




.png)


Shortness of breath can change a whole day in minutes. A person with advanced cancer may be sitting in a favorite chair, talking normally, then suddenly feel as if the room has less air in it. Family members notice the pause between words, the shoulders rising with each breath, the worry that shows up before anyone says it out loud.
That moment is frightening, but it helps to know this. At home oxygen can be a practical tool, not a symbol of giving up. For many people, it becomes one part of a plan that helps them rest more comfortably, move around the apartment with less fear, and save energy for the things that matter most.
I often explain it to families this way. Oxygen isn't there to define the illness. It's there to support the person living with it. Sometimes that means making it easier to get from the bedroom to the bathroom. Sometimes it means being comfortable enough to sit at the table for dinner. Sometimes it means less panic.
Breathing also gets easier to understand when you picture what happens deep in the lungs. If you want a simple visual explanation of how oxygen moves into the blood, this guide to understanding alveoli is a helpful place to start. Those tiny air sacs matter a lot when cancer, treatment, fluid, infection, or weakness interferes with normal breathing.
Regaining Your Breath and Your Life
Maria, a fictional example based on a very familiar situation, had metastatic cancer and lived in a Brooklyn walk-up with her daughter. She wasn't afraid of the infusion chair. She was afraid of the trip from the sofa to the bathroom. The shortness of breath made her feel trapped, and her daughter worried every time she heard the oxygen monitor beep.
What changed first wasn't the disease itself. It was the family's sense of control. Once they understood what oxygen was for, how to use it, and what kind of equipment fit their apartment and routine, the fear dropped. The day still had limits, but it became manageable again.
That's the primary purpose of at home oxygen in cancer care. It's not about turning your home into a hospital. It's about helping daily life feel more livable.
Oxygen at home often works best when families stop seeing it as a crisis device and start seeing it as a support tool for ordinary moments.
Many people hesitate because oxygen feels like a big step. They worry it means the cancer is suddenly worse, or that life will shrink to one room. In practice, the opposite can happen. When breathing is supported appropriately, some people can speak more comfortably, move with less distress, and use their energy more wisely.
Families also get overwhelmed by the practical questions. Where will the machine go in a small apartment? What happens if the power goes out? Who teaches you what the buttons mean? Can someone still go to appointments, family events, or the park?
Those are the right questions. The answers are usually more straightforward than people expect once they're explained clearly.
Understanding Home Oxygen for Cancer Care
Shortness of breath and low oxygen aren't the same thing. That's one of the biggest points of confusion for patients and caregivers.
A person can feel very breathless and still not need oxygen. Another person may not feel dramatic distress but still have blood oxygen levels low enough that oxygen is medically important. At home oxygen treats hypoxemia, which means low blood oxygen. It isn't a general fix for every kind of breathlessness.
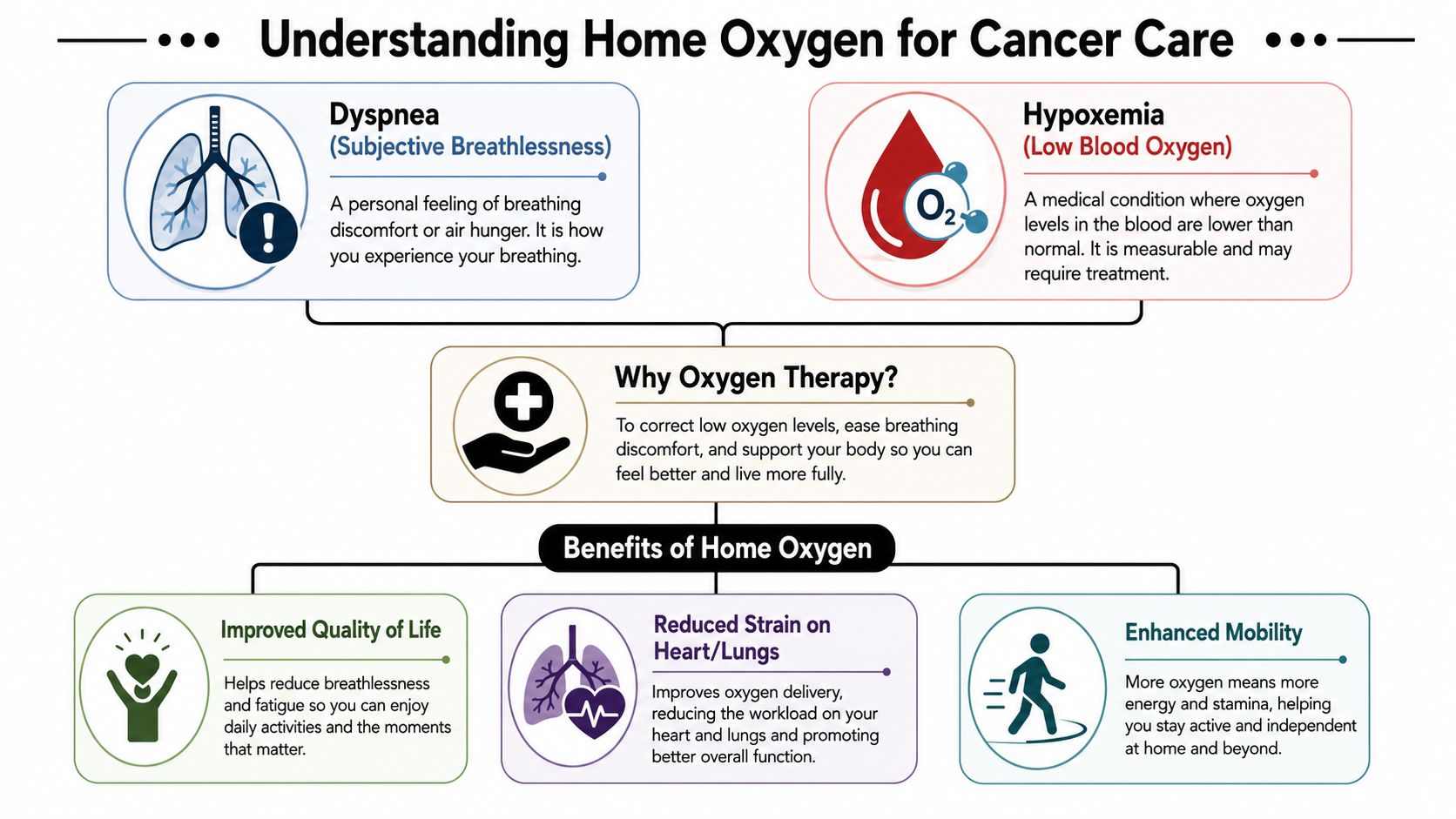
Breathlessness versus low oxygen
I often compare it to a fuel gauge and engine strain. Dyspnea is the feeling that breathing is hard. Hypoxemia is the measured problem showing there isn't enough oxygen in the blood. Oxygen therapy is prescribed based on the measured problem, not just the feeling.
Cancer can affect breathing in several ways. A tumor can reduce lung function. Fluid around the lungs can make expansion harder. Infection, weakness, anemia, prior lung disease, or treatment effects can add to the burden. Some of those causes improve with oxygen. Others need different treatment, such as drainage, medication adjustment, transfusion evaluation, or symptom management. If chemotherapy has affected red blood cells, this overview of anemia from chemo can help explain why breathing may feel harder even when the cause isn't only the lungs.
Clinical point: Oxygen is prescribed for documented low blood oxygen, not simply because breathing feels uncomfortable.
The common qualification thresholds described in StatPearls guidance on home oxygen therapy include SpO2 of 88% or less or PaO2 of 55 mm Hg or less. That same source notes clinicians often target SpO2 90–92% to balance benefit with risk, especially because oxygen given too aggressively can create problems in some patients.
Why the prescription is specific
Families sometimes ask why the oxygen flow rate can't just be turned up until the number looks as high as possible. The answer is simple. More oxygen isn't automatically better. The same clinical guidance notes that prolonged oxygen concentrations above about 50% oxygen can contribute to atelectasis and oxidative stress, and in COPD can worsen hypercapnia. That's why titration matters.
This is also why your team may test oxygen needs in different situations:
- At rest when you're sitting
- With activity such as walking to the bathroom or kitchen
- During sleep if nighttime levels are a concern
That individualized approach matters in cancer care, especially when symptoms change from day to day.
The caregiving side of oxygen decisions
For many families, oxygen becomes part of a broader home support conversation. If you're also thinking through mobility help, supervision, or daily assistance, this guide on exploring elderly care options may be useful for framing what kind of help makes life easier at home.
A helpful mindset is this. Oxygen can be one answer, but it usually isn't the whole answer. In advanced cancer care, the best plan often combines oxygen with medications, pacing, positioning, caregiver support, and treatment of the actual cause whenever possible.
Types of At Home Oxygen Systems
Most families start with the same question. "What exactly are we getting?" The answer depends on how much oxygen is needed, how often it's needed, and what daily life looks like in the home.
The biggest tradeoff is convenience versus power dependency. According to Inogen's overview of home oxygen concentrators, a stationary concentrator draws in room air, removes nitrogen and other gases, and delivers concentrated oxygen. It's often preferred for continuous home use because it avoids tank refills, but it depends on electricity. Portable systems improve mobility, but they require supply planning and refills.
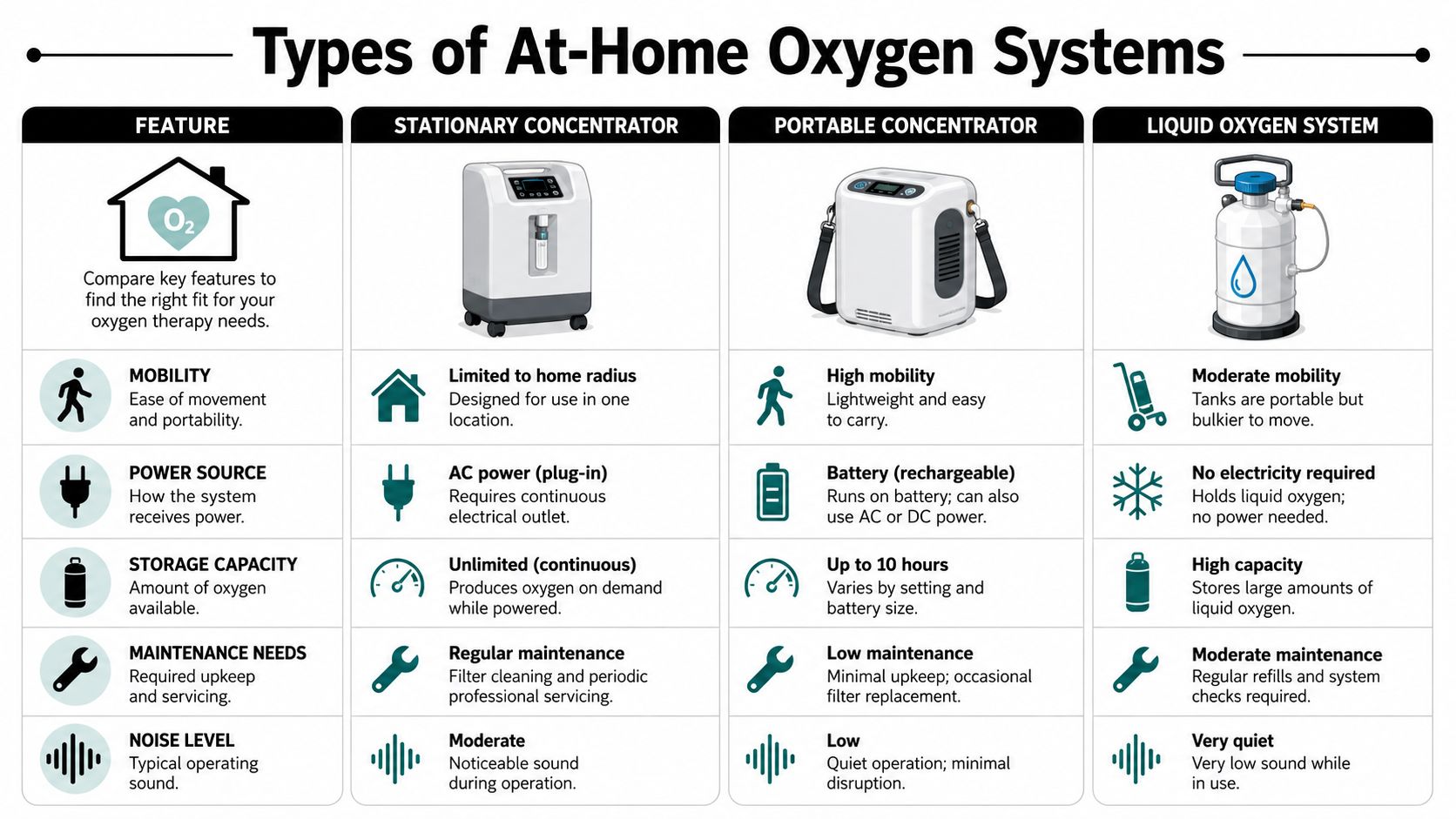
The three main setup styles
A stationary oxygen concentrator usually lives in one main room or bedroom area. It pulls in ambient air and provides concentrated oxygen through tubing to a nasal cannula or mask. This setup is often the easiest for long stretches at home because there are no routine tank swaps.
A compressed gas cylinder stores oxygen in a tank. Some tanks are smaller and easier to carry. Others are larger and stay in the home as backup or primary supply. The advantage is independence from wall power. The tradeoff is that someone has to monitor how much oxygen remains and arrange replacements.
A liquid oxygen system stores oxygen in liquid form and can support portable use. Families often hear about it when mobility is a high priority. The practical issue is logistics. It requires supply management, and people need training on handling and refilling portable units if that system is offered.
Comparing home oxygen delivery systems
| System Type | How It Works | Best For | Key Limitation |
|---|---|---|---|
| Stationary concentrator | Pulls in room air, removes nitrogen, delivers concentrated oxygen through tubing | People who need regular oxygen at home for long periods | Needs uninterrupted electricity |
| Compressed gas tank | Stores oxygen in a cylinder that flows through a regulator | Backup supply, shorter trips, situations where power loss is a concern | Needs replacement and careful supply tracking |
| Liquid oxygen system | Stores oxygen in liquid form for home and portable use | People who need more mobility and a portable option | Requires refill planning and handling support |
| Portable oxygen concentrator | Uses battery or external power to provide oxygen in a smaller device | Appointments, errands, and travel | Battery management and suitability depend on the prescribed setup |
How families choose in real life
In a small New York apartment, the "best" system isn't just about medicine. It's also about layout, outlets, elevator access, caregiver availability, and whether the patient leaves home often for treatment.
A concentrator often works well if someone spends most of the day at home and wants less hassle with deliveries. A tank setup may feel safer to some families because they like having stored oxygen that doesn't stop with a power loss. A portable concentrator may be useful for repeated clinic visits, but it still requires battery planning and confirmation that it meets the prescription.
A good oxygen setup fits the patient's medical needs and the household's routine. Both matter.
Questions worth asking before delivery
Before equipment arrives, ask the DME company or prescribing team:
- What system is being ordered: Is it a stationary concentrator, tanks, a portable concentrator, or a combination?
- What is the backup plan: If the main device stops working, what should the family use right away?
- What training is included: Who will show the patient and caregiver how to turn it on, check alarms, and replace tubing?
- How is resupply handled: If tanks are part of the plan, how do you request more and how quickly can they arrive?
- What works for appointments: If the patient goes to infusion or scans often, what portable setup matches that schedule?
The right equipment can make home oxygen feel manageable. The wrong fit creates stress every day.
Arranging Home Oxygen in New York City
In New York City, setting up oxygen is partly a medical process and partly a logistics process. Families often expect the hardest part to be the prescription. In reality, the hardest part is usually coordinating the details in a way that fits a city apartment, a treatment schedule, and a caregiver's bandwidth.

Step one is the clinical order
The process starts when the treating clinician documents the need for oxygen and writes the prescription. Coverage decisions are tied to documented hypoxemia. Medicare's national coverage policy explains that home oxygen is covered for qualifying acute or chronic conditions when there is evidence such as oxygen saturation at or below the qualifying threshold at rest, and the prescription should match needs at rest, during activity, and during sleep as outlined in the CMS home oxygen coverage determination.
For patients and families, that means the order usually isn't a generic note saying "use oxygen as needed." It needs to be specific enough for the DME company and insurer to act on.
What paperwork usually matters
The names of forms can vary by payer and vendor, but families commonly hear about a certificate of medical necessity, testing results, visit notes, and a signed prescription. The oncology office or hospital team usually gathers and sends the required records.
In city practice, speed matters. A delay of even a day can feel long when someone is breathless. Ask one practical question early: "Who is sending the paperwork, and who will confirm that the equipment company received it?" That one question prevents a lot of repeated phone calls.
A few details help in NYC specifically:
- Apartment access: Tell the supplier if the building has stairs only, a narrow elevator, a doorman, or restricted delivery hours.
- Building communication: Some buildings require advance notice for medical deliveries.
- Caregiver timing: Make sure the person who'll learn the equipment can be present during setup.
- Clinic routine: If infusion visits, scans, or radiation appointments are frequent, mention that before the portable setup is chosen.
Choosing and preparing for a DME delivery
The DME company supplies the equipment, teaches basic use, and handles maintenance or replacement. In practice, a responsive DME provider matters as much as the device itself. Families in the city benefit from asking direct questions about delivery windows, emergency response, after-hours support, and how backup supplies are handled.
What helps most: Ask the supplier to explain the setup as if you're the person who'll be using it alone at 2 a.m.
Once the equipment arrives, expect hands-on teaching. The technician should show how to turn the device on and off, where to connect the tubing, what alarms mean, and what to do if the machine stops. If a portable tank is included, ask for a live demonstration, not just a verbal explanation.
For families also weighing comfort-focused support at home, this article on palliative care vs hospice care can help clarify where oxygen fits within a broader care plan.
A visual walkthrough can also make the process less abstract:
A simple NYC checklist
- Confirm the order: Make sure the prescription reflects how oxygen is needed in daily life.
- Verify the destination details: Apartment number, call box, floor, elevator, and delivery restrictions all matter.
- Prepare the space: Choose an outlet, clear a path for tubing, and decide where backup supplies will stay.
- Have one point person: One family member should track the DME company's name, phone number, and delivery instructions.
- Ask for repeat teaching: If the setup isn't clear, ask the technician to show it again before leaving.
In New York, oxygen setup works best when the home, the clinic, and the supplier communicate clearly. That coordination lowers stress for everyone.
Daily Management and Safety at Home
The first few days with oxygen often feel awkward. Tubing gets caught on chair legs. The cannula may feel dry. Alarms can startle people even when nothing dangerous is happening. That learning curve is normal.
What matters most is building a calm routine. Families do better when they know what to check every day, what problems need a call, and what to do immediately if the power fails.
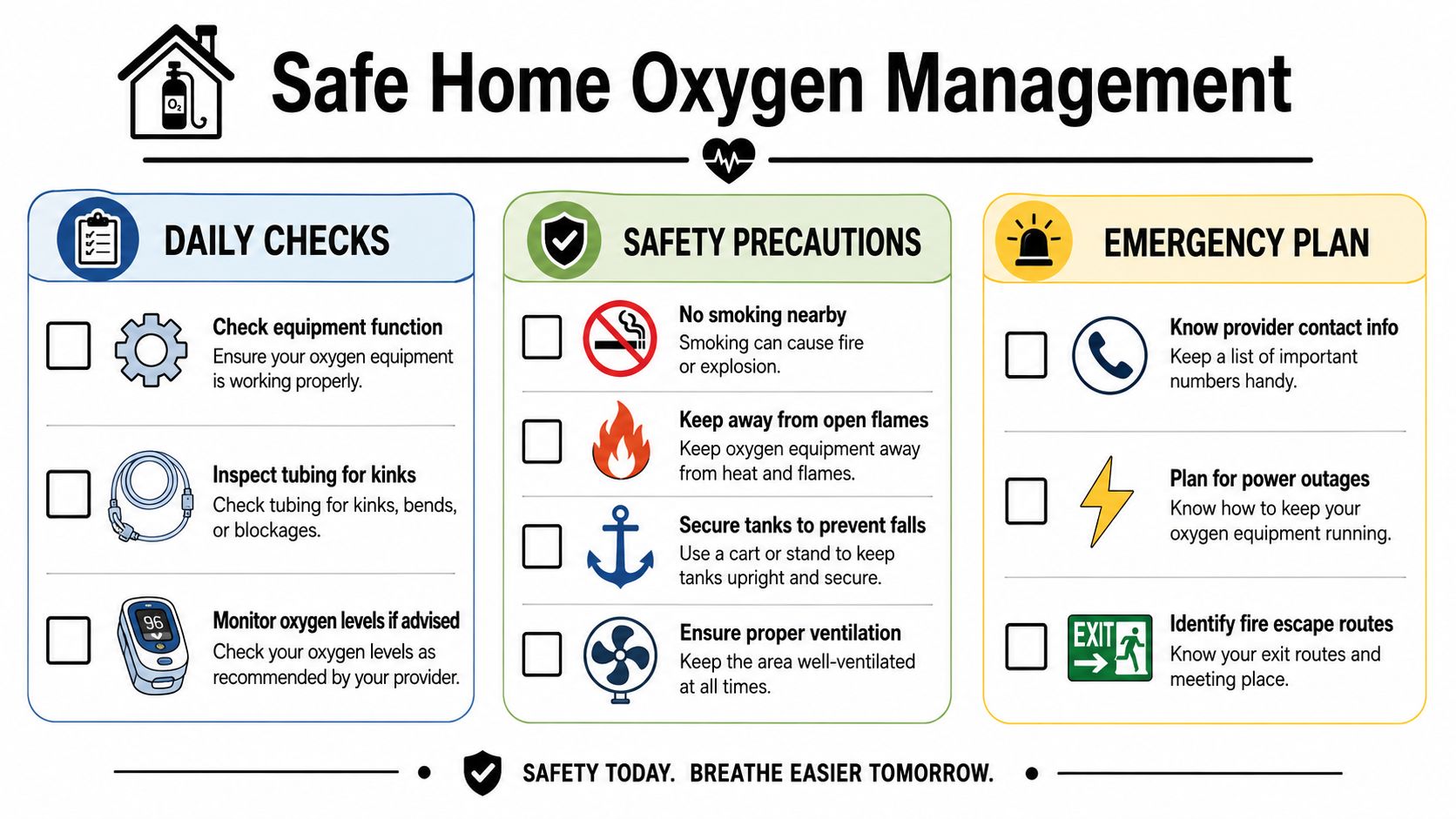
Daily habits that prevent bigger problems
Start with the simple checks. Is the machine on? Is the tubing connected firmly? Is the cannula sitting correctly in the nose? Is the tubing kinked under a footstool, bedrail, or recliner wheel?
A short daily routine often helps:
- Check the path of the tubing: Follow it with your eyes from the machine to the patient.
- Listen for changes: New sounds from the concentrator or regulator deserve attention.
- Keep supplies together: Cannulas, backup tubing, and contact numbers should stay in one known place.
- Watch for skin irritation: Ears, cheeks, and the nostril area can get sore from friction or dryness.
If the home environment also affects breathing comfort, some families ask about cleaner indoor air. While an air purifier doesn't replace oxygen, this guide to best air purifiers for asthma may help with general air-quality questions that come up in shared apartments or city homes.
Safety rules that need to be nonnegotiable
Oxygen itself isn't a flame, but it supports combustion. That means fire safety has to be taken seriously.
Keep oxygen away from smoking, candles, gas flames, and anything that can spark. Tanks should be stored securely so they don't tip. Concentrators need space around them for airflow and shouldn't be wedged tightly against curtains or furniture.
Keep oxygen equipment in a place where it can breathe too.
Families also need a clear outage plan. Temple Health advises that stationary concentrators fail during power outages and that patients should immediately switch to a portable oxygen tank until electricity is restored, as described in its guidance on living with oxygen at home. That backup supply isn't optional. It's a core safety part of the setup.
What to do if something goes wrong
If the concentrator alarm sounds, first check the basics. Look for a disconnected plug, a kink in the tubing, or an accidental power switch change. If power is out, move to the backup tank right away.
If a tank seems empty or the regulator isn't working, use the alternate supply if one is available and call the DME company. If the patient becomes much more short of breath, confused, or distressed while equipment problems are happening, treat that as a medical urgency, not just a device problem.
A written plan on the refrigerator or near the main phone helps. Include the DME number, the oncology number, and simple instructions for switching to backup oxygen.
Staying Mobile and Traveling with Oxygen
Many patients hear "oxygen at home" and think it means staying home. That isn't how it has to work.
I've seen people use portable oxygen to keep doing very ordinary, very meaningful things. One patient used it to make the trip from Bushwick to an infusion appointment without arriving exhausted. Another used it for a Sunday visit with family in Queens. Another wanted enough confidence to sit on a park bench for a little while after a clinic visit.
Mobility starts with planning, not bravery
Leaving the apartment gets easier when the outing is broken into steps. What device is going with you? Who is carrying it? How long will the trip take from door to destination and back again? Where can you sit and rest if needed?
For appointments, think through the whole route, not just the visit itself. In New York, that includes stairs, sidewalks, elevators, rideshare wait time, building lobbies, and time spent checking in. Families often do best when they pack oxygen like they pack medications. Deliberately, and earlier than they think they need to.
A few practical habits help:
- Prepare the night before: Put the device, charger or tank key if needed, and appointment paperwork in one place.
- Bring more support than you think you'll need: Extra tubing, the power cord, and a backup plan matter.
- Know your walking breaks: It's easier to pause early than to push through distress.
- Tell the clinic if oxygen is in use: Staff can often help with seating and pacing once you arrive.
If getting to treatment is the hardest part of the day, this resource on transportation assistance for cancer patients may help you organize the trip itself.
Travel is possible, but details matter
Longer travel takes more coordination. Portable oxygen concentrators need charged batteries and a charging plan. Tank-based travel requires knowing exactly how oxygen will be available along the route and at the destination.
For any substantial trip, speak with the prescribing team and equipment provider ahead of time. If air travel is involved, confirm the device requirements directly with the airline and make sure the oxygen plan covers the airport, the flight, ground transportation, and the place you're staying. The same principle applies to overnight car trips or visits out of town. Oxygen has to be available at every step, not just after arrival.
The trip usually goes better when the oxygen plan is written down, not held in someone's memory.
Freedom often looks smaller, and that's okay
Mobility doesn't have to mean big travel. Sometimes success is attending a grandchild's school event, going downstairs for fresh air, or making it through a scan day with less fear. Portable oxygen can support those goals when it's chosen and prepared well.
That's an important emotional shift. The device may look like a limitation at first. For many families, it becomes the reason the person can keep showing up for life outside the apartment.
Partnering With Your Oncology Team
At home oxygen works best when everyone knows their role. Patients often get stuck between two kinds of problems. One is a medical change. The other is an equipment problem. They can happen on the same day, which is why clear communication matters.
If the machine won't turn on, the tubing connector breaks, the backup tank is missing, or an alarm won't stop despite basic troubleshooting, call the DME company. Those are equipment and supply issues. The oncology office can't replace a malfunctioning concentrator from across town.
If breathing has changed, call the oncology team. New shortness of breath, more coughing, chest discomfort, increasing fatigue, trouble speaking in full sentences, new swelling, or a noticeable drop in function may reflect the cancer, fluid, infection, anemia, treatment effects, or another medical issue. Oxygen may be part of the response, but it may not be the whole answer.
When to call right away
Some symptoms deserve same-day medical attention, even if oxygen equipment seems to be working:
- Sudden worsening of breathing: Especially if it feels different from the person's usual pattern
- Chest pain or pressure: This needs urgent evaluation
- Confusion or unusual sleepiness: Changes in thinking or alertness matter
- Blue or gray lips, face, or nail beds: This can signal significant oxygenation trouble
- Severe distress despite prescribed oxygen: The equipment may be functioning, but the body still needs urgent assessment
If the person appears acutely ill or unsafe, seek emergency care.
Oxygen is one tool in a bigger plan
Cancer-related shortness of breath often needs layered care. Oxygen can support low blood oxygen. Positioning can reduce the work of breathing. Medications may ease air hunger or treat infection, fluid, inflammation, or anxiety. Treatment decisions may also shift if symptoms are changing.
That broader view matters because families sometimes feel they've "failed" if oxygen alone doesn't solve everything. They haven't. It shows that breathlessness in cancer care is often complex, and the right response may involve several interventions at once.
Good cancer care doesn't separate symptoms from treatment. It treats both together.
Keeping communication simple
One page of notes can prevent a lot of confusion. Write down the oxygen prescription, the DME company name and phone number, what equipment is in the home, and the symptoms that are new versus usual. Bring that information to appointments.
It also helps to tell the oncology team what daily life looks like. Saying "She gets breathless walking from the bed to the kitchen" is more useful than saying "She's a little worse." Concrete examples lead to better decisions.
Families don't need to master everything at once. They need a working plan, a backup plan, and a clear sense of who to call when something changes. That's enough to start.
If you or a loved one is dealing with advanced cancer, breathing changes, and the practical realities of care in New York City, Hirschfeld Oncology offers guidance grounded in complex cancer treatment, symptom management, and patient-centered support. You can explore their blog for more help with treatment decisions, daily care questions, and next-step planning.
.png)
.png)




