




.png)


A 2023 meta-analysis found that 43% of people with cancer report clinically meaningful fatigue, and when milder forms are included, the number rises above 70%. During active treatment, severe fatigue was reported in 33.8% of patients in that same analysis. Those numbers matter because they reframe fatigue for what it is. Not weakness, not poor motivation, and not a failure to “push through.”
For many women with breast cancer, fatigue doesn't look dramatic from the outside. It looks like standing in the kitchen and forgetting why you walked in. It looks like needing to sit down halfway through folding laundry. It looks like answering one email, taking a shower, making a phone call, and feeling as if the day is already spent.
Patients often tell me they worried they were “doing cancer badly” because they couldn't bounce back with a nap or a good night's sleep. That's a painful misunderstanding. If you've also been exploring root causes of tiredness in a broader sense, it helps to know that breast cancer fatigue is its own medical problem with its own patterns, triggers, and treatment approach.
The Unseen Struggle of Breast Cancer Fatigue
Breast cancer and fatigue are tightly linked, but fatigue still gets minimized in everyday care. Family members may see you resting and assume rest should fix it. Employers may hear “tired” and think of a normal bad night of sleep. Even patients sometimes underreport it because they don't want to sound ungrateful, discouraged, or dramatic.
That silence creates its own burden. When fatigue isn't named clearly, people start blaming themselves for symptoms that are completely consistent with cancer and its treatment.
Why this symptom feels so isolating
Breast cancer fatigue is often invisible. Nausea shows. Hair loss shows. A surgical scar shows. Fatigue usually doesn't.
So patients try to keep performing. They show up to treatment. They answer texts. They make dinner when they can. On the outside, they may look functional. On the inside, they may feel as though someone turned the dimmer switch down on every physical and mental task.
Fatigue can be one of the most disruptive symptoms in oncology precisely because it affects everything at once. Strength, concentration, mood, sleep, work, and relationships.
What patients most need to hear early
A few points make an immediate difference:
- This is common: You are not unusual if fatigue becomes one of the hardest parts of treatment.
- This is medical: It may reflect inflammation, treatment effects, anemia, poor sleep, pain, mood symptoms, or several factors at the same time.
- This is actionable: “Get more rest” is rarely enough. Good fatigue care usually requires a plan.
That plan starts with understanding what cancer-related fatigue is, and just as important, what it is not.
What Cancer-Related Fatigue Really Means
A useful way to think about cancer-related fatigue, or CRF, is this: your body is acting like a phone battery that no longer holds a full charge. You can plug it in overnight, but it still drains faster than expected. Small tasks use more power. Recovery is incomplete. Some days the battery drops for no obvious reason.
That's different from ordinary tiredness. Normal tiredness is proportional. If you've had a busy day, you feel worn out, you sleep, and your energy usually improves. CRF doesn't follow that clean pattern.

How CRF differs from being tired
Cancer-related fatigue is usually:
- Out of proportion to activity: You may feel depleted after something minor, like getting dressed or making breakfast.
- Not fully relieved by rest: A nap may help a little, but it often doesn't reset you.
- Persistent: It can last through treatment, between cycles, and sometimes long into survivorship.
- Function-limiting: It changes what you can realistically do in a day.
Ordinary tiredness is usually more predictable and easier to reverse.
It's physical, mental, and emotional
CRF isn't only about heavy limbs or low stamina. Many patients also describe a slowed mind. They lose words mid-sentence, struggle to focus on reading, or feel overwhelmed by decisions they'd normally make easily.
There's also an emotional layer. When your body is depleted for weeks or months, frustration builds. Some patients feel guilty. Others feel disconnected from their old selves. That emotional distress doesn't mean the fatigue is “just stress.” It means fatigue affects the whole person.
Practical rule: If your energy loss is interfering with work, household tasks, concentration, or your ability to enjoy a normal conversation, it deserves the same clinical attention as pain or nausea.
The language that helps in appointments
Patients often get better care when they describe fatigue specifically rather than saying “I'm just tired.” More useful phrases include:
- “Rest doesn't bring me back to baseline.”
- “I can do one activity, then I crash.”
- “My body feels weak, and my thinking feels slower.”
- “I'm sleeping, but I'm not restored.”
That kind of description helps your oncology team separate CRF from simple sleep deprivation, depression alone, medication sedation, or another medical issue that needs its own workup.
The Many Causes of Fatigue During Breast Cancer
Fatigue during breast cancer is rarely caused by a single thing. In clinic, the most helpful approach is to sort it into layers. What is the cancer itself doing? What are treatments doing? What other issues are piling on top?
That framework matters because different causes respond to different solutions.
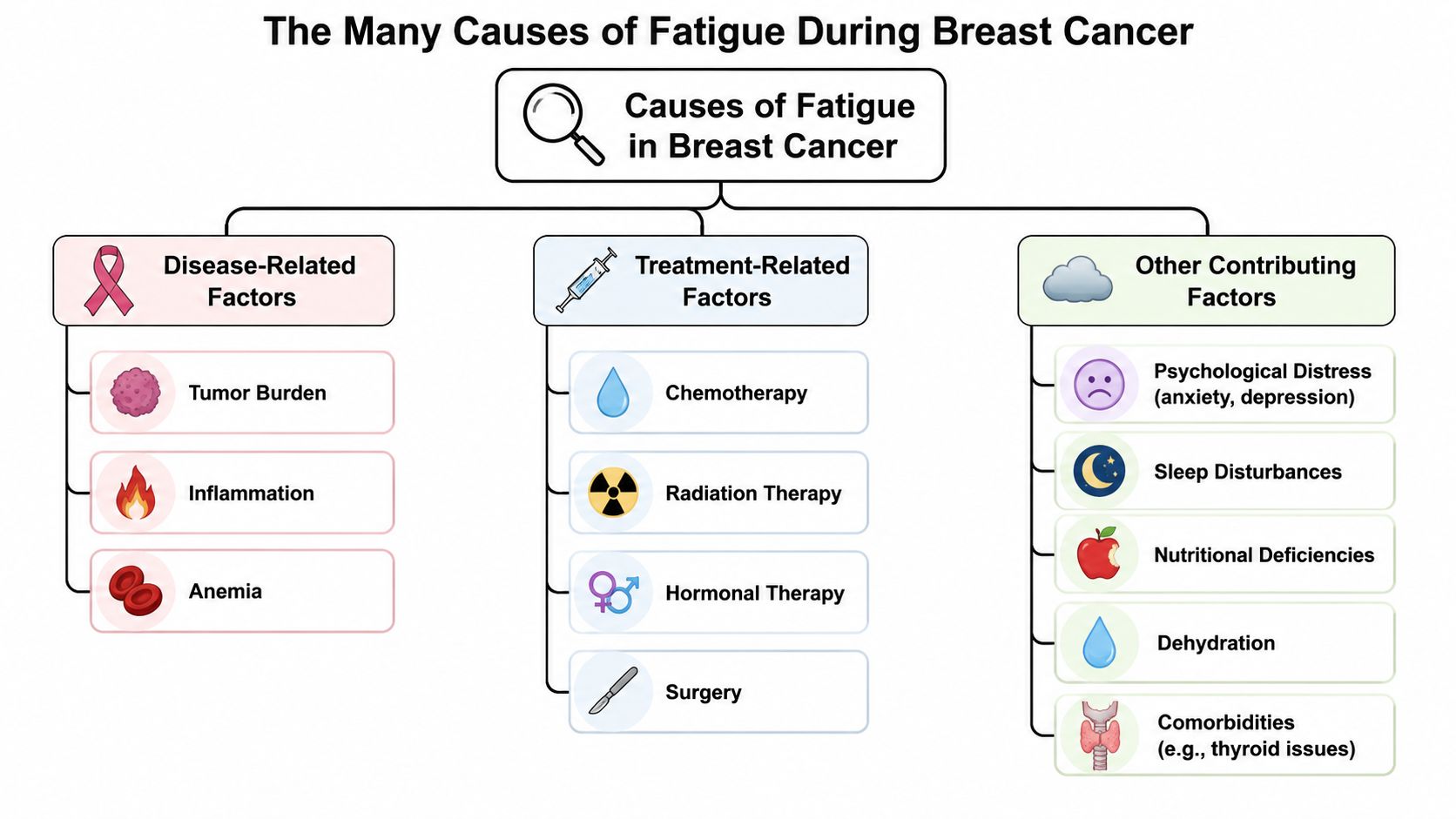
Disease-related causes
The cancer itself can drain energy before treatment even starts. Tumors change metabolism, trigger inflammatory signaling, and can increase the body's baseline energy demands. In more advanced disease, fatigue may also reflect pain, appetite loss, weight loss, or the effort the body is making to adapt to a larger disease burden.
Some patients feel frustrated when fatigue starts “too early,” as if it shouldn't count until chemotherapy begins. It counts. Early fatigue is real.
Treatment-related causes
Treatment often adds another layer:
- Chemotherapy: This can lower blood counts, increase inflammation, disrupt appetite, and create a pattern of post-treatment crashes.
- Radiation: Energy often fades gradually over a course of treatment rather than all at once.
- Hormonal therapy: Some patients develop a slower, more chronic fatigue pattern, often tied to sleep disruption and mood changes.
- Surgery: Recovery, pain, anesthesia effects, and reduced mobility all contribute.
- Immunotherapy and targeted therapy: These can be effective and sometimes more tolerable, but they can still produce meaningful fatigue, especially when side effects affect sleep, appetite, or daily rhythm.
There's an important trade-off here. A treatment that's better tolerated in one patient may not be better tolerated in another. Less aggressive doesn't automatically mean energizing. More aggressive doesn't always mean unbearable. The right question is not “Which treatment causes no fatigue?” It's “Which treatment gives the best cancer control with the most manageable symptom burden for this person?”
The stage-specific uncertainty patients often feel
There is limited data-driven guidance on how fatigue trajectories differ by stage. That leaves many patients with advanced disease unsure whether a less aggressive approach, such as lower-dose chemotherapy plus immunotherapy, will meaningfully reduce fatigue compared with conventional treatment, even though emerging evidence suggests treatment pacing and supportive care timing can influence the experience.
That uncertainty is real in practice. It's one reason fatigue management has to be individualized rather than copied from a generic handout.
Other contributors that deserve attention
Very often, the “extra” causes are the ones we can improve most directly.
- Anemia: Low red blood cells can make even short walks exhausting. If you're dealing with treatment-related blood count changes, this guide on anemia from chemotherapy can help you understand the basics before discussing next steps with your doctor.
- Sleep disruption: Pain, hot flashes, steroids, anxiety, and bathroom trips can fragment sleep badly. Poor sleep also affects balance and confidence with movement. For patients who feel unsteady, this piece on understanding sleep-related fall hazards adds useful context.
- Mood symptoms: Anxiety and depression can amplify fatigue and make recovery feel impossible.
- Nutrition and hydration: Not eating enough or drinking enough leaves the body without fuel.
- Other medical issues: Thyroid disease, infection, medication side effects, and uncontrolled pain can all present as “fatigue.”
When patients understand that fatigue has components, they often feel less trapped. The symptom is still hard, but it stops feeling mysterious.
How Your Doctor Assesses and Tracks Fatigue
The most important rule in fatigue assessment is simple. If you don't report it clearly, your team may underestimate it.
That happens more often than patients realize. Some people mention fatigue in passing at the end of a visit. Others normalize it because they assume nothing can be done. But breast cancer and fatigue should be followed as deliberately as blood pressure, pain, or nausea.
What assessment usually looks like
Most oncology teams start with direct questions. How severe is the fatigue? When does it happen? Is it constant or cyclical? What tasks can you no longer do easily? Does rest help at all?
You may also be asked to rate it on a 0 to 10 scale, keep a daily symptom log, or complete a questionnaire about function, sleep, mood, and energy. Those tools aren't paperwork for the sake of paperwork. They help distinguish patterns.
For example, fatigue that peaks right after infusion may need a different strategy than fatigue that stays flat all month. Fatigue with dizziness points us one way. Fatigue with insomnia and racing thoughts points us another way.
Why tracking matters over time
Fatigue is not static. In prospective research, about 21% of breast cancer patients fell into a high-risk group with severe fatigue from diagnosis through year 4 post-treatment according to this report on persistent fatigue trajectories. That finding matters because it supports early identification rather than waiting for fatigue to become entrenched.
In practical terms, I want patients to tell us:
- What changed: “I used to walk the block. Now I can't get to the corner.”
- When it changed: “This got worse after my second cycle.”
- What comes with it: shortness of breath, low mood, poor sleep, palpitations, weakness, pain, or loss of appetite.
- How it affects safety: trouble driving, climbing stairs, showering alone, or carrying groceries.
If fatigue is changing your daily function, it also often changes your performance status, which is one of the key tools oncologists use when weighing treatment tolerance and next-step decisions.
The best fatigue assessment is not “Are you tired?” It's “What can you no longer do the way you could last month?”
Red flags that should prompt a call
Some fatigue can wait for the next scheduled visit. Some shouldn't.
Call your team promptly if fatigue is paired with:
- New shortness of breath
- Chest discomfort
- Fainting or near-fainting
- Confusion
- Rapid worsening over days
- Severe weakness that makes walking unsafe
- Dark thoughts, hopelessness, or loss of interest that feels unmanageable
Those symptoms may point to anemia, infection, medication toxicity, uncontrolled depression, dehydration, cardiac issues, or another problem that needs immediate attention.
Evidence-Based Strategies to Manage Fatigue
The best fatigue plans are multimodal. A single fix usually doesn't exist. What works is matching the intervention to the driver, then layering support where needed.
What doesn't work well is vague advice. “Try to rest more” helps almost no one by itself. Rest matters, but too much rest can also lead to deconditioning, worse sleep at night, and a smaller functional world.
Start with the treatable medical drivers
If fatigue is being powered by a correctable medical issue, that issue has to be addressed directly.
Examples include:
- Anemia management: If blood counts are low, your oncologist will evaluate the cause and decide whether treatment changes or supportive measures are appropriate.
- Pain control: Poorly controlled pain exhausts patients. Better pain management often improves sleep and restores activity.
- Medication review: Sedating medicines can worsen daytime exhaustion.
- Sleep-disrupting side effects: Night sweats, reflux, nausea, steroids, and urinary symptoms all deserve active treatment.
This is why fatigue care belongs in oncology visits. It's not a side conversation. It's part of treatment tolerance.
Exercise is often the highest-yield intervention
This surprises many patients. When you already feel depleted, movement sounds backwards. But structured, scaled activity is one of the most reliable ways to reduce fatigue over time.
The key is dose and timing. The goal is not to “work out harder.” The goal is to avoid the crash cycle of overdoing it on one day and losing the next two.
For many patients, that means:
- Short walks instead of ambitious workouts
- Light resistance work instead of all-cardio
- Consistency instead of intensity
- Adjustments on infusion weeks or rough days
For people receiving immunotherapy or targeted therapy, exercise still matters, but it has to be coordinated with symptom patterns. Joint pain, muscle aches, neuropathy, or immune-related side effects may call for a slower build and closer communication with the care team.
ACT and psycho-oncology are not “optional extras”
In long-term survivors, fatigue is more strongly linked to psychological symptoms such as depression and anxiety than to cardiovascular issues from treatment, according to this survivor fatigue study. That doesn't mean fatigue is psychological. It means mood symptoms can become major maintainers of fatigue and deserve serious treatment.
Psycho-oncology, counseling, and Acceptance and Commitment Therapy (ACT) can be useful. ACT doesn't try to argue you out of feeling tired. It helps patients reduce the way fatigue dominates decisions, identity, and daily behavior. For some people, that means less avoidance, better pacing, more engagement with meaningful activities, and lower distress around symptoms.
Clinical reality: When anxiety, insomnia, and fatigue travel together, treating only one of them rarely works.
If you tend to wake up already drained, it can also help to compare your pattern against common sleep issues. This overview of reasons for morning fatigue is a practical complement to the cancer-specific discussion.
Nutrition, hydration, and sleep still matter
These aren't glamorous interventions, but they are foundational. Fatigue gets worse when patients are under-fueled, dehydrated, or sleeping in short, fragmented bursts.
A good plan usually includes:
- Regular eating even when appetite is low
- Protein and calorie support when intake drops
- Hydration through the day rather than all at once
- A consistent sleep routine
- Lower stimulation late at night
- Daytime light exposure and some movement to support circadian rhythm
What doesn't usually help is chasing energy with sugar, caffeine late in the day, or long daytime naps that steal nighttime sleep.
Summary of fatigue management strategies
| Strategy | Description | Key Takeaway |
|---|---|---|
| Medical review | Evaluate anemia, pain, medication effects, sleep disruption, and other reversible drivers | Fatigue often improves when the underlying cause is treated |
| Structured exercise | Use gentle aerobic and strength-based activity scaled to tolerance | Consistency beats intensity |
| Psycho-oncology support | Address anxiety, depression, distress, and symptom coping with counseling or ACT | Mental health care is fatigue care |
| Nutrition and hydration | Maintain regular intake, especially during treatment weeks | Low fuel worsens low energy |
| Sleep hygiene | Protect nighttime sleep and reduce behaviors that fragment rest | More time in bed doesn't always mean better restoration |
| Activity pacing | Alternate activity and recovery to avoid crash cycles | Overdoing good days often backfires |
A good fatigue plan should feel realistic. If it looks impressive on paper but can't be followed on your hardest days, it's the wrong plan.
Practical Tips for Conserving Your Energy
One of the most useful ways to think about fatigue is as a limited daily budget. Some patients use the “spoon theory.” Others call it an energy bank. The principle is the same. You don't wake up with endless capacity, so spending has to be deliberate.
That doesn't mean living timidly. It means protecting energy for what matters most.

Pacing through the day
Many patients feel best in the morning and assume that means they should “get everything done.” Then they crash by early afternoon. Better pacing usually works like this:
- Break tasks into smaller units: Fold one basket of laundry, not all of it.
- Pause before you feel wiped out: Resting early works better than recovering late.
- Alternate task types: Follow a physical task with a seated one.
A chair in the shower, a stool in the kitchen, or sitting to get dressed can preserve surprising amounts of energy. These changes aren't giving in. They're smart energy management.
Planning and prioritizing
It helps to decide what needs your best hours.
Try a simple sort:
- Must do: medications, meals, treatment, key calls
- Should do: one household task, a short walk, a needed errand
- Could do: lower-priority chores that can wait
Many patients benefit from planning meals, rides, and errands on paper rather than making repeated decisions when they're already drained. Nutrition also matters here. If eating has become difficult, this guide to nutrition for cancer patients offers practical ideas to discuss with your team.
Permission to accept help
A 2019 meta-analysis of more than 12,000 breast cancer survivors found that having a partner was associated with a lower risk of severe fatigue after treatment in this Annals of Oncology analysis. The message isn't that only partnered patients do better. The message is that social support matters.
Support can look like many things:
- Someone driving you to treatment
- A friend handling groceries
- A family member taking over school pickup
- A neighbor dropping off dinner
- A coworker helping reorganize deadlines
Ask for help in concrete terms. “Can you bring soup on Tuesday?” works better than “Let me know if you need anything.”
The hardest part for many patients is permission. Permission to say no. Permission to leave early. Permission to rest before you've “earned” it. That shift can reduce both fatigue and the guilt that often rides alongside it.
Partnering with Your Care Team at Hirschfeld Oncology
Breast cancer and fatigue deserve direct, ongoing attention. Fatigue can begin before treatment, intensify during therapy, and sometimes persist long afterward. It may reflect the cancer itself, treatment effects, anemia, poor sleep, emotional distress, or several overlapping problems at once.
That complexity is exactly why generic advice falls short. Patients do best when fatigue is tracked carefully, discussed early, and managed with a plan that combines symptom review, medical treatment, structured movement, sleep support, nutrition, and psycho-oncology when needed.
This becomes even more important in advanced or treatment-resistant disease. When care decisions involve immunotherapy, targeted therapy, low-dose chemotherapy, or other individualized regimens, quality of life isn't a side issue. It is one of the central outcomes that guides treatment choice.
In Brooklyn, many patients are looking for more than a standard protocol. They want honest conversations about trade-offs. They want treatment that aims for control without unnecessary toxicity. They want a team that understands that preserving function, stamina, and independence matters.
If fatigue is worsening, interfering with safety, or changing what you can do day to day, bring it up clearly and early. Don't minimize it. Don't assume it's something you just have to endure. And don't wait until you're in a crisis to ask for help.
For patients and families in Williamsburg, Bushwick, and the surrounding New York City communities, careful symptom management should be part of good cancer care from the start, not an afterthought.
If you're dealing with persistent fatigue during or after breast cancer treatment and want a more individualized approach, Hirschfeld Oncology offers patient-centered cancer care focused on thoughtful treatment selection, close monitoring, and quality of life. Patients, caregivers, and referring physicians can request a consultation to discuss supportive care strategies, advanced treatment options, and a plan specific to personal goals and tolerability.
.png)
.png)




