




.png)


A stage 4 kidney cancer diagnosis usually lands in the middle of ordinary life. One phone call, one scan result, one clinic visit, and suddenly your family is learning a new language made of biopsy reports, metastases, immunotherapy, and treatment plans. What's needed in that moment isn't more alarm. They need a clear explanation of what decisions matter now, what options are real, and where hope realistically fits into the picture.
The first thing I want patients to know is this. Stage 4 kidney cancer treatment is no longer a conversation limited to comfort care alone. The situation has evolved. There are now about a dozen FDA-approved treatments for metastatic kidney cancer, and immunotherapy is a cornerstone of first-line treatment. Outcomes are still serious, but they are not frozen in the past. The U.S. SEER registry reports a 20.3% five-year relative survival for distant kidney and renal pelvis cancer, and one academic center reports 25% five-year survival for stage 4 patients compared with 11% nationally in earlier eras, showing how much treatment has evolved over time according to UT Southwestern's review of metastatic kidney cancer progress.
That change matters because it shifts the question. The question is no longer only, “Is there anything to do?” The better question is, “Which treatment path fits this person's disease, strength, symptoms, and goals?”
Your Stage 4 Kidney Cancer Diagnosis A New Perspective
Why this diagnosis means something different today
“Stage 4” still means the cancer is advanced. No careful oncologist should minimize that. But advanced does not mean there are no meaningful options, and it does not mean every patient follows the same course.
What has changed most is that treatment has become strategic and personalized. Some patients need rapid disease control because symptoms are pressing. Others are stable enough to think carefully about sequencing therapies over time. Many can be treated in a way that aims not only to slow the cancer, but also to preserve day-to-day living.
Practical rule: Don't treat the words “stage 4” as a complete prognosis. They describe the extent of spread, not the whole story of how your cancer will behave or how you'll respond.
Families often expect a single recommendation, as if there is one correct drug and one standard timeline. In reality, modern stage 4 kidney cancer treatment works more like a series of informed decisions. Your care team weighs where the cancer has spread, how quickly it's growing, whether you have symptoms, how strong you feel, and what trade-offs you're willing to accept.
Hope that is grounded, not false reassurance
Hope is most useful when it's specific. In metastatic kidney cancer, it comes from the fact that the field now has multiple active treatments and better first-line tools than it used to. Immunotherapy changed the tone of care because it gave oncologists a way to pursue durable control in some patients, not just short-lived shrinkage.
That doesn't mean every treatment works for every person. Some cancers respond well and stay controlled for a long time. Others resist an early regimen and require a change in plan. Side effects can also become a major part of decision-making. But the days when this disease was approached as uniformly untreatable are over.
A better way to think about this diagnosis is as the start of a partnership. Your oncologist's job is not merely to prescribe. It is to help you choose wisely, monitor closely, adjust quickly, and keep your quality of life in view at every step.
Understanding Your Diagnosis and Prognosis Factors
What stage 4 actually means
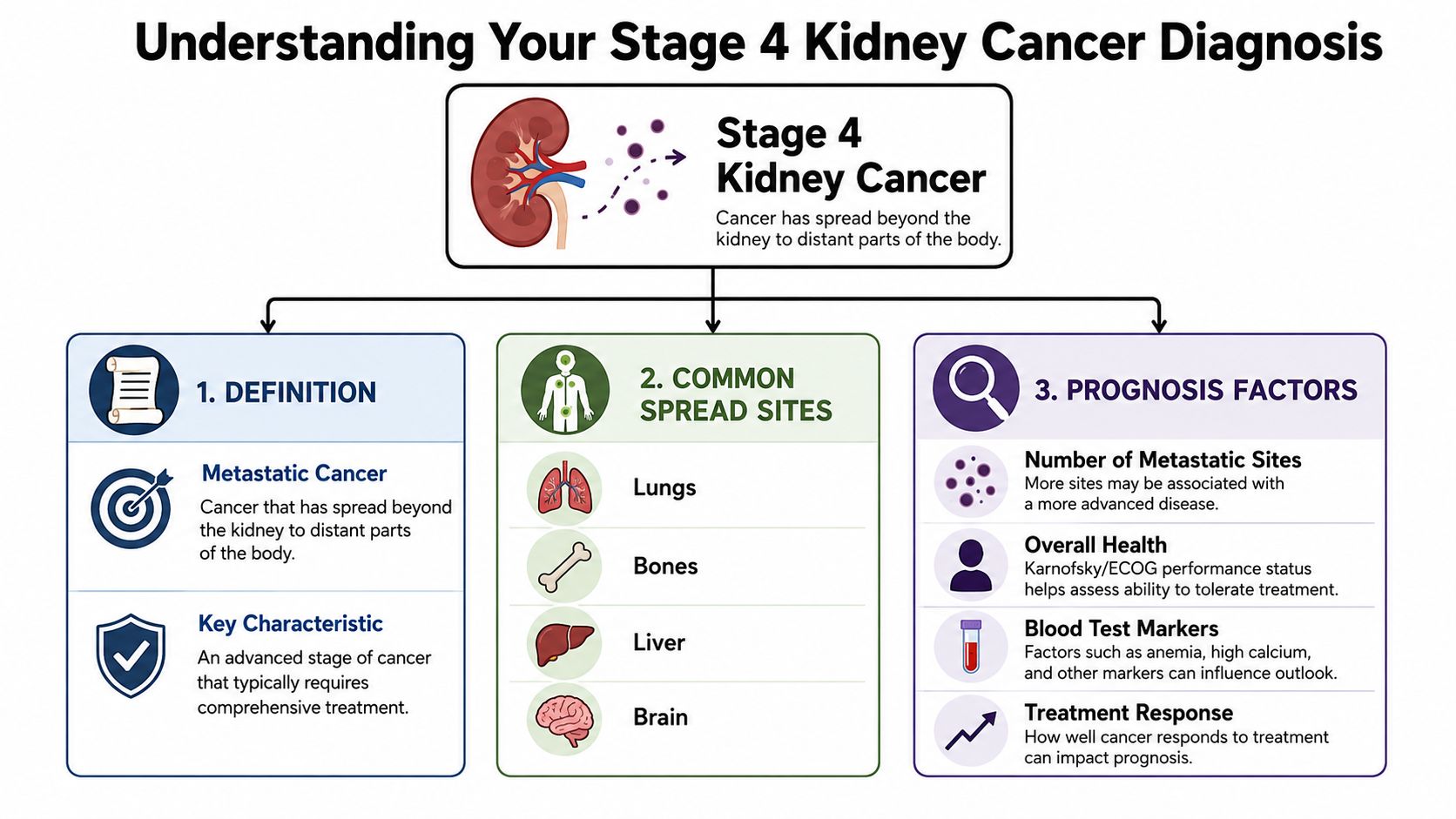
Stage 4 kidney cancer usually means the cancer has spread beyond the kidney to distant parts of the body. You may hear the words metastatic or advanced renal cell carcinoma. Those terms can sound abstract, but the practical meaning is straightforward. The disease is no longer confined to one organ, so treatment usually has to address the whole body, not just the kidney itself.
About 15% of kidney and renal pelvis cancers are diagnosed as distant or metastatic, and the U.S. age-adjusted incidence is 18.0 cases per 100,000 people per year, according to this review of metastatic renal cell carcinoma. The same review notes that in advanced disease, modern systemic therapy has produced a radiological response in 26% to 32% of patients, and one neoadjuvant series reported a 28.3% median reduction in primary tumor diameter. Those numbers help explain why treatment now often combines more than one approach rather than relying on surgery alone.
Why prognosis is personal
Patients often ask for a number. That's understandable, but a single number rarely helps much because prognosis depends on several factors working together.
Two of the most important are risk category and performance status. Risk category uses clinical features and bloodwork to estimate how aggressive the disease may be. Performance status is simpler. It asks how well your body is functioning in real life. Can you walk around normally? Work? Cook? Climb stairs? Spend most of the day in bed?
I often tell families to think of performance status like the overall condition of a car before a long trip. Two cars may be headed down the same road, but if one engine is already struggling, you choose a different speed, route, and maintenance plan. Cancer treatment works the same way.
For some patients, molecular features and tumor subtype also shape decisions. If you want a plain-language overview of how personalized cancer planning is evolving, this explanation of precision oncology is a useful starting point.
The questions that matter most early
Bring these questions to your first serious treatment discussion:
- How much disease is present: Is the cancer limited to a few areas, or is it widely spread?
- How fast is it acting: Do the scans and symptoms suggest a slower course or an urgent one?
- How strong is the patient today: Can they tolerate combination therapy, or is a gentler start wiser?
- What is the immediate goal: Shrink tumors quickly, control symptoms, delay progression, or all of the above?
The most useful prognosis is the one that explains why your doctor is recommending a specific plan for you, not an average patient in a database.
Your First-Line Treatment Options
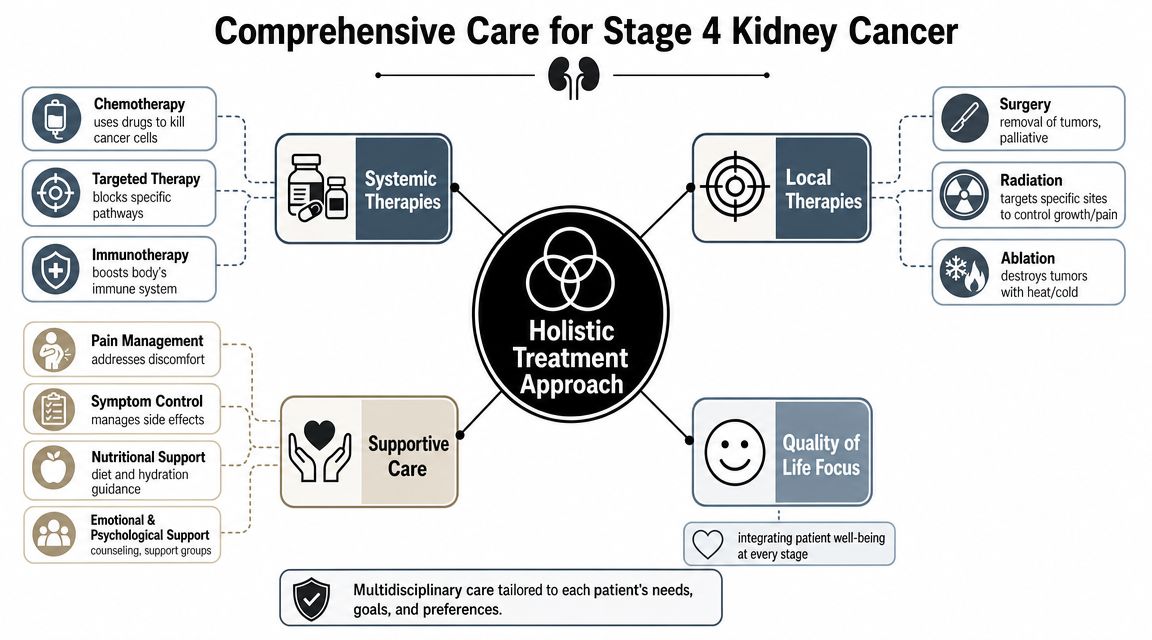
Stage 4 kidney cancer treatment often begins with systemic therapy, meaning treatment that travels through the body to reach cancer wherever it is. The backbone of modern first-line care is usually some combination of immunotherapy and targeted therapy.
How the main drug types differ
Immunotherapy helps the immune system recognize and attack cancer more effectively. These drugs are often given by IV infusion. They can produce durable control in some patients, but they can also trigger immune-related side effects that affect organs such as the skin, bowel, liver, lungs, or hormone glands.
Targeted therapy blocks growth signals or blood vessel pathways that kidney cancer uses to survive. Many of these medicines are pills. They can be very effective, but side effects like fatigue, diarrhea, mouth soreness, hand-foot symptoms, and high blood pressure can shape whether a regimen remains tolerable.
The National Cancer Institute lists several evidence-based first-line regimens for stage IV renal cell carcinoma, including ipilimumab plus nivolumab, pembrolizumab plus axitinib, pembrolizumab plus lenvatinib, and nivolumab plus cabozantinib, with surgery reserved for selected patients rather than used automatically in everyone, as outlined in the NCI kidney cancer treatment PDQ. If you want more background on the immune side of these regimens, this overview of immunotherapy for stage 4 cancer may help frame the discussion.
Common First-Line Combination Therapies for Stage 4 Kidney Cancer
| Combination | Type | How It Works | Key Considerations |
|---|---|---|---|
| Ipilimumab plus nivolumab | Dual immunotherapy | Stimulates immune attack through checkpoint blockade | Often considered when durable immune control is a central goal. Requires close monitoring for immune-related toxicity. |
| Pembrolizumab plus axitinib | Immunotherapy plus targeted therapy | Combines immune activation with blockade of cancer growth and blood vessel signaling | Often useful when both response and disease control are priorities. Includes IV treatment plus oral medication. |
| Pembrolizumab plus lenvatinib | Immunotherapy plus targeted therapy | Pairs checkpoint inhibition with a potent targeted agent | Can be effective, but side effects may require dose adjustments and careful follow-up. |
| Nivolumab plus cabozantinib | Immunotherapy plus targeted therapy | Combines immune checkpoint therapy with targeted inhibition of tumor signaling pathways | Strong option when active disease control is needed, though tolerability becomes a major part of management. |
What works on paper versus what works for you
Practicality is central to medicine. A regimen can be very strong scientifically and still be the wrong opening move for a particular patient.
Someone who is still active, eating well, and ready for a more intensive approach may choose a combination with a higher risk of side effects because the potential upside justifies it. Another patient with frailty, weight loss, or multiple medical problems may need a plan that is easier to tolerate, even if it looks less aggressive on a chart.
A good example of this trade-off comes from a stage 4 kidney cancer trial reported by Memorial Sloan Kettering. Adding cabozantinib to standard treatment increased disease control to about 87% compared with 55%, and extended median time to progression to 16.9 months compared with 11.3 months, according to MSK's report on the cabozantinib combination trial. The cost of that gain was more toxicity, including issues such as dose interruptions, hypertension, diarrhea, and fatigue.
The best first-line regimen isn't the one with the most impressive headline. It's the one a patient can start, stay on, and benefit from without losing too much of daily life in the process.
Questions worth asking before you start
- Will this regimen be IV, oral, or both
- Which side effects are most likely to affect my daily routine
- How will we know early if it's helping
- What is the backup plan if toxicity becomes a problem
- Would a different first choice better match my work, caregiving, or travel realities
Those questions don't weaken care. They improve it.
Navigating Later Lines of Treatment
One of the most important things to understand early is that treatment rarely ends with the first regimen. If the cancer stops responding, that doesn't mean options have run out. It means the strategy changes.
Treatment is often a sequence, not a single shot
Oncologists think about metastatic kidney cancer over time. The first treatment aims to control disease and set the pace. Later treatments are chosen based on what happened with the first one. Did the cancer shrink? Stay stable? Progress quickly? Did side effects become the main problem? Those answers guide the next move.
That process is called sequencing. It matters because kidney cancer often remains treatable across multiple lines if decisions stay organized and the patient stays supported.
What later-line decisions usually depend on
Later treatment choices often hinge on a few practical questions:
- What did the first therapy contain: If you started with an immune-based regimen, your next step may lean more heavily on targeted therapy.
- Why was the first regimen stopped: Cancer growth and drug intolerance are different problems and lead to different next options.
- How is the patient functioning now: A person who tolerated treatment well can often consider more active next-line therapy than someone who has become medically fragile.
- What pace does the disease have now: Slow progression allows more deliberation. Symptomatic or accelerating disease may require a quicker pivot.
A useful benchmark comes from the cabozantinib data already noted earlier. In that trial, adding cabozantinib improved disease control to about 87% versus 55% and extended median time to progression to 16.9 months versus 11.3 months. The larger lesson is not just that one drug helped. It's that effective sequencing can prolong control when the right agent is introduced at the right moment.
Real trade-offs in later treatment
Second- and third-line care isn't just about finding another drug. It's about matching the next therapy to the patient you are now, not the patient you were months earlier.
Sometimes that means switching to a medicine with a different side-effect profile because the body needs a break from the first regimen's toxicities. Sometimes it means choosing a treatment that can be monitored closely in the outpatient setting. In selected situations, clinicians may also consider lower-intensity approaches when preserving function matters more than maximal intensity.
A change in treatment is not a failure. In advanced kidney cancer, it's often a planned part of good care.
The right mindset is long-game thinking. You want every line of therapy to do useful work while leaving enough strength for the next decision.
Beyond Systemic Drugs Local and Supportive Care
Drug therapy gets most of the attention, but many of the most important decisions in stage 4 kidney cancer treatment involve care around the drugs. Surgery, radiation, symptom control, and supportive services often make the difference between merely receiving treatment and living through treatment in a manageable way.
When local treatment still matters
Even in stage IV disease, local treatment can still play a role. According to guidance from the Canadian Cancer Society, options such as nephrectomy, palliative radiation for pain, and even active surveillance for asymptomatic patients may be appropriate depending on disease burden, symptoms, and overall fitness, as described in this stage IV kidney cancer treatment overview.
That means surgery is not automatically off the table just because the cancer has spread. In selected patients, removing the kidney can still make sense. The key phrase is selected patients. Surgery may be considered when a person has a limited burden of metastases, good overall function, or a specific reason to remove the primary tumor, such as bleeding, pain, or a plan that combines surgery with systemic treatment.
Radiation has a different role. It usually doesn't treat the whole disease, but it can be extremely effective for specific symptoms. Bone pain, bleeding, or a troublesome metastatic spot may improve significantly with targeted radiation.
Supportive care is active care
Supportive care does not mean giving up. It means reducing the burden of both the cancer and its treatment so the patient can keep going.
That often includes:
- Pain control: Bone metastases, abdominal pressure, and post-treatment discomfort should be addressed early, not after they become overwhelming.
- Fatigue management: This may involve medication review, hydration, nutrition support, sleep strategies, and adjusting treatment intensity.
- Nausea and appetite support: Small changes in supportive medications can dramatically improve a patient's ability to eat and maintain strength.
- Home-based help: Families managing symptoms between visits may benefit from practical guidance on palliative care at home, especially when comfort, dignity, and daily support become central concerns.
For a broader oncology perspective, this discussion of integrating palliative care early in oncology treatment pathways for better quality of life captures why symptom-directed care belongs early, not only at the end of treatment.
Sometimes observation is the right move
Not every patient needs immediate systemic therapy the day stage 4 disease is identified. If someone is asymptomatic or too unwell for treatment right away, careful observation can be reasonable. This is one of the least understood parts of advanced cancer care.
Observation is not neglect. It is a decision to avoid treatment toxicity until treatment is more clearly necessary or more likely to help. That approach requires close follow-up and honest communication, but in the right setting it can be a thoughtful, patient-centered choice.
Relief of pain, preservation of energy, and time at home are not secondary outcomes. For many patients, they are part of the main treatment goal.
Finding Your Path and Seeking Specialized Care
A first visit after a stage 4 kidney cancer diagnosis often begins with one question: “What should we do first?” The hard part is that there may be more than one reasonable answer. One patient may be best served by starting combination systemic therapy soon. Another may need a second opinion about surgery, radiation, or a clinical trial before choosing a first treatment. A third may need time to recover strength so that treatment is more tolerable and more likely to help.

What specialized care adds
Specialized care adds experienced judgment.
In stage 4 kidney cancer treatment, the right choice depends on more than the drug list. It depends on pace of disease, symptoms, kidney cancer subtype, sites of spread, kidney function, other medical problems, and performance status, meaning how well a person is able to function day to day. It also depends on something just as important: what the patient wants life to look like during treatment.
Two people can have the same diagnosis on paper and need different plans in practice. Someone who is active, working, and willing to accept more side effects for a stronger first attempt at disease control may choose differently from someone who is losing weight, resting much of the day, or trying to protect time and energy at home. Neither goal is wrong. The treatment plan should fit the person, not the other way around.
Teams that treat metastatic kidney cancer regularly are often better at judging these trade-offs. They tend to recognize earlier when side effects are becoming too costly, when a dose change may preserve benefit, and when it makes more sense to switch strategies than to keep pushing a regimen that is wearing a patient down.
Clinical trials should come up early in that discussion. For the right patient, a trial may be a sound first or second step, not only a later option after standard treatments stop working.
Questions that help you choose your team
A second opinion is often useful when the treatment choices are close or the reasoning is not clear. Ask plain questions and listen for plain answers:
- How often do you treat metastatic kidney cancer
- What factors make you recommend immune-only treatment versus an immune-plus-targeted combination
- When do you involve surgeons, radiation oncologists, or palliative care clinicians
- How do you watch for side effects, and how quickly can patients reach your team between visits
- Do you discuss clinical trials early if they fit my goals and health status
- How will you adjust the plan if my priorities change
Here is a useful primer to watch as you think through how advanced cancer decisions are made in practice:
Building a plan around your life
The best plan is medically sound and livable.
Some patients want the most active treatment that offers a real chance of longer control, even if it means more clinic time, closer monitoring, and a higher risk of side effects. Others want to protect energy for work, parenting, travel, or feeling well enough to be present at home. Many want both, and that is where ongoing discussion matters. Priorities can change after treatment begins, and the care plan should be able to change with them.
Shared decision-making is a practical process. The oncology team explains the expected benefits, the likely burdens, and what the backup plan looks like if the first approach does not go as hoped. Patients and families explain what matters most right now, what side effects feel acceptable, and what trade-offs do not fit their goals.
For patients seeking a consultation in New York City, one option is Hirschfeld Oncology, a Brooklyn practice and infusion center that uses individualized oncology planning, including immunotherapy, targeted therapy, low-dose chemotherapy, and symptom-focused monitoring for complex and advanced cancers. Whether you meet with that group or another experienced team, look for the same standards: clear recommendations, careful follow-up, and a willingness to revise the plan when the cancer changes or your goals do.
You do not need to memorize every drug name before your next appointment. You do need a team that can explain the choices clearly, respect your priorities, and help you make decisions one step at a time.
If you or a loved one is weighing treatment options for advanced cancer and want a more personalized discussion of risks, benefits, and tolerability, Hirschfeld Oncology can be a useful place to start learning about individualized care pathways and requesting a consultation.
.png)
.png)




