




.png)


Only 72.7% of women ages 18 to 44 in the United States had a well-woman visit in the past year, according to America's Health Rankings. For an oncology audience, that number lands differently. I spend my days thinking about what happens when disease is found late, when symptoms finally appear, when treatment becomes harder and the margin for error gets smaller.
That's why the annual well woman exam deserves more respect than it usually gets. It isn't a formality. It's one of the few routine visits designed to catch problems before they announce themselves, and that matters because early breast and cervical cancers often don't cause obvious symptoms.
For patients living with cancer, survivors rebuilding after treatment, and caregivers trying to keep a loved one on track, this visit belongs in the same conversation as scans, pathology reports, treatment decisions, and survivorship planning. Preventive care and oncology are connected much more tightly than many people realize.
Why Your Annual Exam Is More Than Just a Checkup
The usual mistake is to think of the annual well woman exam as basic maintenance. In practice, it's much closer to risk surveillance. It creates a protected space to review symptoms, changes in menstrual patterns, sexual health concerns, family history, and screening needs before a small issue becomes a serious one.
That matters because cancer care often starts long before a biopsy. It starts when someone mentions new pelvic pain, unexpected bleeding, nipple changes, bloating that doesn't fit the usual pattern, or a family history that should trigger closer attention. A well-woman visit gives those details a place to be heard and acted on.
For people already familiar with oncology, the value is even clearer. We know that many cancers are more manageable when found early. We also know that viral risk matters in cancer prevention, especially in cervical disease. If you want a clear explanation of that connection, this discussion of how viruses can cause cancer helps frame why routine gynecologic care is not separate from cancer prevention.
Practical rule: Don't judge the value of this visit by how healthy you feel that day. Preventive care works best before symptoms force the issue.
There's also a systems issue behind the statistic. When nearly a third of eligible women miss this visit, the gap doesn't just reflect scheduling inconvenience. It often reflects fear, prior bad experiences, cost concerns, caregiving burdens, treatment fatigue, or the belief that “no symptoms” means “no need.” In oncology, that logic rarely serves patients well.
The annual well woman exam is a quiet form of self-advocacy. It doesn't feel dramatic. It often feels ordinary. But ordinary, repeated preventive care is one of the strongest tools medicine has.
The True Purpose of a Well-Woman Visit
The purpose of this visit is to make gynecologic and breast care specific to your risks, symptoms, treatment history, and plans. In oncology, that matters because cancer prevention and earlier detection rarely depend on one dramatic finding. They depend on small details being taken seriously before they become advanced disease.

It centers decisions that change risk over time
A strong well-woman visit should account for fertility goals, contraception, pregnancy plans, sexual health, menopause, and symptom patterns. Those topics are not separate from cancer care. They shape which screenings make sense, which medications are realistic, and whether a symptom deserves monitoring, imaging, referral, or biopsy.
For a survivor, the trade-offs are often more complicated. Tamoxifen can change bleeding patterns. Aromatase inhibitors can worsen dryness and pain with intercourse. Prior pelvic radiation can alter tissue, increase discomfort, and make a routine exam feel anything but routine. A thoughtful visit puts those facts together instead of treating each complaint in isolation.
It gives clinical meaning to symptoms patients often minimize
Patients often bring up concerns late because they seem minor, embarrassing, or expected after treatment. I would rather hear about a symptom early and find a benign explanation than hear about it months later after it has become harder to sort out.
Common examples include painful intercourse, vulvar irritation, persistent bloating, urinary urgency, nipple changes, breast skin thickening, bleeding after menopause, or pelvic pressure. Any one of those may turn out to be noncancerous. Some point to treatment effects, infection, hormonal shifts, pelvic floor dysfunction, or benign breast disease. Some require a closer look because the differential diagnosis includes cervical, uterine, ovarian, vulvar, vaginal, or breast cancer.
Family history belongs in the same discussion. A brief mention that several relatives had breast, ovarian, pancreatic, or prostate cancer can change what happens next. It may prompt a referral for counseling about genetic testing and hereditary cancer risk, which can affect screening, prevention, and sometimes treatment decisions for the whole family.
It creates a plan, not just a record
The best visit ends with clear follow-through. That may mean routine screening on schedule. It may mean a pelvic ultrasound, diagnostic breast imaging, HPV-based screening at the right interval, symptom treatment, pelvic floor therapy, or referral to gynecologic oncology if something does not fit a benign pattern.
That planning matters for people who already know oncology well. Survivors and caregivers understand that delayed evaluation is rarely neutral. Persistent symptoms can reflect treatment effects, but they can also signal recurrence, a second primary cancer, or a preventable problem that is easier to manage early.
If it helps, bring notes. Write down symptoms you have normalized, prior cancer treatment that could affect the exam, and the questions you keep postponing. Patients often benefit from broader support around strength, recovery, and daily function too, and this resource offers expert women's wellness advice that can complement medical care.
A strong annual well woman exam turns scattered concerns into a practical prevention and follow-up plan.
What to Expect During Your Exam
For many patients, the hardest part of a well-woman visit is not the exam itself. It is the fear that a routine appointment could uncover something serious. In oncology, I see the other side of that fear too. A symptom mentioned early can lead to a simple explanation or an earlier diagnosis, and timing often changes what treatment looks like.
The visit usually starts with a focused history. Expect questions about bleeding patterns, pelvic pain, discharge, urinary changes, sexual health, menopause symptoms, medications, prior surgeries, pregnancies, and family history. For cancer patients and survivors, this is the point to mention prior chemotherapy, radiation, endocrine therapy, risk-reducing surgery, lymphedema, vaginal dryness, pain with intercourse, or any new symptom that feels small but persistent.
That conversation guides the rest of the appointment. A patient with postmenopausal bleeding needs a different workup than a patient who feels well and is due for screening. A breast cancer survivor on endocrine therapy may need a closer discussion of vulvovaginal symptoms and bone health. A woman with bloating, early satiety, and pelvic pressure may need prompt imaging or referral rather than reassurance alone.
The physical exam is customized, not automatic. Basic measurements such as blood pressure and weight are often recorded first. After that, the clinician decides which parts of the exam are useful based on your age, symptoms, treatment history, and current risk.
A breast exam usually includes inspection and palpation to check for a new mass, skin dimpling, nipple inversion, discharge, focal tenderness, or asymmetry. If you have already been through a call-back mammogram after screening, this is a good time to ask how that result affects future imaging and whether your surveillance plan still fits your risk.
A pelvic exam can include several parts:
- External exam: inspection of the vulva and surrounding skin for lesions, irritation, atrophy, color change, scarring, or signs of infection
- Speculum exam: placement of a speculum so the vagina and cervix can be seen directly, and so cervical samples can be collected if screening or testing is due
- Bimanual exam: gloved fingers in the vagina with the other hand on the abdomen to assess tenderness, uterine size, pelvic masses, or fullness
Patients often ask which part will hurt. The honest answer is that discomfort varies. Pelvic floor tension, prior trauma, treatment-related atrophy, active infection, and anxiety can all make the exam harder. A careful clinician can slow down, use a smaller speculum, add lubricant when appropriate, explain each step before it happens, and stop if pain becomes more than expected.
Cervical screening is often misunderstood, especially by survivors who have had years of imaging, labs, and follow-up visits. A Pap test checks cervical cells for abnormal changes. An HPV test looks for high-risk viral types linked to cervical cancer. You may need one, both, or neither at a given annual visit, depending on your age, prior results, hysterectomy status, immune status, and history of cervical precancer or cancer.
The annual visit and the screening interval are separate decisions. Some women need cervical screening that day. Others need symptom evaluation, medication management, or a focused exam even when no Pap or HPV test is due.
If your history is medically complex, bring records or a short written summary. It helps to securely organize your family's medical info before the appointment so dates of biopsies, surgeries, pathology results, imaging, and treatment exposures are easy to review. That level of detail matters when the question is whether a finding looks benign, treatment-related, or concerning enough to pursue now.
Understanding Your Results and Planning Next Steps
For patients who have lived through cancer workups, a test result rarely feels routine. Even a normal report can stir up old fear. The goal after a well-woman exam is not just to wait for results. It is to know what each result means, what happens next, and how quickly follow-up should occur.
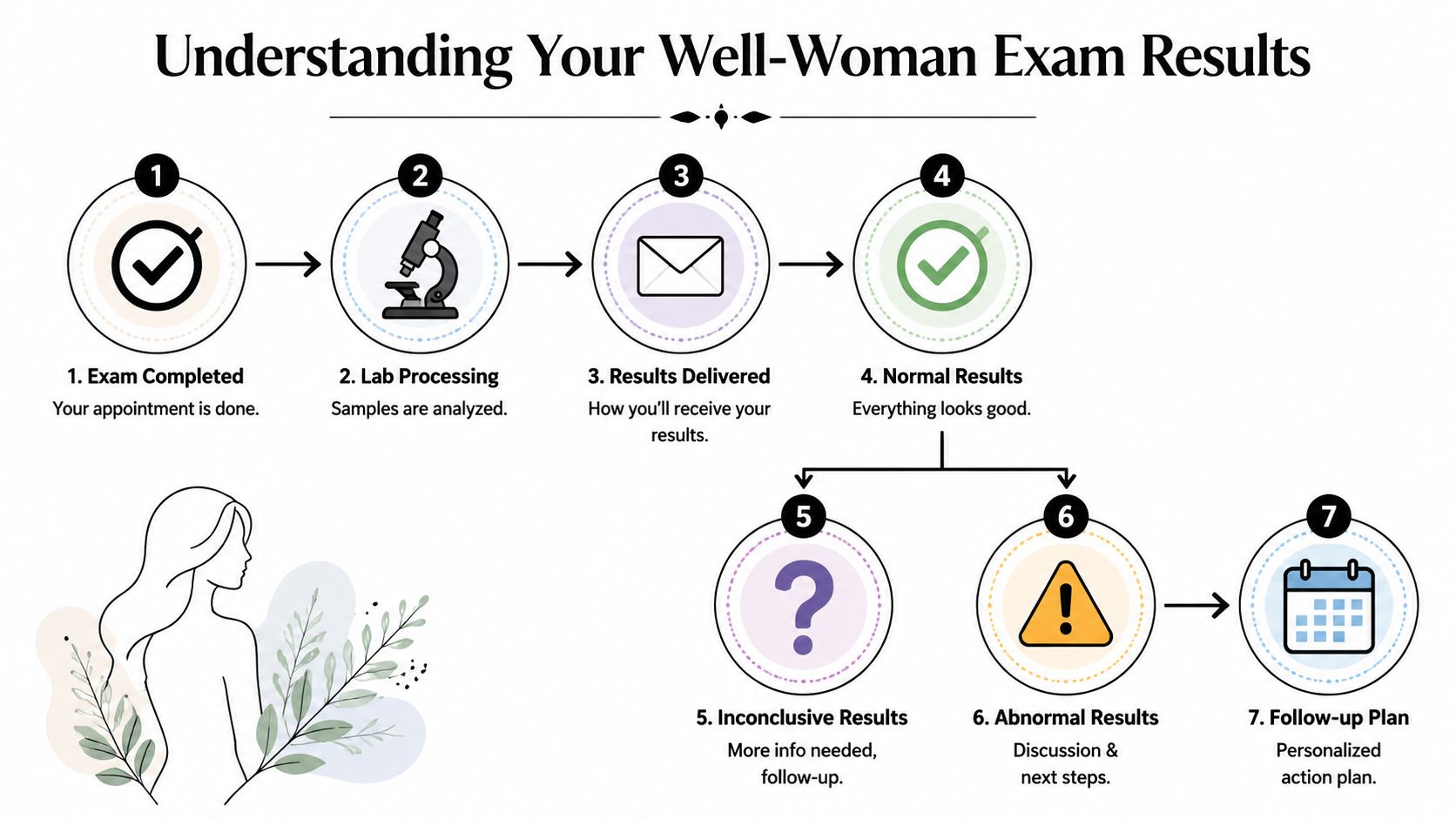
What normal, inconclusive, and abnormal usually mean
A normal result means that test did not show a concerning finding. It does not guarantee that future problems cannot develop, and it does not overrule new symptoms such as bleeding, breast changes, pelvic pressure, or persistent pain. In oncology, that distinction matters. Screening looks for silent problems. Symptom evaluation addresses what is happening now.
An inconclusive result usually means the sample or image did not answer the clinical question clearly enough. The next step is often a repeat Pap test, repeat HPV test, repeat imaging, or a closer examination. This is common medicine, not a sign that something serious was missed.
An abnormal result means more clarification is needed. Many abnormal cervical screening results reflect cell changes, inflammation, or HPV-related findings that are manageable and still far from invasive cancer. In breast care, an abnormal screening exam may lead to diagnostic mammography, ultrasound, or MRI based on the finding, breast density, prior imaging, and personal cancer history.
What a good follow-up plan should include
Patients do best when the plan is specific. Before you leave, you should know whether your results will arrive by phone, portal, or follow-up visit, how long that usually takes, and who is responsible for contacting you if something needs action.
Ask for the next step in plain language. Do you return in a year, repeat testing sooner, schedule colposcopy, get pelvic ultrasound, or see a breast or gynecologic specialist? Those details matter because delayed follow-up is one of the common ways a preventable problem becomes a more advanced one.
I also tell patients to ask one practical question: "What symptoms should make me call before the next scheduled visit?" For someone with a history of cancer, that answer may be as important as the result itself.
Keeping records organized makes follow-up faster and safer, especially if care is split between gynecology, primary care, breast imaging, and oncology. If your household is managing multiple appointments and reports, this guide can help you securely organize your family's medical info so biopsy dates, pathology findings, imaging reports, and treatment summaries are easy to review when decisions need to be made quickly.
Specialist referral is appropriate when findings move beyond routine prevention. Persistent cervical abnormalities, postmenopausal bleeding, a new pelvic mass, suspicious breast imaging, or symptoms that do not fit a benign pattern all deserve timely evaluation. Referral does not mean a worst-case diagnosis. It means the case now requires a narrower lens, better tools, or a clinician who handles that problem every day.
That distinction protects patients. In my field, the difference between "watch this" and "work this up now" can change stage at diagnosis, treatment intensity, and long-term quality of life.
Guidance for Cancer Patients and Survivors
Cancer patients often ask whether an annual well woman exam still matters once oncology care takes over. The answer is yes. It may look different, and the timing may need coordination, but it still matters.

During active treatment
Chemotherapy, endocrine therapy, targeted therapy, and pelvic treatments can change vaginal tissue, menstrual patterns, sexual function, and bone health. Patients may develop dryness, irritation, painful intercourse, unexpected bleeding, infections, or abrupt menopause symptoms. Those concerns are not side notes. They affect quality of life, adherence to treatment, intimacy, sleep, and mental health.
A well-woman visit gives those issues clinical attention. Sometimes the most important outcome of the appointment isn't a screening test. It's identifying a symptom that needs treatment, adjusting supportive care, or clarifying which changes are expected and which need investigation.
Practical examples include:
- Bleeding after treatment: this should never be brushed aside as “probably hormones” without assessment.
- Pelvic pain or pressure: may reflect benign causes, treatment effects, or a problem that deserves imaging.
- Severe dryness or pain with intimacy: often improves when a clinician addresses it directly instead of waiting for the patient to bring it up repeatedly.
In survivorship
Survivors often live with two competing instincts. One is vigilance. The other is exhaustion from appointments. The annual well woman exam helps make that vigilance efficient rather than constant.
For breast cancer survivors, it can support conversations about endocrine therapy side effects, menopause symptoms, sexual health, and new breast concerns. For gynecologic cancer survivors, it can help monitor symptoms that deserve prompt attention, including bleeding, pressure, pain, or changes in urinary and bowel function. For anyone treated with therapies that affect ovarian function or hormonal status, this visit can also help frame questions about long-term health and day-to-day function.
Some survivors skip this visit because they think oncology follow-up covers everything. It usually doesn't. Oncology visits and gynecologic preventive care answer different questions.
Caregivers should know this too. Many patients who are medically knowledgeable still postpone gynecologic care because it feels less urgent than cancer treatment. Yet survivors regularly tell clinicians that the “small” symptoms were the hardest to discuss and the easiest to delay.
The emotional side deserves room as well. An exam can reactivate fear, grief, body image distress, or memories of diagnosis and treatment. If loss and medical trauma are part of the picture in your family, outside support can help, including services such as Grande Prairie grief services for people looking for structured counseling support.
When to be especially proactive
Book the visit sooner rather than later if any of these apply:
- New bleeding: especially after menopause, after cancer treatment, or after a period of stability.
- Persistent pelvic symptoms: bloating, pain, pressure, or fullness that doesn't settle.
- Breast changes: skin dimpling, nipple inversion, discharge, or a new lump.
- Sexual health problems affecting daily life: pain, dryness, or recurrent irritation.
- A history of hereditary cancer concerns: especially if family history has changed or genetic questions were never fully addressed.
How to Prepare for Your Appointment
Preparation makes this visit better for both you and your clinician. A little organization helps the appointment move quickly toward your real concerns instead of spending most of the time reconstructing details.
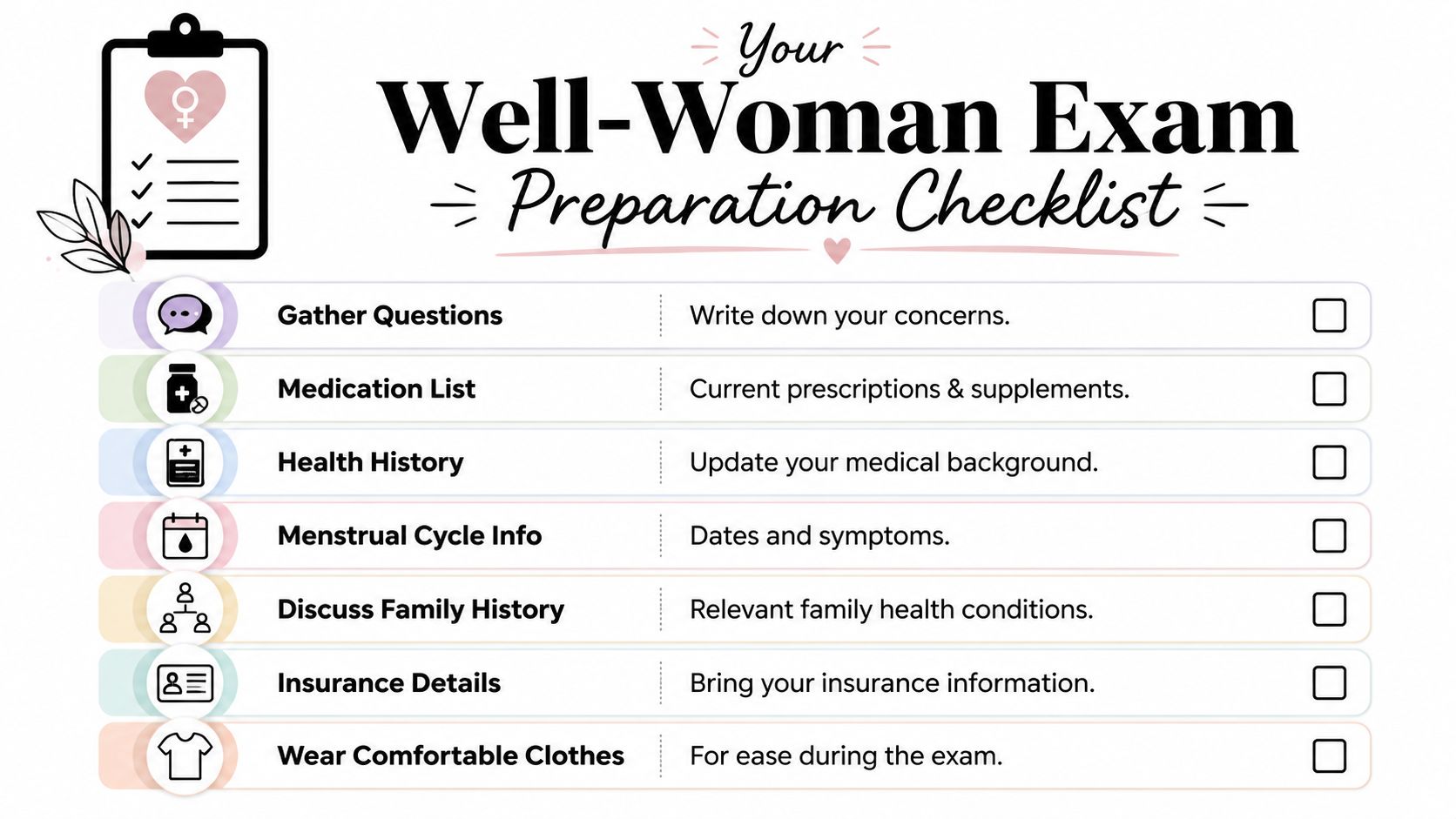
Bring the right information
You don't need a perfect binder, but you do need the basics.
- Medication list: include prescriptions, supplements, hormone therapies, and cancer-related medications.
- Symptom notes: write down what changed, when it started, and what makes it better or worse.
- Family history updates: especially breast, ovarian, colorectal, or other cancers in close relatives.
- Cycle information: if you menstruate, note timing changes, bleeding patterns, and pain.
- Prior reports if relevant: Pap results, imaging reports, surgery summaries, or treatment history.
Make the visit easier on yourself
If pelvic exams are painful, anxiety-provoking, or complicated by prior trauma, say so at the start. That single sentence changes how a thoughtful clinician approaches the visit. You can ask for slower pacing, explanation before each step, a smaller speculum, breaks, or postponing parts of the exam if needed.
This short video may also help reduce uncertainty before the appointment:
A practical checklist before you leave home:
- Write your top questions first: don't rely on memory once the visit starts.
- Wear comfortable clothes: changing in and out of exam attire is easier when you're not rushed.
- Bring insurance and ID: administrative delays add stress you don't need.
- Be direct about sensitive issues: clinicians can only address the symptoms they know about.
The best annual well woman exam is the one where you say the thing you almost decided not to mention.
Answers to Your Most Common Questions
Is the pelvic exam supposed to hurt
It shouldn't be ignored if it hurts. Some pressure can be normal, but sharp pain, severe discomfort, or panic are reasons to stop and regroup. Pain may reflect muscle tension, dryness, menopause-related tissue changes, past trauma, vulvar conditions, or other issues that deserve attention.
What if I have a history of sexual trauma
Tell the clinician before the exam begins, even if you keep it brief. You don't owe a full story. A trauma-informed clinician can explain each step, ask permission before touch, slow the pace, and help you stay in control of the visit.
Do I still need an annual well woman exam if I'm not sexually active
Yes. Sexual activity is only one part of gynecologic care. Breast symptoms, pelvic pain, abnormal bleeding, menopause concerns, and other health issues still matter.
What if I'm postmenopausal
You still need gynecologic attention, especially if you develop bleeding, pelvic pressure, pain, vulvar irritation, or urinary changes. Postmenopausal symptoms are common. They are not automatic reasons to avoid evaluation.
Do I need this visit if I'm in a same-sex relationship
Yes. Relationship status does not remove the need for breast and gynecologic care. Screening and symptom evaluation are based on your body, your history, and your risk profile.
What if I don't have insurance
Cost worries stop many patients from seeking care. The good news is that the annual well-woman exam is required as a preventive benefit under qualifying plans through the Affordable Care Act, as noted earlier. If you're uninsured, ask local clinics, community health centers, or hospital systems about low-cost women's health services and screening programs.
I'm already seeing multiple doctors for cancer care. Isn't that enough
Usually not. Oncology follow-up is focused on cancer treatment, surveillance, side effects, and disease-specific concerns. Gynecologic preventive care has its own purpose. Both matter, and one doesn't fully replace the other.
If you or a loved one is facing a complex cancer diagnosis and need thoughtful guidance on next steps, treatment options, or supportive care, Hirschfeld Oncology offers practical education and patient-centered oncology insight for people navigating difficult decisions.
.png)
.png)




