




.png)


The call often comes fast. A biopsy was done because a lymph node grew quickly, or abdominal pain led to a scan, and now you're hearing a phrase you may never have heard before: Burkitt lymphoma.
Most families register two things at once. First, this cancer moves quickly. Second, treatment needs to start quickly. Both are true. The part many people don't hear clearly enough in that first conversation is this: Burkitt lymphoma is also one of the most treatable aggressive cancers we see, and modern burkitt lymphoma treatment is built around cure.
Understanding Your Burkitt Lymphoma Diagnosis
Burkitt lymphoma is an aggressive B-cell non-Hodgkin lymphoma. It grows fast, which is frightening, but that same biology also makes it highly sensitive to the right chemotherapy-based treatment.
That's why the diagnosis phase can feel compressed. A patient may go from symptom evaluation to biopsy result to hospital admission or treatment planning in just a short stretch of time. Families sometimes worry that the speed means the outlook must be poor. In Burkitt lymphoma, the opposite can be true. We move fast because this disease responds best when we act decisively.
The most important fact to hold onto is that Burkitt lymphoma has become one of oncology's major success stories. Cure rates now exceed 90% in pediatric populations and 80% in carefully selected adult cohorts treated with modern dose-intensive chemotherapy regimens, according to a review in PMC on Burkitt lymphoma outcomes and treatment evolution.
What this diagnosis means in practical terms
When I explain this diagnosis to families, I usually frame it this way: the cancer is urgent, but it is not hopeless. Urgent and treatable can exist together.
A few points matter right away:
- This is usually treated with curative intent. The plan isn't merely to slow the disease down.
- Treatment choices are deliberate. Your team isn't picking the strongest-sounding regimen. They're matching intensity to your body, your age, your disease burden, and your risk of complications.
- The pathology matters. The exact biopsy findings guide treatment, so if you're still trying to understand the report, this guide on how to read a pathology report can help you decode the terminology.
Burkitt lymphoma is one of the few cancers where speed matters enormously, but modern treatment also gives us real reason for hope.
Why people feel overwhelmed so quickly
The first days after diagnosis are usually packed with scans, blood work, discussions about fertility, infection prevention, hospital logistics, and treatment consent. That pace is normal. It reflects the biology of the disease, not a lack of control.
What helps most is focusing on the immediate next step, not the entire course at once. First confirm the diagnosis. Then stage the disease. Then protect the kidneys and metabolic system before chemotherapy begins. Then start the right regimen. That sequence is the foundation of effective burkitt lymphoma treatment.
How Diagnosis and Staging Shape Your Treatment Path
A 32-year-old and a 72-year-old can both hear the words "Burkitt lymphoma" on the same day and still need very different treatment plans. The biology matters. So does the body that has to get through treatment.
The early workup gives your team the information needed to choose the right intensity. In Burkitt lymphoma, that decision has real consequences. Too little treatment can miss the chance for cure. Too much treatment in a frail patient can cause serious complications before the lymphoma is under control.
The tests that shape the plan
Doctors usually build the first treatment plan from several pieces of information taken together:
- Imaging studies to see where lymphoma is present and whether there are bulky masses
- Blood tests, including LDH, kidney function, liver function, and uric acid
- Bone marrow testing when marrow involvement is suspected or needs to be ruled out
- Evaluation for CNS disease, because Burkitt lymphoma can involve the brain or spinal fluid at diagnosis
- A fitness assessment, including performance status, heart and kidney reserve, and other medical problems
Biology can also matter beyond standard staging. Some patients benefit from a better understanding of how lab and tumor features guide treatment choices. This primer on what molecular testing means in cancer care explains that broader concept in plain language.
Stage is only part of the story
Patients often focus on stage first. That is reasonable, but stage alone does not decide the regimen.
In practice, oncologists also look at tumor bulk, LDH, marrow or CNS involvement, symptoms, organ function, and whether the patient can tolerate inpatient intensive therapy. For younger adults with good organ reserve, standard high-intensity treatment may be the best path because it offers the strongest chance of cure. For older adults, or for patients with diabetes, heart disease, reduced kidney function, or poor functional status, the conversation becomes more nuanced. The goal is still cure whenever it is realistic, but the regimen may need adjustment so treatment remains deliverable.
That trade-off is not a compromise in the casual sense. It is clinical judgment.
What "low risk" and "high risk" mean in real life
In Burkitt lymphoma, risk grouping helps teams estimate how aggressive the disease is and how much treatment a patient is likely to need. "Low risk" does not mean a mild cancer. It usually means the pattern of disease may allow a shorter or less intensive approach without clearly giving up the chance of cure.
"High risk" often means a larger disease burden, involvement of the marrow or central nervous system, a very high LDH, or other features that raise the likelihood of complications and relapse. Those patients often need a more intensive plan and closer monitoring.
For adults, especially adults over 60, real-world care can differ from trial language. Clinical trials often enroll fitter patients who can tolerate demanding regimens. In daily practice, oncologists have to ask a harder question: can this specific patient complete the treatment safely enough for it to work? That is one reason two excellent cancer centers may recommend slightly different approaches for the same diagnosis.
Questions worth asking at the first treatment meeting
A useful discussion early on should answer these questions clearly:
- Where is the lymphoma located? Nodes, abdomen, marrow, spinal fluid, or several sites.
- Is this considered lower-risk or higher-risk disease, and why? Ask which findings are driving that label.
- How much treatment can my body safely tolerate? Age alone should not decide this, but age does affect risk.
- Will I need CNS-directed treatment? That changes both the regimen and the schedule.
- Do I need care at a center that treats Burkitt lymphoma often? Experience matters, especially if treatment will be intensive.
For patients in New York City, this part is especially practical. If the plan may require inpatient chemotherapy, rapid lab turnaround, transfusion support, lumbar punctures, and experienced ICU backup, it is reasonable to ask whether your care should be centered at a major academic or high-volume lymphoma program. In Burkitt lymphoma, access to that infrastructure can shape outcomes as much as the drug names on the consent form.
When families understand why a plan is being recommended, the process feels less arbitrary and more grounded in the facts of the disease and the patient in front of us.
Urgent First Steps Managing Tumor Lysis Syndrome
Before the first full cycle of chemotherapy, the immediate concern is often tumor lysis syndrome, usually shortened to TLS.
Burkitt lymphoma cells can break apart very quickly once treatment starts. That sounds like good news, and in one sense it is. But when too many cancer cells die at once, they release their contents into the bloodstream faster than the body can clear them. The kidneys can get overwhelmed. Electrolytes can shift dangerously. Heart rhythm problems and kidney injury can follow.
Why teams prepare before they “attack” the lymphoma
The simplest analogy is a drainage system after a sudden flood. If too much debris hits at once, the pipes clog before the water clears.
That's why burkitt lymphoma treatment often begins with preventive measures before the main chemotherapy is underway. Common steps include:
- IV hydration to help the kidneys flush waste products efficiently
- Frequent blood testing to catch changes early
- Medicines such as allopurinol or rasburicase to reduce the impact of uric acid buildup
- Close monitoring in the hospital when tumor burden is high or lab risk is concerning
What families should expect in the first days
These early days can feel strangely anticlimactic because much of the work looks supportive rather than anticancer. Fluids run. Nurses draw labs repeatedly. Medications are given to prevent complications. That isn't delay. It's part of treatment.
The safest Burkitt lymphoma treatment plan is often the one that respects how fast the cancer dies, not just how fast it grows.
If your team is talking about hydration, kidney protection, urine output, or repeated chemistry panels, they're doing exactly what they should. Preventing TLS is one of the first signs that the plan is thoughtful and experienced.
Standard Intensive Chemo-Immunotherapy Regimens
A common early conversation goes like this. The family hears that Burkitt lymphoma grows fast, reads that it is often curable, and assumes the strongest regimen is automatically the best choice. In practice, the decision is more exacting. The goal is still cure, but the treatment has to be strong enough to control the lymphoma and tolerable enough for the patient to finish it safely.
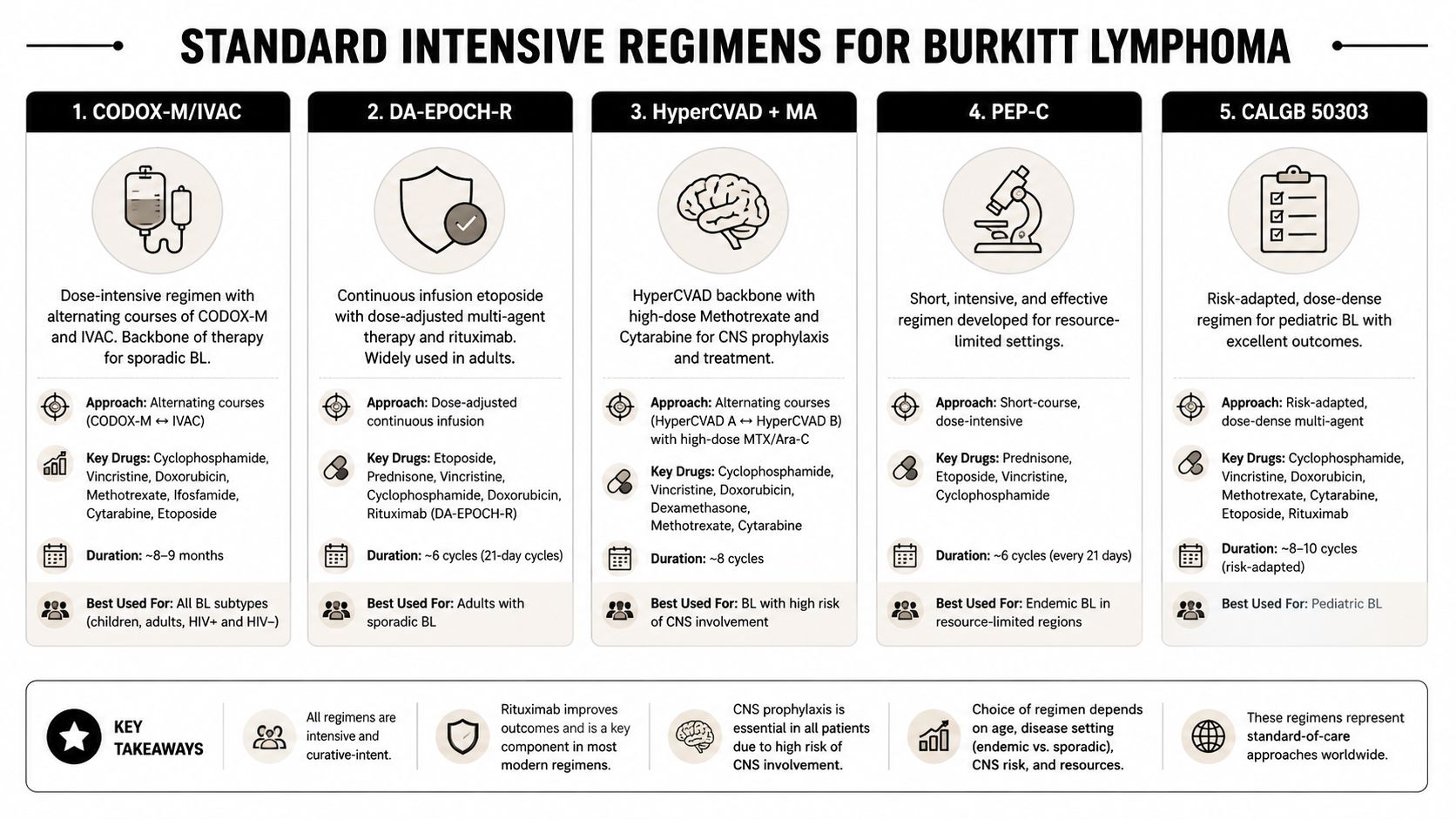
For many years, the backbone of Burkitt lymphoma treatment has been intensive multi-agent chemo-immunotherapy. Regimens such as R-CODOX-M/IVAC, R-Hyper-CVAD, and pediatric-derived programs combine several chemotherapy drugs with rituximab because Burkitt lymphoma can outgrow weaker treatment. These are not casual outpatient plans. They often require admission, frequent lab checks, transfusion support, infection prevention, and rapid response if kidney function, liver tests, or blood counts shift.
If you want a plain-language refresher on why these drugs are combined and timed so carefully, this guide on how chemotherapy works explains the basics.
What makes these regimens hard to deliver
Intensity comes from more than the drug names. It comes from dose, schedule, and the expectation that each cycle stays on track. Burkitt lymphoma is one of the diseases where timing matters, so treatment delays caused by infection, severe mucositis, organ injury, or prolonged low blood counts can undermine the plan.
These regimens usually include:
- Several active drugs given in close sequence
- Rituximab to target CD20-positive lymphoma cells
- High supportive care needs, often including growth factor support, transfusions, and inpatient monitoring
- CNS-directed therapy as part of the full treatment strategy
Why “standard” does not mean “right for every adult”
Clinical reality and trial results often diverge. A regimen developed in younger or highly selected patients may still be the best curative option for a healthy 28-year-old. The same regimen can be dangerous in a 74-year-old with diabetes, reduced kidney function, or limited help at home after discharge.
Real-world series in adults have shown that treatment failure and treatment-related death remain meaningful risks outside ideal trial populations, especially when patients are older or medically fragile, as reviewed in a recent adult Burkitt lymphoma update in Blood. The practical lesson is straightforward. Fitness matters as much as intent.
The best regimen is the most effective treatment a patient can realistically complete, not the most aggressive protocol listed on paper.
That distinction matters a great deal in adults and older adults. I often frame it this way for families: we are not choosing between “strong treatment” and “weak treatment.” We are choosing between a plan that offers curative pressure against the lymphoma and a plan that the patient's body can tolerate without losing the window to continue therapy.
Comparison of Common Burkitt Lymphoma Regimens
| Regimen | Typical Patient | Intensity & Setting | Key Feature |
|---|---|---|---|
| R-CODOX-M/IVAC | Younger, fit patients | Very intensive, often inpatient-heavy | Designed for rapid, high-power disease control |
| R-Hyper-CVAD | Selected fit adults | Intensive, usually requires close hospital-level monitoring | Alternating cycles with strong CNS-conscious strategy |
| Pediatric-inspired regimens such as R-BFM | Children, adolescents, some selected young adults | Intensive, specialized supportive care required | Built from regimens associated with excellent pediatric outcomes |
| LMB-based approaches | Selected patients in experienced centers | High intensity with substantial supportive care demands | Effective but can carry major toxicity burdens |
| Intensive rituximab-containing multidrug programs broadly | Fit adults with curative intent | High intensity, often inpatient or hybrid | Favors early disease eradication with little margin for poor tolerance |
How experienced teams make the choice
The deciding factors are concrete. Age matters, but physiologic reserve matters more. Kidney function, liver function, performance status, HIV control when relevant, baseline neuropathy, cardiac history, active infections, and the ability to return quickly for fever or dehydration all shape the plan. Social support matters too. A patient living alone on the fifth floor without reliable transportation faces different risks than a patient with family nearby and easy access to the treating center.
For a younger adult with good organ function, standard intensive therapy may offer the best chance of cure. For an older adult, or for someone already strained by other illnesses, the wiser choice may be a modified or dose-adjusted approach discussed in the next section. That is not backing away from treatment. It is good oncology. In New York City, where access to tertiary centers is better than in many parts of the country, patients should ask a direct question early: Does this team routinely treat adult Burkitt lymphoma, and how do they adjust intensity for older or less fit patients? The answer often tells you how individualized your care will be.
Protecting the Brain with CNS Prophylaxis
A common moment in the first treatment discussions goes like this. The scans show lymphoma in the abdomen, chest, or marrow, and then the team says they also need to protect the brain and spinal fluid. Families are often surprised by that shift. The reason is that Burkitt lymphoma can reach the central nervous system early, and standard IV chemotherapy may not give reliable coverage in that space.
That is why many treatment plans include CNS prophylaxis, usually with intrathecal chemotherapy given through a lumbar puncture. In some cases, the broader chemotherapy regimen also contributes CNS-active treatment, but direct treatment into the spinal fluid is still a routine part of care for many patients.
Why this step matters
The goal is to prevent a relapse in one of the hardest places to treat. Even when the visible lymphoma is outside the brain, a small number of lymphoma cells can be present in the cerebrospinal fluid or nearby tissues. If those cells are missed early, the disease can return in a way that is more dangerous and harder to control.
This matters for adults in particular. Younger patients often tolerate repeated lumbar punctures and intensive schedules better. Older adults, or patients who are already weak from bulky disease, kidney strain, infection, or severe weight loss, may find this part of treatment more taxing. The answer is usually not to skip it. The answer is to plan it carefully, with an experienced team that knows how to reduce procedure-related headaches, manage anticoagulation issues, and coordinate timing with the rest of chemotherapy.
What intrathecal treatment is actually like
The procedure is similar to a spinal tap. The lower back is cleaned and numbed, a needle is placed into the fluid space, and the medication is injected directly into the cerebrospinal fluid. The treatment itself is usually brief.
Patients often ask what it feels like. Pressure is more common than sharp pain. The side effect I discuss most often is headache afterward, along with fatigue, temporary back soreness, or nausea. These risks are real, but they are usually manageable. Good hydration, careful positioning, and experienced technique make a difference.
If Burkitt lymphoma is already present in the CNS, the schedule is often more intensive than standard prophylaxis. That can mean more lumbar punctures, closer neurologic follow-up, and a treatment plan built around both disease control and tolerability.
The real-world trade-off
CNS prophylaxis is one of the clearest examples of why Burkitt lymphoma treatment has to be individualized. On paper, the logic is straightforward. In practice, a 28-year-old with strong organ function and a 78-year-old with diabetes, atrial fibrillation, and borderline kidney function do not experience this step the same way.
For a fit patient, the main challenge may be inconvenience and temporary discomfort. For an older adult, each lumbar puncture can have more ripple effects. Dehydration, post-procedure headache, confusion after sedation, trouble arranging transportation home, or difficulty returning quickly for fever all matter. In New York City, where traffic, parking, and long travel times between boroughs can turn a short procedure into an all-day event, those details are part of treatment planning, not side issues.
How to discuss it with your team
Ask direct questions:
- Why is CNS prophylaxis recommended in my case?
- Am I getting preventive treatment only, or is there concern for active CNS involvement?
- How many lumbar punctures are planned, and can the schedule change if side effects build up?
- What symptoms after the procedure should trigger a same-day call?
- If I am older or medically fragile, how will you adjust the plan to keep treatment on track?
Families do better with this part of care when they understand its purpose. Intrathecal chemotherapy is invasive. It is also a deliberate attempt to close off a known route of relapse. For many patients, that added layer of treatment is part of giving curative therapy its best chance to work.
Modern Approaches for Adults Dose-Adjusted Therapy
A common adult Burkitt lymphoma conversation goes like this: the disease is aggressive, cure is still the goal, and the hardest question is often how much treatment a particular patient can safely absorb without losing time to complications. That question comes up most often in adults who are no longer 25, and in older patients whose heart, kidneys, nerves, or stamina may not tolerate the same plan used in a younger trial population.
One of the main regimens that changed this discussion is DA-EPOCH-R, short for dose-adjusted etoposide, prednisone, doxorubicin, cyclophosphamide, and rituximab. In practice, its appeal is straightforward. It aims to preserve curative intent while adjusting treatment intensity to the patient's marrow recovery and side effects from the prior cycle.

Why DA-EPOCH-R is different
Unlike fixed high-intensity regimens that start at full strength for nearly everyone, DA-EPOCH-R is built around adjustment. The chemotherapy is typically infused over 96 hours per cycle, and the dose in later cycles is raised or lowered according to how the blood counts recover and whether serious toxicity developed. That design matters in the clinic because Burkitt lymphoma treatment fails patients in two ways. Sometimes the lymphoma is not controlled. Sometimes the regimen is so hard on the patient that infections, organ injury, prolonged hospitalization, or treatment delays become the dominant problem.
The National Cancer Institute press release on adult Burkitt lymphoma and DA-EPOCH-R highlights why many centers adopted this approach for selected adults. The regimen can often be delivered outside the hospital and may reduce some of the acute toxicity seen with older intensive platforms.
That does not make it easy treatment.
Patients still need frequent labs, growth factor support, careful infection precautions, and a team that can react quickly if fever, dehydration, neuropathy, or low counts develop.
Which adults are most likely to benefit
The best candidate is not the oldest patient in the room. Age matters, but physiologic reserve matters more.
DA-EPOCH-R often enters the discussion for adults who may still be treated with curative intent but who carry a narrower margin for toxicity, including:
- Patients with borderline organ function, where fixed very high doses may be harder to deliver safely
- Adults with important comorbidities, such as cardiac disease, diabetes, or kidney impairment
- People at higher risk from long inpatient stays, including those who decondition quickly or have limited caregiver support
- Older adults, especially when the team is trying to balance disease control with the actual risk of treatment-related harm
In real-world practice, this is the trade-off. A more intensive regimen may look stronger on paper for a very fit patient. A dose-adjusted program may be the better route if it gives an older or more medically fragile adult the best chance of completing curative therapy without repeated interruptions.
What the evidence supports, and where caution is still warranted
Prospective studies helped establish DA-EPOCH-R as a serious option in adults with Burkitt lymphoma, and follow-up from the original NCI-led work showed durable remissions in many patients treated on this platform. The full study report in the Journal of Clinical Oncology is a better source for those outcomes than a secondary summary, and it is the paper many hematologic oncologists look back to when discussing this regimen.
Still, trial results do not remove bedside judgment. Patients seen in daily practice are older on average, carry more comorbid illness, and do not all have the same access to rapid lab checks, infusion support, emergency evaluation, or experienced lymphoma nursing teams. For an adult in their 60s or 70s, the question is rarely just whether DA-EPOCH-R can work. The question is whether the person can complete it safely enough to give it a fair chance to work.
That distinction deserves a plain conversation with the treating team.
Here's a short overview of the treatment philosophy behind infusion-based care in adults:
Outpatient treatment changes the experience of care
For the right patient, outpatient delivery changes more than location. Sleeping at home, eating familiar food, staying in motion, and having family nearby can make a meaningful difference during repeated cycles of chemotherapy. I have also seen the opposite problem. A regimen that is technically outpatient can become harder than an inpatient admission if the patient lives alone, cannot get to urgent labs, or has no reliable way to reach the cancer center quickly when fever starts at 10 p.m.
That is especially relevant in New York City. Infusion pumps, return visits, blood count checks, and same-day evaluations are manageable only if the logistics work. Borough-to-borough travel, weather, caregiver availability, and proximity to an emergency department that communicates well with the oncology team all affect whether outpatient therapy is a smart choice or a risky one.
A sound adult Burkitt lymphoma plan matches the biology of the disease to the patient's actual ability to complete treatment.
What about relapse or refractory disease
If Burkitt lymphoma does not respond adequately or returns after treatment, the strategy changes quickly and usually requires input from a center with expertise in aggressive lymphoma. Depending on the pattern of relapse and the patient's condition, options may include salvage chemotherapy, stem cell transplant, CAR-T cell therapy, or a clinical trial.
This setting is harder than first-line treatment, and candid discussion matters. Some patients remain candidates for aggressive salvage. Others need a plan that is still active but more realistic about tolerability, hospitalization risk, and the likely benefit of each next step.
Finding Your Path Forward in New York City
If you or a family member is facing Burkitt lymphoma in New York City, the practical question is not just which regimen exists. It's which regimen makes sense for this patient, right now, with the local resources available to support it safely.
That distinction matters most in adults. Younger, very fit patients may still do best with a classic intensive inpatient strategy. Many older adults and patients with other health problems need a more individualized conversation. The evidence gap is real. The NIH summary of the less toxic adult Burkitt lymphoma alternative notes that data on DA-EPOCH-R specifically in elderly adults over 65 remain limited, even though standard regimens are often especially toxic in this group.
What to ask at your consultation
Bring a written list. In a fast-moving diagnosis, people forget what they meant to ask.
Consider these questions:
- Am I being treated with curative intent? Most patients should hear a direct answer.
- Why is this regimen the best fit for me specifically? Ask what factors drove the choice.
- How worried are you about tolerability in my case? This matters as much as effectiveness.
- Will I need CNS prophylaxis or treatment? If yes, ask how it will be delivered.
- What supportive care is in place for infection risk, low blood counts, and tumor lysis syndrome?
- Would a second opinion change the plan or just confirm it? Either outcome can be valuable.
Why expertise matters in NYC
New York gives patients access to major cancer programs, but access alone isn't enough. Burkitt lymphoma requires a team that can make rapid decisions, manage complications early, and adjust treatment when the original plan stops fitting the patient.
For older adults in Brooklyn, Williamsburg, Bushwick, and the surrounding city, that often means looking for clinicians who are comfortable with the gray areas, not just the textbook pathways. The best adult Burkitt care usually comes from a careful balance of urgency, experience, and honest risk assessment.
You do not need false reassurance. You need a team that can explain the trade-offs clearly, move quickly, and preserve the chance of cure without ignoring the cost of treatment itself.
If you're in New York City and need help weighing intensive therapy against a more individualized, lower-toxicity approach, Hirschfeld Oncology offers compassionate consultation, outpatient infusion support, and practical guidance for patients and families navigating complex cancer treatment decisions.
.png)
.png)




