




.png)


You open the patient portal, see a red flag next to calcium, and your mind jumps straight to the worst conclusion. That reaction is completely understandable. A high calcium result during cancer treatment can feel like one more problem piled onto an already heavy situation.
But this finding has a name, a pattern, and a treatment path. In oncology, hypercalcemia means calcium in the blood is higher than it should be. It can be serious, especially when symptoms are building, but it's also a well-known complication that cancer teams deal with regularly.
What matters most is not panicking and not ignoring it. A high calcium result is a signal. The job is to figure out what your body is trying to tell us, how urgent it is, and what we can do next.
Understanding a High Calcium Result
A lab report that says “high calcium” often creates more confusion than clarity. Patients ask whether they ate the wrong food, took too many supplements, or whether this means the cancer has suddenly worsened overnight. Usually, it's more complex than any one meal or one pill.
In cancer care, high calcium and cancer often show up together because some tumors can disrupt the body's normal calcium controls. This is not rare. The Endocrine Society notes that hypercalcemia of malignancy affects 2% to 30% of patients with cancer, and the most common cause is PTHrP-driven hypercalcemia, which accounts for about 80% of cases (Endocrine Society overview of hypercalcemia of malignancy).
What the calcium number actually means
Calcium in the blood helps nerves fire, muscles contract, and the heart beat in a steady rhythm. Your body normally regulates it tightly. When that control slips, symptoms can range from dry mouth and constipation to confusion and dangerous dehydration.
If you want a plain-English refresher on how calcium is measured and why lab interpretation can be tricky, this Lola health calcium test analysis is a helpful background read. In oncology, though, the question isn't only “Is the number high?” It's also “Why is it high in this person, right now?”
A calcium result doesn't stand alone. Doctors read it alongside symptoms, kidney function, medications, hydration status, and the overall behavior of the cancer. They also ask whether this might fit into a broader pattern of tumor signaling, which is part of why cancer teams pay so much attention to cancer biomarkers.
Practical rule: A high calcium result is not a diagnosis by itself. It's a clue that needs context.
When oncologists become especially concerned
Some calcium elevations are mild and picked up on routine blood work. Others come with obvious symptoms and need same-day action. StatPearls, as summarized by the Endocrine Society page above, notes that calcium levels greater than 13 mg/dL at presentation should raise suspicion for malignancy.
That doesn't mean every high result is an emergency. It does mean the response should be deliberate. If a patient has cancer and develops high calcium, the medical team has to decide quickly whether this is a mild lab abnormality, an early warning sign, or an urgent complication that needs treatment now.
Why Cancer Can Cause High Calcium Levels
The easiest way to understand this is to think of calcium balance like a home thermostat. Under normal conditions, the body keeps blood calcium within a narrow range. Bones act like a storage bank, the kidneys help filter and hold the right amount, and hormones coordinate the whole system.
Cancer can break that thermostat in several different ways.
Hormone mimicry
The most common mechanism is that a tumor makes a substance called PTHrP. This substance behaves enough like parathyroid hormone that the body gets fooled into releasing more calcium into the bloodstream. It's as if the thermostat senses a false drop in temperature and turns the heater on even though the house is already warm.
This pattern matters because it explains why some patients develop high calcium even when there isn't obvious bone destruction on imaging. The tumor is sending a chemical instruction that shifts calcium regulation in the wrong direction.
Bone breakdown and kidney strain
Another route is direct damage to bone. When cancer spreads to bone, it can disrupt normal bone turnover and release stored calcium into the blood. Bone is not inert. It's active tissue. When metastatic disease injures it, calcium can spill out the way money leaves a cracked savings jar.
That process often overlaps with kidney stress. If a patient is dehydrated, weakened, or has reduced kidney function, the body has a harder time clearing excess calcium. The result can become self-reinforcing. High calcium worsens dehydration, dehydration worsens calcium clearance, and the patient starts feeling progressively worse.
For people dealing with metastatic spread to the skeleton, treatment decisions often overlap with broader planning around bone metastases treatment.

Less common patterns still matter
Some blood cancers, including myeloma, can drive bone breakdown through their own signaling pathways. A smaller group of cancers can alter vitamin D activity in a way that increases calcium absorption from the gut. These aren't the patterns most patients hear about first, but they remain part of the doctor's differential when the labs don't fit the usual script.
A useful way to think about it is this:
- Tumor sends a false hormone signal. Calcium rises even without obvious bone injury.
- Cancer damages bone directly. Stored calcium leaks into circulation.
- Kidneys can't keep up. Dehydration or renal impairment makes clearance harder.
- A rarer metabolic pathway is involved. Vitamin D or blood-cancer biology changes calcium handling.
High calcium is usually not random. In cancer care, there is almost always a mechanism we can identify and address.
Recognizing the Signs and Symptoms of Hypercalcemia
One reason hypercalcemia gets missed at first is that the symptoms can look like many other things. Fatigue can be blamed on chemotherapy. Constipation can be blamed on pain medication. Brain fog can be blamed on poor sleep, stress, or the cancer itself.
The pattern matters. When several of these symptoms appear together, high calcium should move higher on the list.
What mild symptoms can feel like
At the milder end, patients often describe a general slowdown. They feel washed out, nauseated, constipated, or less interested in food. Some develop vague abdominal discomfort. Others say, “I don't feel like myself.”
Those symptoms are easy to dismiss because they aren't dramatic. But they're often the earliest warning that the chemistry is drifting.
When symptoms become more concerning
As calcium rises further, the nervous system and kidneys start to show the strain more clearly. Patients may become very thirsty, urinate more often, or seem unusually dehydrated. Family members sometimes notice irritability, trouble concentrating, or confusion before the patient does.
That shift is important. Hypercalcemia can move from uncomfortable to dangerous faster than many people expect, especially if dehydration is already present.
| Severity Level | Common Symptoms ("The Moans, Groans, Stones, and Bones") |
|---|---|
| Mild | Fatigue, constipation, nausea, poor appetite, vague abdominal discomfort, mild bone discomfort |
| Moderate | Increased thirst, increased urination, dehydration, worsening constipation, more noticeable weakness, trouble concentrating, mood changes |
| Severe | Marked confusion, lethargy, difficulty staying awake, severe weakness, vomiting, signs of kidney failure, stupor, coma |
Red flags that need urgent attention
Some symptoms should prompt immediate medical contact the same day, and some should prompt an emergency evaluation.
- New confusion: If a patient seems disoriented, slow to answer, or unusually sleepy, don't wait for the next routine appointment.
- Severe dehydration: Very dry mouth, minimal urine, dizziness, or inability to keep fluids down can signal a dangerous cycle.
- Rapid decline: If someone goes from functioning reasonably well to barely getting out of bed, that's not something to monitor casually at home.
- Caregiver alarm: If family members say, “This is not how they usually act,” that observation carries weight.
Don't judge urgency by the lab value alone. Judge it by the person in front of you.
A practical rule for families is simple. If symptoms are mainly annoying, call the oncology office promptly. If symptoms are affecting alertness, hydration, or safety, go to the hospital.
What High Calcium Signals About Your Cancer
This is often the hardest question because it isn't only medical. It's emotional. Patients usually want to know what the calcium result means for the cancer itself, not just how to lower the number.
In many cases, hypercalcemia is a sign that the cancer is biologically active and affecting the body beyond the original tumor site. The American Cancer Society, as summarized in the verified data, notes that it can happen when cancer is advanced or has spread to bone. That's hard information to receive, but it's also useful information. It helps the oncology team understand how the disease is behaving.
What it often means in practice
When I talk with patients about this finding, I try to separate two truths that can coexist.
First, high calcium can be a marker of serious disease activity. Second, it is still treatable, and treatment can make a patient feel much better fairly quickly. Those are not contradictory statements. Many patients hear “serious” and assume “nothing can be done.” That isn't accurate.
Doctors use this result to reassess the whole picture:
- Is the current cancer treatment still controlling the disease?
- Has bone involvement become more important?
- Is kidney function making the situation worse?
- Do we need symptom-focused treatment urgently while also adjusting the long-term cancer plan?
It can also be a biological clue before diagnosis
There's another side to this topic that many people haven't heard. Research has suggested that high blood calcium may appear before certain cancers are diagnosed. A Wake Forest Baptist Medical Center report from 2013 said it was the first study to find that higher blood calcium levels might predict ovarian cancer in some women (Wake Forest Baptist report on calcium levels and ovarian cancer).
That does not mean calcium causes cancer. It means calcium can sometimes function as an early biomarker, a signal that points toward disease before the diagnosis is obvious.
A high calcium result is not always a verdict. Sometimes it's the body revealing part of the story earlier than expected.
For someone who already has cancer, the key takeaway is more practical than philosophical. This result helps doctors understand disease behavior. It may affect prognosis, but it also guides action. It tells the team where to look, what to treat first, and how urgently the treatment plan may need to change.
How Doctors Diagnose and Treat Acute Hypercalcemia
When a patient has symptoms and the calcium is high, the first priority is stabilization. The second is identifying the cause. Those steps usually happen together, especially in the hospital or urgent outpatient setting.
Early in the workup, doctors repeat or confirm calcium testing and look closely at kidney function, hydration, and hormone patterns. Depending on the case, they may check PTH and PTHrP to distinguish cancer-related hypercalcemia from other causes of high calcium. If the broader picture suggests a blood disorder, some patients may also need more specialized evaluation, which can include procedures such as a bone marrow biopsy.
A visual summary helps many families follow the process:
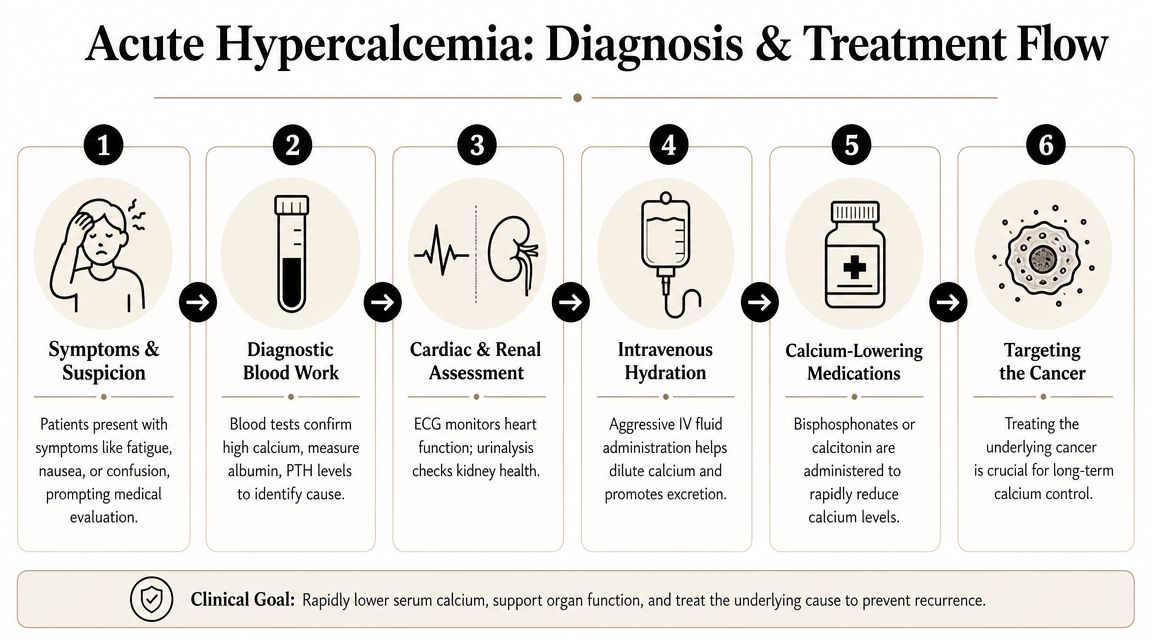
What treatment usually starts with
Most patients with significant hypercalcemia need IV fluids first. High calcium often dehydrates people, and dehydration makes the calcium harder to clear. Rehydration helps the kidneys do their job again.
After that, medication choice depends on severity, recurrence, kidney function, and the likely mechanism. For severe hypercalcemia, expert guidance recommends IV bisphosphonates or denosumab to suppress bone resorption, and calcitonin is often added at the beginning because it can lower calcium quickly, though it should be limited to 48–72 hours due to tachyphylaxis (guideline summary on treating high calcium in people with cancer).
Why these drugs work
Bisphosphonates and denosumab don't just chase the lab number. They target the biology that is driving calcium upward. If the problem is excessive osteoclast activity, these treatments slow the bone breakdown that keeps feeding calcium into the bloodstream.
Calcitonin works faster, but briefly. It's like using a fast-acting tool while waiting for the heavier treatment to take effect. That's why it's helpful at the front end but not as a long-term solution.
Later in the decision path, denosumab becomes especially important if hypercalcemia recurs despite bisphosphonate therapy. That situation tells the team that the first antiresorptive strategy wasn't enough or isn't durable enough for the biology of that cancer.
This short video can help patients visualize the emergency-to-treatment sequence:
What does not work well
Families often ask about drinking more water at home, stopping supplements, or waiting to see if the number comes down on its own. Those steps may help at the margins in mild cases, but they don't reliably treat significant cancer-related hypercalcemia.
Here's the practical distinction:
- Hydration helps. It supports kidney clearance.
- Calcitonin helps quickly. But only for a short window.
- Bisphosphonates or denosumab address the engine of the problem. They are the backbone of treatment.
- Treating the cancer itself remains essential. Without that, the calcium often returns.
Long-Term Management and Preventing Recurrence
Once the crisis has settled, the primary work becomes prevention. Patients usually want to know whether this will happen again, what they should watch for, and whether they need to change everything about their diet and supplements.
The answer is more nuanced than “avoid calcium.” In long-term management, oversimplified advice causes trouble.
The daily habits that matter most
Hydration is the most consistent practical safeguard. It won't fix cancer-driven hypercalcemia by itself, but it helps reduce the chances that mild calcium elevation will snowball into a more symptomatic episode.
Patients also do better when they know their own early warning signs. If constipation, nausea, unusual thirst, or mental clouding showed up before the first episode, those symptoms deserve quicker attention the next time.
- Stay ahead of dehydration: Sip fluids regularly, especially after infusion days, poor appetite, or vomiting.
- Report subtle symptoms early: Waiting until confusion or severe weakness develops makes treatment harder.
- Keep follow-up labs on schedule: Trends matter more than any one isolated blood draw.
- Review medications and supplements: Bring bottles or a full list to visits. Over-the-counter products count.

The supplement question patients ask all the time
Personalized oncology guidance is of great importance. Some patients on cancer therapies, especially postmenopausal women with ER-positive breast cancer on aromatase inhibitors, may be advised to aim for about 1,200 mg/day of calcium from food plus supplements to protect bone health, but excess calcium supplements or antacid use can itself contribute to hypercalcemia and kidney injury (Dartmouth Cancer Center discussion of calcium and cancer).
That's why “stop all calcium forever” is not a smart blanket rule. Some people need bone protection. Others need strict caution because their kidneys are under strain or their calcium is already unstable.
Ask a narrower question than “Should I take calcium?” Ask, “Given my treatment, kidneys, and recent labs, how much calcium is safe for me?”
Outpatient prevention often includes ongoing therapy
For some patients, long-term control includes repeat antiresorptive treatment such as bisphosphonates or denosumab in the outpatient setting. The right choice depends on recurrence pattern, cancer type, kidney function, and how well prior treatment worked.
What works best is a plan that connects symptoms, lab monitoring, infusion timing, and the underlying cancer strategy. What doesn't work is treating hypercalcemia like a one-time event when the cancer biology suggests it may return.
The Hirschfeld Oncology Approach to Care
High calcium is never just a chemistry problem. It affects thinking, appetite, kidney function, mobility, and whether a patient can continue cancer treatment safely. Good care has to bring all of those pieces together.
At Hirschfeld Oncology, the approach starts with the assumption that a flagged calcium level deserves context, not reflex. The team looks at symptoms, hydration, kidney function, cancer activity, medication history, and the patient's goals. For one person, the priority may be fast stabilization so treatment can continue. For another, the focus may be comfort, fewer hospital visits, and keeping care manageable close to home.
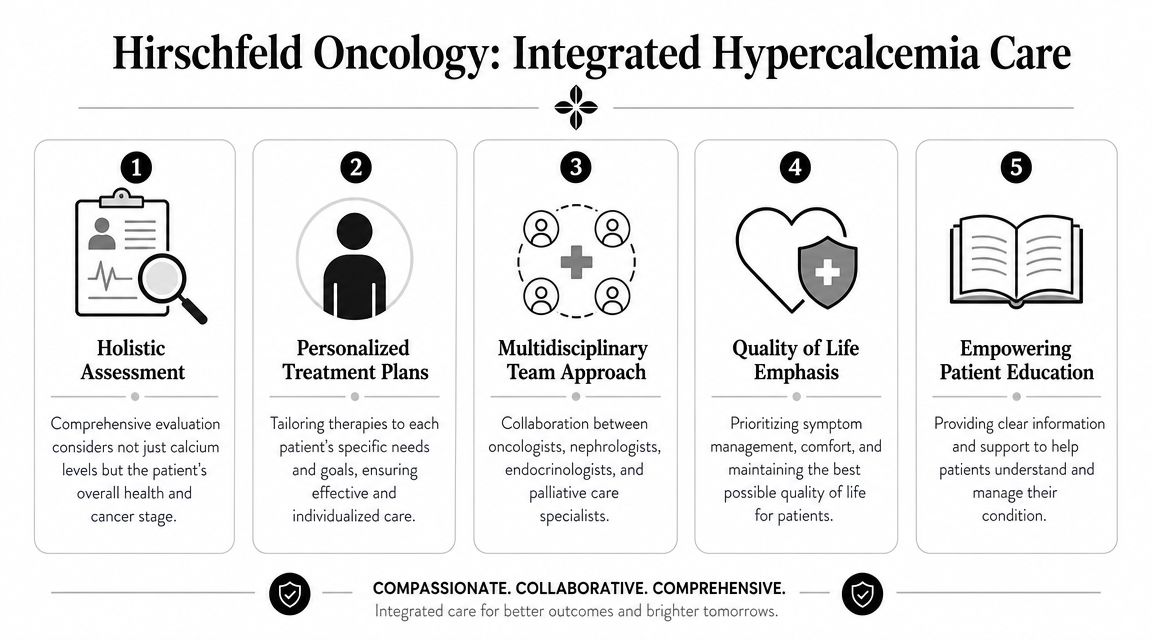
What integrated care looks like
The most effective management combines prompt symptom recognition with a treatment plan that fits the larger cancer picture. In practice, that means coordinating acute interventions, outpatient infusions, reassessment of the underlying cancer regimen, and clear patient education.
This model is especially valuable for people with advanced or treatment-resistant disease, because they often need more than a standard one-size-fits-all pathway. They need close monitoring without unnecessary delays, and they need decisions that reflect tolerability as well as disease control.
Why patients and families notice the difference
Families usually feel the difference when communication is clear. They know what symptoms matter, when to call, whether supplements are safe, and what the next lab or infusion is meant to accomplish.
That kind of care also helps reduce a common problem in oncology. A patient leaves the hospital feeling better, but no one has clearly explained how to prevent the next episode. Integrated follow-up closes that gap.
If you or a loved one is dealing with high calcium and cancer, Hirschfeld Oncology offers consultations for patients who need experienced, individualized cancer care with close monitoring, infusion support, and treatment planning aligned with quality of life as well as disease control.
.png)
.png)




