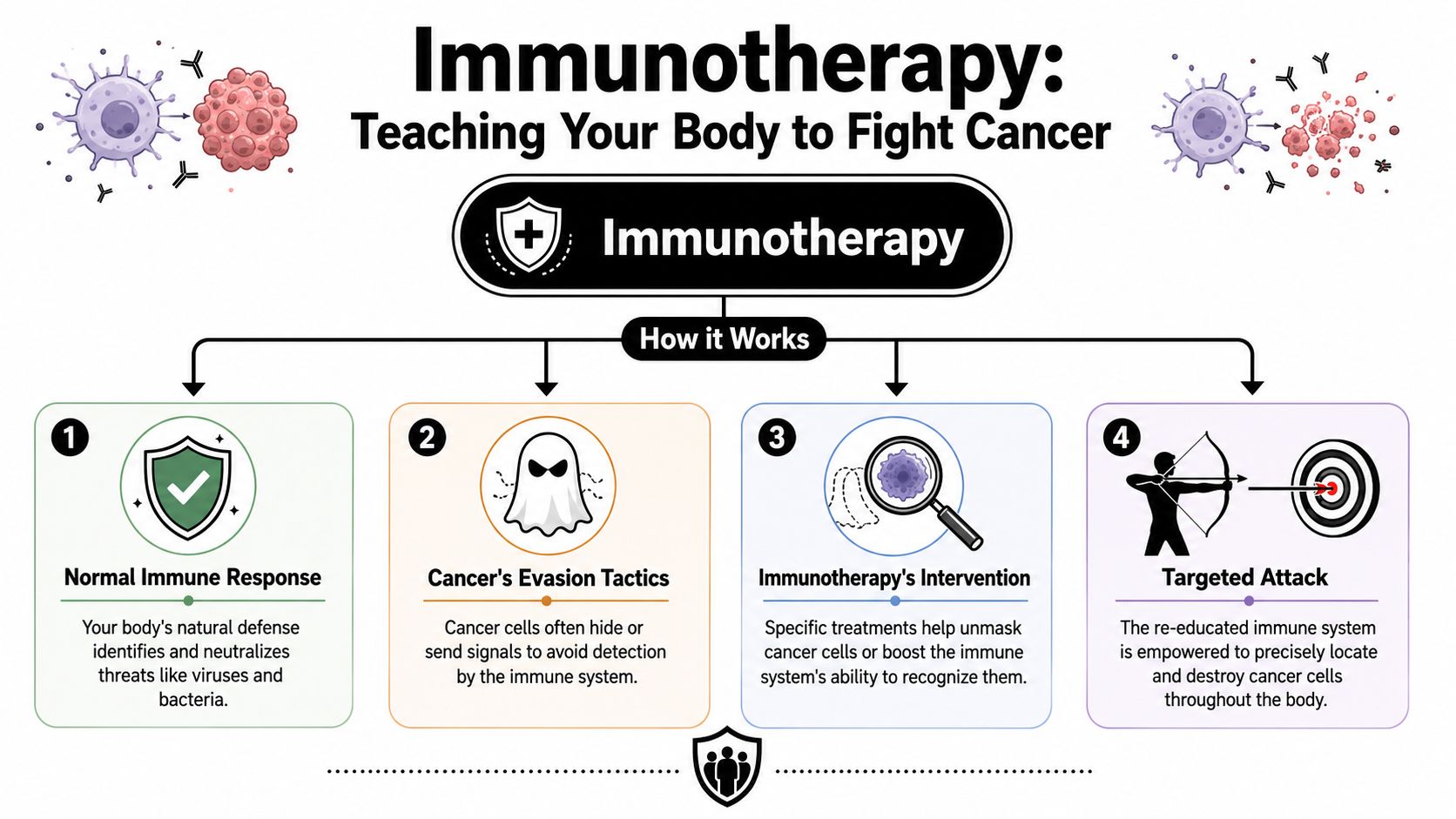
The simplest way to think about it
Think of your immune system as a security team. Its job is to patrol your body and remove threats. Cancer cells, however, can look enough like normal cells that the security team hesitates.
Checkpoint inhibitor drugs help by removing one of the "brakes" on immune cells, especially T cells. If you've wanted a plain-English overview of that process, this guide on how immunotherapy works for cancer is a helpful companion.
Here is the step-by-step version:
- Your immune system scans for threats. T cells are part of that defense.
- Cancer uses a hiding signal. Some tumor cells express PD-L1, a protein that interacts with PD-1 on T cells.
- That interaction shuts the T cell down. The immune cell gets the message that it shouldn't attack.
- Checkpoint inhibitors block that signal. When the signal is blocked, the T cell has a better chance of recognizing the cancer as dangerous.
What PD-1 and PD-L1 actually mean
These names sound technical because they are. But the idea is straightforward.
- PD-1 is a checkpoint on immune cells.
- PD-L1 is a matching signal that can appear on tumor cells and some immune cells.
- When they connect, the immune attack may slow down or stop.
A checkpoint inhibitor such as pembrolizumab interrupts that connection. It doesn't create a brand-new immune system. It helps the existing one work more effectively against cancer that's been escaping notice.
Later in the conversation, your oncologist may talk about whether your tumor is PD-L1 positive. That isn't just lab jargon. It's one of the practical clues doctors use to decide whether a checkpoint inhibitor is likely to help.
Some readers prefer hearing this explained aloud. This short video gives a patient-friendly overview.
Practical rule: Immunotherapy doesn't "boost" the immune system in a vague, general way. It changes a specific interaction so immune cells can better recognize cancer.
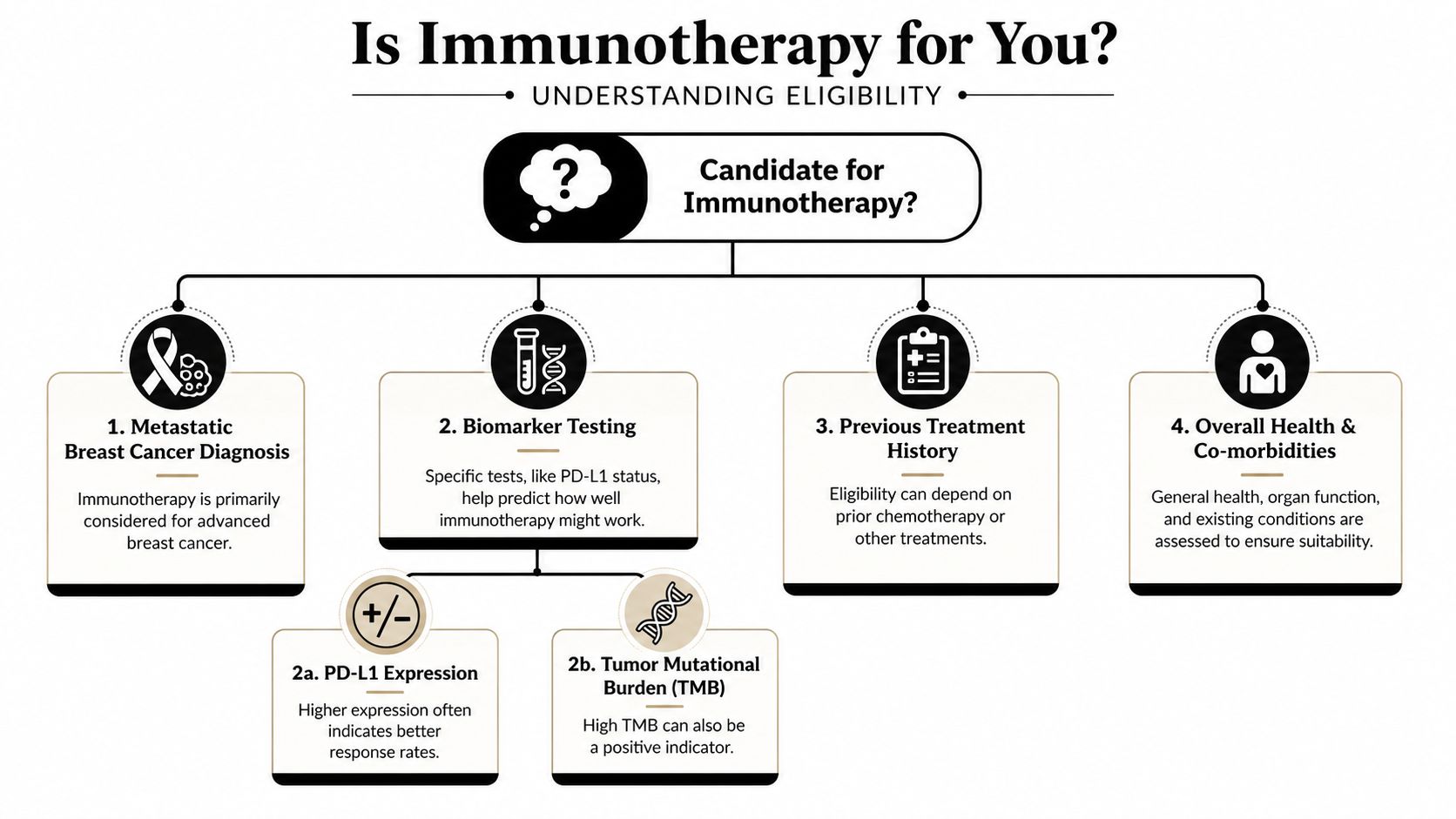
Who Is a Candidate for Immunotherapy
The most important question isn't whether immunotherapy exists. It's whether your cancer has the features that make it a reasonable option.
For breast cancer, candidacy is driven by subtype and biomarkers. Immunotherapy is not used the same way across all metastatic breast cancers. The clearest role today is in metastatic triple-negative breast cancer, often called TNBC.
TNBC means the cancer doesn't have the usual treatment targets of estrogen receptor, progesterone receptor, or HER2. Because those common targets are absent, oncologists look more closely at other features, including immune-related markers.
The key group most likely to benefit
For first-line metastatic TNBC, pembrolizumab plus chemotherapy is the standard of care when the tumor expresses PD-L1 with a combined positive score, or CPS, of 10 or higher, based on results from KEYNOTE-355 summarized in the Journal for ImmunoTherapy of Cancer review of immunotherapy biomarkers and treatment selection.
That sentence contains a lot of jargon, so let's slow it down.
- First-line means the first treatment used for metastatic disease.
- PD-L1 is the immune-related marker discussed earlier.
- CPS stands for combined positive score, a way the pathologist measures PD-L1 expression.
- CPS 10 or higher is the threshold that matters for this particular treatment decision in metastatic TNBC.
What a biomarker test means for you
When your oncologist sends tissue for biomarker testing, they aren't just collecting abstract data. They're trying to answer practical questions:
| Question | Why it matters |
|---|---|
| Is this truly triple-negative disease? | That shapes the overall treatment path. |
| Is the tumor PD-L1 positive? | That helps determine if checkpoint inhibition is appropriate. |
| What is the CPS score? | In metastatic TNBC, the threshold can affect eligibility for pembrolizumab with chemotherapy. |
Patients often feel uneasy when they hear, "We're waiting on pathology" or "We're waiting on biomarker results." But this waiting has a purpose. The results may change the treatment recommendation in a major way.
Other factors doctors weigh
Biomarkers don't make the decision by themselves. Your team also looks at:
- Prior treatment history. What you've already received can influence what comes next.
- Overall health. Autoimmune disease, organ function, and daily functioning all matter.
- Urgency of treatment. If cancer is causing rapid symptoms, your doctor may weigh speed and reliability carefully.
- Personal goals. Some patients prioritize the most aggressive tumor control. Others prioritize fewer clinic visits or less toxicity.
A good immunotherapy decision starts with two questions: what does the tumor biology show, and what matters most to the person living with it?
Approved Treatments and Combination Therapies
When patients hear "immunotherapy," they sometimes picture a broad category with many equivalent drugs. In metastatic breast cancer, the actual list is much narrower. The best-established checkpoint inhibitor in this setting is pembrolizumab (Keytruda), used for selected patients with metastatic TNBC based on biomarker testing.
Doctors also talk about immunotherapy in combination with chemotherapy because these treatments can work together. Chemotherapy doesn't only kill cancer cells. In some situations, it may also make the cancer more visible to the immune system by releasing tumor material that immune cells can recognize.
Why combination therapy is common
Pembrolizumab has shown activity by itself in metastatic TNBC. In heavily pretreated metastatic patients, pembrolizumab monotherapy produced an 18.5% overall response rate in the KEYNOTE-012 trial, as described in this review of immunotherapy in breast cancer published in PMC.
That same review also highlights why combinations draw so much interest. In the neoadjuvant setting, pembrolizumab plus chemotherapy reached a 60% pathologic complete response rate, compared with 20% for chemotherapy alone. Those aren't metastatic data, but they help explain why oncologists view chemotherapy and checkpoint blockade as partners rather than competitors.
Quick reference for current practice
| Drug Name (Brand Name) | Target | Approved For |
|---|---|---|
| Pembrolizumab (Keytruda) | PD-1 | Metastatic triple-negative breast cancer with appropriate PD-L1 expression in the approved setting |
| Dostarlimab (Jemperli) | Checkpoint pathway | Certain breast cancer patients with specific tumor markers, as described in regulatory use discussions of metastatic disease |
The exact chemotherapy partner, treatment schedule, and sequencing depend on your disease pattern, symptoms, prior therapies, and pathology results. That's why two patients with "metastatic breast cancer" may leave clinic with very different plans.
What treatment usually looks like in practice
Some patients receive immunotherapy and chemotherapy together from the start. Others aren't candidates because their cancer subtype or biomarkers don't fit the approved use. Others may discuss clinical trials if standard options have been exhausted.
This is also where expectations matter. An active drug can still fail in an individual person. A promising regimen can help one patient dramatically and do very little for another. That's frustrating, but it's the reality of metastatic cancer care.
The right question isn't "Is immunotherapy powerful?" It's "Is this the right immune-based treatment for this tumor, at this moment, for this patient?"
Managing Side Effects and Treatment Realities
Patients often ask whether immunotherapy is "easier" than chemotherapy. Sometimes it is. Sometimes it isn't. The side effects are different, and that's an important distinction.
Chemotherapy side effects usually happen because the drug affects fast-growing normal cells along with cancer cells. Immunotherapy side effects happen because the immune system can become overactive and inflame normal tissues. Doctors call these immune-related adverse events.

What side effects can feel like
A patient on treatment might say, "I'm more tired than usual," or "I've developed a rash," or "My bowels suddenly changed." Those details matter. Common immune-related problems can include fatigue, skin changes, diarrhea or colitis, thyroid problems, cough, or shortness of breath.
Some symptoms start subtly. A little more fatigue might seem like stress. Mild diarrhea might seem like something you ate. But with immunotherapy, small changes can be the first sign of inflammation that needs attention.
Here are the symptoms I tell families to report early:
- New bowel changes. Diarrhea, cramping, or blood can signal colitis.
- Breathing symptoms. New cough or shortness of breath needs prompt review.
- Skin changes. Rash or itching may be manageable, but your team should know.
- Hormone-related clues. Worsening fatigue, feeling unusually cold, dizziness, or headaches can point to thyroid or other endocrine changes.
The most important rule during treatment
Call your oncology team early. Don't wait to "see if it passes" for several days if something feels off.
Immune-related side effects are often manageable, but timing matters. Your team may pause treatment, order labs, prescribe steroids, or bring you in for evaluation. Fast communication can prevent a manageable problem from becoming a serious one.
If you're on immunotherapy and develop a new symptom, your first assumption shouldn't be that it's unrelated.
Managing expectations honestly
Immunotherapy can be life-changing for some patients. It can also fail completely. Both statements are true.
That emotional tension is hard. Patients want hope without false reassurance. Families want a plan without pretending uncertainty doesn't exist. A good oncology conversation leaves room for both. We hope for a meaningful response, we watch carefully, and we pivot if the treatment isn't helping or is causing too much harm.
Your Immunotherapy Journey at a NYC Cancer Center
In New York City, one of the hardest parts of cancer care isn't only choosing treatment. It's navigating logistics while you're already overwhelmed. Pathology reports, biomarker testing, infusion schedules, scan timing, transportation, work leave, and second opinions can pile up quickly.
A typical immunotherapy journey starts with a careful review of your records. Your oncologist looks at the original biopsy, confirms the breast cancer subtype, reviews where the cancer has spread, and checks whether enough tissue is available for biomarker testing. If testing hasn't been completed, it may be ordered on prior tissue or on a new biopsy.
What visits usually include
At an outpatient infusion practice such as Hirschfeld Oncology's Brooklyn cancer center, the process generally includes consultation, lab monitoring, infusion visits, and periodic scans to see whether treatment is working. The team also tracks side effects closely, because a treatment plan is only useful if you can tolerate it safely.
Patients often want to know how long the infusion itself takes and how often they need to come in. The answer depends on the specific regimen, whether chemotherapy is being given at the same visit, and how your doctor structures monitoring. Your team should give you a written schedule, not just a verbal summary.
Questions worth bringing to your appointment
Bring a notebook, or bring someone who can take notes. Ask direct questions such as:
- What biomarkers has my tumor been tested for?
- Am I a candidate for checkpoint inhibitor treatment? Why or why not?
- Will immunotherapy be given alone or with chemotherapy?
- What symptoms should trigger a same-day call?
- How will we know if it's working?
For some NYC patients, the treatment journey also overlaps with concerns about delays in diagnosis, insurance issues, or fragmented care. If that applies to your family, these resources after delayed cancer diagnosis in NYC may help you identify practical support options while treatment planning is underway.
Finding Hope in Clinical Trials and Next Steps
Standard treatment matters, but it isn't the end of the story. Clinical trials are where the field keeps moving, especially for patients whose tumors don't match current approved uses or whose cancer has progressed after prior therapy.
One area drawing real interest is tumor-infiltrating lymphocyte therapy, often shortened to TIL therapy. This is a highly personalized approach. Doctors collect immune cells that have already entered the tumor, expand or prepare them, and then return them to the patient in an effort to create a stronger anti-cancer response.
In a phase I clinical trial, TIL therapy led to significant tumor shrinkage in 50% of the six women who received the infusion, and one patient from an earlier cohort remained cancer-free, according to the National Cancer Institute report on personalized immunotherapy for metastatic breast cancer. That's early research, not a guarantee, but it shows why trial discussions are worth having.
When to ask about a trial
Some patients think clinical trials are only for the very end of treatment. That's not always true. It can be smart to ask earlier, especially if:
- Your tumor doesn't fit the approved biomarker profile for current immunotherapy.
- Standard treatment has stopped working and you want to know what's next.
- You want access to emerging strategies while you're still strong enough for trial participation.
If you want a starting point for that conversation, this overview of clinical trials for breast cancer can help you understand how trials are structured and what questions to bring to clinic.
The next conversation to have
Ask your oncologist for three things in plain language:
- Your exact breast cancer subtype.
- Your biomarker results, including whether PD-L1 testing was done.
- The reason your doctor does or doesn't recommend immunotherapy now.
Those answers won't solve everything. But they turn a confusing idea into a treatment decision grounded in your biology, not in headlines or hope alone.
If you're weighing immunotherapy for metastatic breast cancer and want help understanding your subtype, biomarker results, treatment options, or possible clinical trial pathways, you can request a consultation through Hirschfeld Oncology. A careful review of records, pathology, prior treatments, and treatment goals can help clarify what options make sense now.
.png)
.png)




