




.png)


A lot of people arrive at this question on a hard day.
You may have just heard that cancer has reached the bones. Or maybe your oncologist said you need a “bone-strengthening infusion,” and now you're trying to understand whether that means pain control, fracture prevention, or something more serious. Many patients and families nod in the office, then go home and realize they still don't have a clear picture of what the medicine is doing inside the body.
That confusion is understandable. Bone metastases sit at the intersection of cancer care, pain management, and bone biology. Patient handouts often make bisphosphonates sound simple. Research articles often make them sound impossible to follow. The truth is in between.
Bisphosphonates are established medicines used to protect bone. They don't attack cancer cells the same way chemotherapy or targeted therapy does. Instead, they help slow the damage cancer can cause in the skeleton. That matters because strong bones support movement, comfort, independence, and safety.
If you've been wondering how do bisphosphonates work, the short answer is this: they slow the cells that break bone down. That gives the body a better chance to preserve bone and reduce complications. But the full answer is more useful, especially if you're deciding about an infusion, weighing side effects, or preparing questions for your oncology visit.
Your Guide to Bone-Strengthening Cancer Treatment
A family is sitting in clinic. The scan review has already been hard. Then a new phrase enters the conversation: “bone-strengthening treatment.”
For many patients, that phrase brings two feelings at once. Relief, because there is a treatment that can help protect the skeleton. Anxiety, because it means the bones need that protection in the first place.
That reaction makes sense. By the time bisphosphonates come up, you may also be hearing about fracture risk, bone pain, dental checks, blood tests, and even high calcium caused by cancer. It is a lot to absorb, especially when you are already processing advanced cancer and making treatment decisions quickly.
What this treatment is trying to accomplish
Bisphosphonates are medicines used to slow bone breakdown. In advanced cancer care, the goal is straightforward. Protect the parts of the skeleton that cancer can weaken, so serious bone problems are less likely.
A helpful way to frame them is this: they are not the main anticancer treatment in the way chemotherapy, hormone therapy, immunotherapy, or targeted therapy may be. They are part of supportive cancer care that helps preserve comfort, function, and safety. For many patients, that translates into fewer interruptions to daily life and fewer bone-related emergencies.
Your oncology team may recommend them to lower the risk of problems such as:
- Fractures: Bones affected by metastases can break more easily
- Worsening bone pain: Ongoing bone damage can increase pain over time
- Reduced mobility: Pain or structural weakness can make walking, standing, or routine activity harder
- High calcium in the blood: Fast bone breakdown can release extra calcium into circulation
Bone protection matters because your skeleton is not just a set of x-rays. It is what lets you get out of bed, climb steps, sit comfortably, and move through the day with less fear of injury.
Why understanding the mechanism helps
Patients often feel calmer once the purpose of treatment is clear. A bisphosphonate can sound abstract at first, especially if it is introduced as an infusion added onto an already full cancer plan. Once you know that the medicine is aimed at slowing the bone damage process, the conversation becomes easier to follow.
That understanding also leads to better questions. You can ask why one drug was chosen over another, whether IV treatment fits your situation better than a pill, what side effects deserve a call, and how your team will monitor calcium, kidney function, and dental safety.
That is the middle ground many patients want. More detail than a brief handout, but in language that still makes sense during a stressful week.
How Cancer Can Weaken Your Bones
Your bones aren't static. They're living tissue, always being renewed.
A simple way to picture this is to imagine two crews working on the same building. One crew removes old, damaged material. The other crew lays down fresh, strong material. In bone, the demolition crew is made of osteoclasts. The construction crew is made of osteoblasts.
Normal bone remodeling
In healthy bone, these two crews stay in balance.
Osteoclasts break down older bone. Osteoblasts rebuild it. That ongoing exchange is called bone remodeling, and it's normal. It helps bones stay strong, repair wear and tear, and adapt over time.
| Bone cell | Simple role | Everyday analogy |
|---|---|---|
| Osteoclast | Breaks down old bone | Demolition crew |
| Osteoblast | Builds new bone | Construction crew |
When that process is balanced, the skeleton stays sturdy even though it's constantly changing.
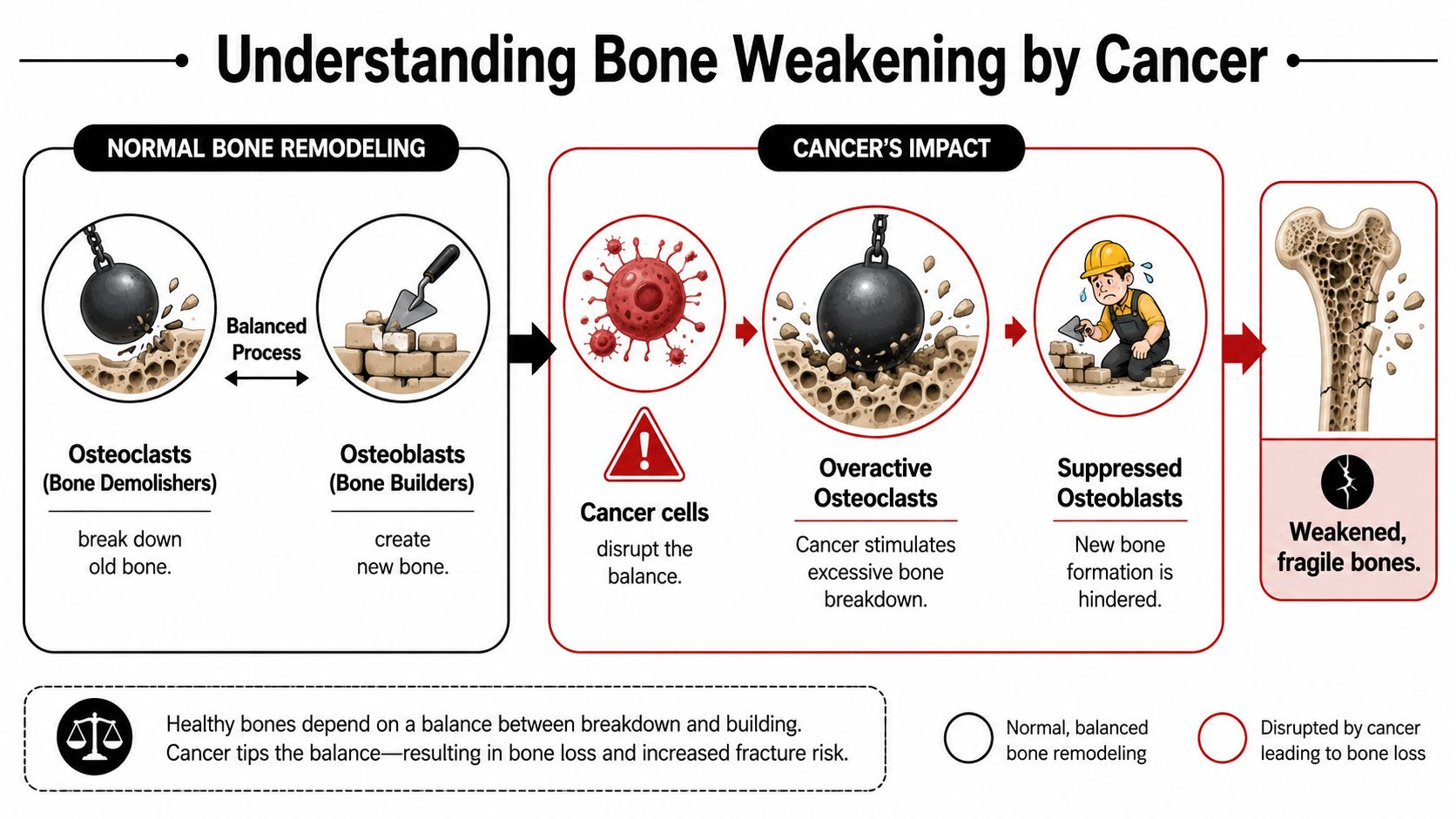
What changes when cancer reaches bone
Cancer cells can disrupt that balance.
In many cases, metastatic cancer in bone drives too much osteoclast activity. In plain language, the demolition crew starts working too aggressively. Bone gets cleared away faster than it can be rebuilt. Over time, that can create weak spots.
Those weak spots can lead to:
- Pain: Bone under stress often hurts before anything breaks
- Fragility: Bones may become less able to handle ordinary force
- Fracture risk: A weakened area can crack or collapse more easily
- High calcium levels: As bone is broken down, calcium can enter the bloodstream. If you want a plain-language explanation of that problem, this overview of high calcium and cancer is helpful.
Cancer in bone doesn't always mean the whole skeleton is failing. Often, it means certain areas are being remodeled in the wrong direction.
Where patients often get confused
Many people assume bone metastases only cause trouble if a bone breaks. That's not true. Damage often starts earlier. Pain, instability, and rising calcium can all happen before a visible fracture.
Another point of confusion is the phrase “bone-strengthening.” These medicines don't work like pouring cement into the bone. They work by calming down the part of the process that is removing too much bone too quickly.
That difference matters, because it explains both the benefit and the timing. The goal is to slow destruction so the skeleton has a better chance to hold up.
The Core Mechanism How Bisphosphonates Protect Bone
A common question in clinic sounds like this: “If this medicine is supposed to strengthen bone, how does it work once it gets into my body?”
The short answer is that bisphosphonates attach themselves to bone surfaces, especially the spots where bone is being worn away fastest. In advanced cancer care, that matters because those high-turnover areas are often the ones under the most stress.

A useful way to picture it is this. The drug settles into the bone surface like a protective coating in the places being actively dissolved. Then, when an osteoclast starts breaking down that patch of bone, it also pulls in the medicine. The cell that is causing the damage takes up the drug that interferes with its work.
That targeting explains why bisphosphonates are different from a medicine that circulates everywhere with the same effect in every tissue. They have a strong attraction to bone mineral, so their action is concentrated where bone resorption is happening.
What the drug does inside the osteoclast
The bisphosphonates most often used in oncology are usually the nitrogen-containing group. Inside the osteoclast, they block an enzyme called farnesyl pyrophosphate synthase, or FPPS, in the mevalonate pathway (review of bisphosphonate pharmacology and cellular effects).
Those terms are technical, so let's translate them into plain language. Osteoclasts need this pathway to maintain the internal tools that let them attach to bone, organize their cell membrane, and break bone down in an orderly way. When the pathway is blocked, the cell loses function. It becomes less able to resorb bone and may then undergo programmed cell death.
Practical rule: Bisphosphonates do not directly create new bone. They slow the removal of existing bone.
That distinction helps patients make sense of what these drugs can and cannot do. They are best understood as medicines that put the brakes on excess bone breakdown. Once that process slows, the bone-building side has a better chance to keep up.
Why this matters at the bedside
For patients and families, the mechanism leads to three practical effects:
- The drug goes where the problem is most active. Areas of rapid bone turnover attract more of the medicine.
- Overactive osteoclasts are suppressed. The cells driving excess bone loss become less effective.
- Bone gets more time to hold its structure. Slower breakdown can reduce ongoing weakening.
This short visual may help if you like seeing the concept explained another way:
One point that often surprises patients
Bisphosphonates can stay bound in bone for a long time. That long residence helps explain why some drugs in this class can be given at extended intervals in certain settings. In cancer care, the schedule is chosen differently than in osteoporosis, but the underlying principle is the same. The medicine remains anchored in bone and continues working at sites where osteoclast activity is high.
This is the part many patient handouts skip. Bisphosphonates do not “fill in” weak spots like plaster. They change the behavior of the cells removing bone, and that cellular effect is what helps protect the skeleton over time.
Types of Bisphosphonates and How They Are Given
A question families often ask in clinic is simple: if these medicines all protect bone, why are there different ones, and why does one person get a pill while another gets an infusion?
The short answer is that bisphosphonates belong to the same drug family, but they are not interchangeable in every cancer setting. Some attach to bone and shut down osteoclast activity more strongly than others. In advanced cancer, that difference matters because the goal is usually not routine bone maintenance. It is control of active bone damage with a treatment plan your oncology team can monitor closely.
Two main categories
Doctors often divide bisphosphonates into nitrogen-containing and non-nitrogen-containing drugs. That sounds technical, but the practical idea is straightforward. Both groups interfere with the cells that break down bone. They just do it in different ways.
Nitrogen-containing bisphosphonates block a pathway osteoclasts need in order to function and survive. Non-nitrogen-containing drugs are turned into compounds inside the cell that disrupt its energy use. If osteoclasts are the demolition crew, both drug types slow the crew down. The nitrogen-containing group usually does that more powerfully, which is why it is used more often in cancer-related bone disease and myeloma (drug class differences and potency).
| Type | How it works | Typical role in practice |
|---|---|---|
| Nitrogen-containing | Blocks a key osteoclast survival pathway | More often chosen when stronger suppression of bone breakdown is needed |
| Non-nitrogen-containing | Forms toxic ATP-like compounds inside osteoclasts | Used less often in modern oncology care |
Why the route matters
Bisphosphonates can be given by mouth or by intravenous infusion.
Oral forms are common in osteoporosis care. They can work well, but they come with practical limits. Absorption from the stomach is low and the instructions are strict. Patients usually have to take the pill on an empty stomach with plain water and stay upright afterward. For someone dealing with advanced cancer, nausea, swallowing problems, poor appetite, or a crowded treatment schedule can make that hard.
That is one reason oncology care often uses IV bisphosphonates instead. An infusion delivers the full dose directly into the bloodstream, avoids the absorption issue, and fits more easily with lab checks and clinic visits. For patients already receiving treatment for bone metastases and related complications, that route is often the more practical choice.
What patients commonly receive
In cancer care, the bisphosphonate used most often is zoledronic acid, given by IV infusion on a schedule set by your oncology team. Pamidronate is another IV option used in some situations. Oral drugs such as alendronate, risedronate, or ibandronate are far more familiar in osteoporosis than in metastatic cancer care.
If your doctor recommends an infusion, that does not mean a pill was weaker for everyone or that something has gone wrong. It usually means your team is matching the drug and the route to the problem in front of them: active bone metastases, risk of fracture, pain, calcium problems, kidney function, and the rest of your treatment plan.
This is a good place to ask specific questions. Which bisphosphonate are you recommending? Why this one instead of another? How often will I receive it? What blood work will you follow? Patients who understand those decisions tend to have clearer, more productive conversations with their oncology team.
Why Bisphosphonates Are Used in Advanced Cancer Care
A patient comes in with new back pain. A week earlier, walking was manageable. Now turning in bed hurts, standing feels uncertain, and the family is worried about what happens if the bone gives way. In advanced cancer, that is often the moment bisphosphonates enter the conversation. They are used to lower the strain that cancer can place on bone and to reduce the chance that one bone problem turns into several.

Three reasons oncologists use them
The first reason is direct protection. If cancer in the bone is speeding up breakdown, bisphosphonates can slow that process. That may help the bone stay more stable and can lessen the cycle of damage that feeds pain.
The second reason is to lower the risk of major bone complications, often called skeletal-related events. Doctors use that term as shorthand for problems such as fractures, spinal cord compression, or needing radiation or surgery because a bone has become painful or fragile. Patients do not need to memorize the label. The practical point is what matters. Fewer bone crises can mean safer movement, fewer urgent decisions, and more continuity in day-to-day life.
The third reason is treatment of hypercalcemia of malignancy. When bone breaks down quickly, calcium can rise in the blood. That can cause dehydration, confusion, constipation, weakness, and heart rhythm problems. In that setting, bisphosphonates are not being used solely to “strengthen bones.” They are part of treating a medical complication that can become serious quickly.
Why this role is so established
Bisphosphonates are used in advanced cancer because years of clinical practice have shown that controlling bone breakdown can prevent real complications, not just change lab values or scan wording. For patients and families, that distinction matters. The goal is often preserving function. Can you walk more safely, sit with less pain, avoid an emergency admission, or continue cancer treatment without a fracture disrupting the plan?
A simple way to picture it is this. If cancer has made the bone act like a wall that is being chipped away faster than it can be repaired, bisphosphonates help slow the workers doing the chipping. They do not remove the cancer by themselves, and they do not rebuild every damaged area. What they can do is buy stability, reduce risk, and support the rest of the treatment plan.
In advanced cancer, the aim is often fewer bone emergencies, steadier mobility, and more predictable daily life.
Where this fits in a broader plan
Bisphosphonates are one part of bone-directed care. They are often used alongside systemic cancer treatment, radiation, pain management, physical therapy, mobility aids, and fall-prevention steps. If you want a clearer picture of how those pieces fit together, this guide to treatment options for bone metastases can help.
Daily function matters here too. Some patients ask what movement is still safe when bones hurt or feel weak. Exercise plans need to be individualized, especially when metastases affect weight-bearing bones, but general resources on effective workouts for joint pain can help frame questions to bring to your oncology or rehabilitation team.
For some patients, an outpatient infusion center is part of that plan. Hirschfeld Oncology provides infusion-based cancer care and supportive treatment in Brooklyn as one option for patients who need coordinated management of advanced disease.
Managing Side Effects and Ensuring Your Safety
Patients often ask about side effects before they ask about the science. That makes sense. If you're considering an infusion, you want to know how you might feel and what the actual risks are.
The honest answer is that bisphosphonates are useful medicines with known tradeoffs. Patients generally tolerate them reasonably well, but safety depends on matching the drug to the patient and monitoring carefully over time.
Common concerns after treatment starts
With IV bisphosphonates, some patients feel temporarily achy or flu-like after treatment. Others notice fatigue for a short time. Teams also keep an eye on calcium and kidney-related labs, because those values matter when giving these medications safely.
With oral forms, the main issue is often irritation of the esophagus or stomach area. That's one reason oral dosing comes with strict instructions and why IV therapy is often preferred in oncology.
A few practical habits help:
- Stay in communication: Tell your team promptly about new pain, feverish feelings, or trouble swallowing
- Keep lab appointments: Blood work helps your clinicians judge safety before and during treatment
- Bring up dental plans early: Tooth extractions or major dental work may affect timing
Rare but serious risks
Longer-term use has been linked to atypical femur fractures, and oral forms can cause esophageal injury. Guidance also notes that therapy may need reassessment over time, including discussion of whether treatment should pause in some settings (benefit-risk discussion and reassessment).
In cancer care, patients also often hear about osteonecrosis of the jaw, usually shortened to ONJ. Even when a risk is uncommon, the name alone can be alarming. The important point is not to panic, but to prepare. A dental evaluation before treatment, good oral hygiene, and prompt reporting of jaw pain or exposed bone are standard precautions.
Don't wait for a side effect to become severe before mentioning it. Early reporting gives your team more room to adjust safely.
Questions worth asking your oncology team
A short checklist can make visits more productive:
- Do I need dental clearance first: Ask before starting, not after the first infusion.
- How will my kidneys be monitored: Your doctor may adjust treatment based on labs and overall health.
- What symptoms should trigger a call: New thigh pain, swallowing pain, jaw symptoms, or worsening bone pain deserve discussion.
- How long are we planning to continue: Duration is part of the treatment decision, not an afterthought.
For some patients, supportive movement also matters once pain is better controlled. If you're looking for gentle ideas, this guide to effective workouts for joint pain may be a useful starting point, especially if stiffness and reduced activity have become part of daily life.
If you're balancing several treatment effects at once, a broader guide to cancer side effects can help you keep symptoms organized for your care team.
Alternatives and Your Common Questions Answered
Bisphosphonates aren't the only way to slow bone breakdown. Another common option is denosumab, often known by the brand name Xgeva in oncology. It reaches the same broad goal through a different pathway. Instead of binding into bone and being taken up by osteoclasts, it targets RANKL, a signal involved in osteoclast formation and activity.
That difference matters, but it doesn't make one drug automatically right for everyone. Oncologists choose between them based on the cancer type, kidney function, prior treatment, calcium issues, convenience, and the overall treatment strategy.
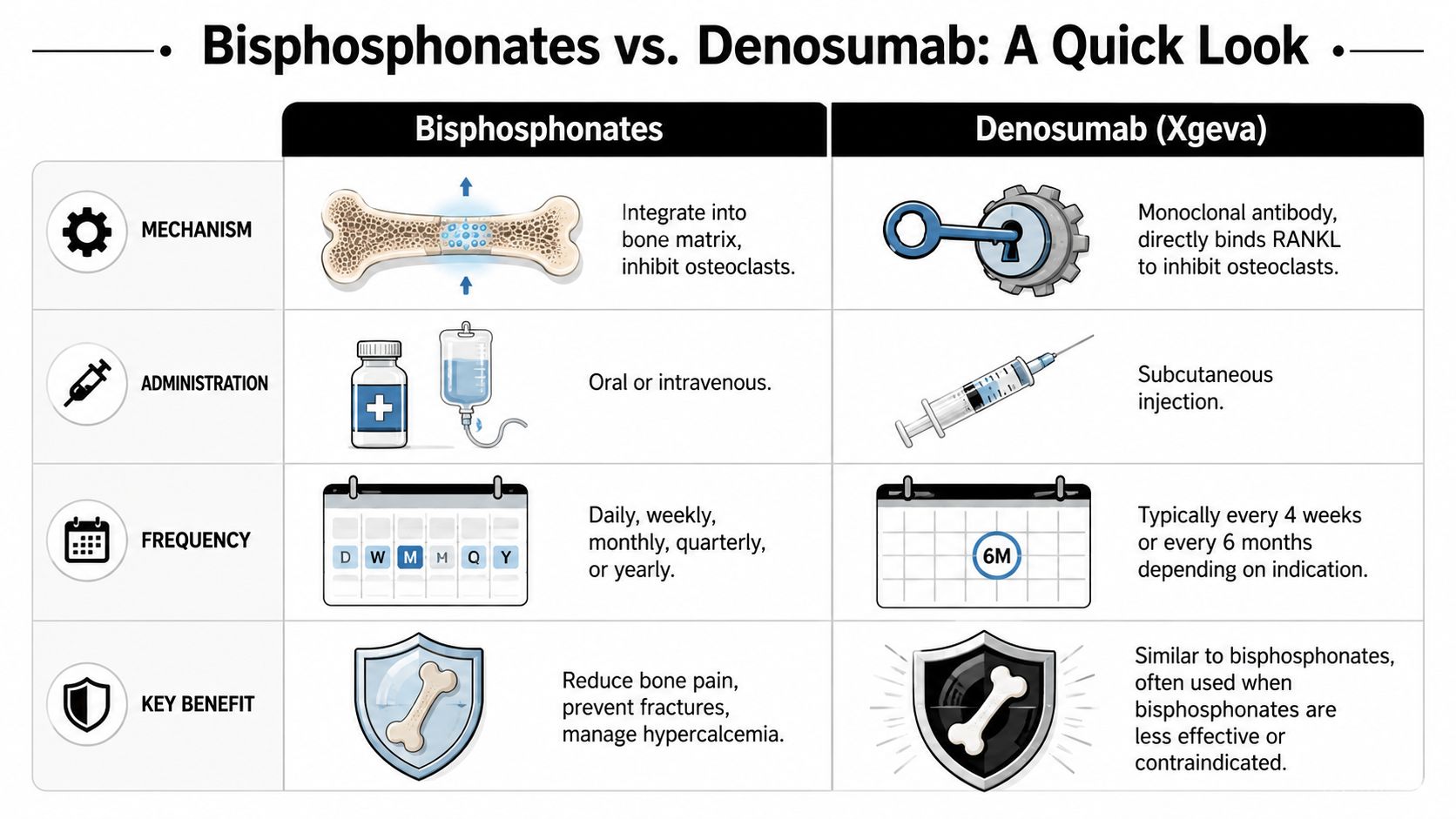
Bisphosphonates vs Denosumab at a Glance
| Feature | Bisphosphonates (e.g., Zoledronic Acid) | Denosumab (Xgeva) |
|---|---|---|
| Basic mechanism | Bind in bone matrix and inhibit osteoclast activity | Binds RANKL and blocks osteoclast signaling |
| How given | Oral or intravenous | Subcutaneous injection |
| Dosing patterns | Can be daily, weekly, monthly, quarterly, or yearly depending on drug and indication | Often given on a repeating injection schedule depending on indication |
| Common role | Bone protection, fracture prevention, hypercalcemia management | Similar bone protection role, often chosen when clinically appropriate |
Rapid answers to common questions
How long does the IV take?
The exact timing depends on the specific drug, infusion center workflow, and whether labs are drawn the same day. Your team can tell you what to expect for your regimen.
How will I feel right after?
Some people feel fine. Some feel tired or achy for a short period. If you've had infusion reactions before, mention that ahead of time.
Is jaw damage common?
It's a real concern, but not something most patients experience. Prevention matters. Dental review before treatment and prompt reporting of mouth or jaw symptoms go a long way.
How long will I need treatment?
That varies. In osteoporosis, some guidance discusses reassessment and possible drug holidays. In advanced cancer, decisions are more individualized and depend on ongoing benefit, tolerance, and the larger oncology plan.
If bisphosphonates don't directly build bone, why do doctors call them bone-strengthening drugs?
Because slowing bone removal can preserve the skeleton and improve bone density over time. The strength comes from protecting bone from excessive breakdown.
What should I do before my first treatment?
Bring a medication list, tell your team about dental issues, ask about labs, and report any swallowing problems, kidney concerns, or new bone pain.
If you're dealing with bone metastases, high calcium, or questions about infusion-based supportive care, Hirschfeld Oncology offers educational resources and oncology treatment information for patients and families navigating advanced cancer.
.png)
.png)




